


Prosthetic contact lenses offer a multifaceted approach to addressing the needs of a wide variety of traumatic eye injuries and blind eyes.
These custom-designed lenses replicate the intricate details of one’s eyes and can be fully customized to the patient’s natural eye color and shape while also providing a realistic appearance and matching the other eye.
Indications for prosthetic contact lenses
Prosthetic contact lenses provide visual rehabilitation and improve visual functioning and quality of life. Today, we have a wide variety of prosthetics that are available to meet the patient’s needs.
Indications for ocular prosthetics include:1-3
- Iris defects: ocular albinism, traumatic iris injury, or congenital iris pathologies
- Corneal opacities
- Color vision deficiency
- Blind eye
- Post-enucleation
The prosthetic lens fitting process
Step 1: Consultation and assessment
Understand the specific needs and preferences of the patient during the initial visit in terms of medical history, degree of photophobia, visual acuity, suitable tints, and lens characteristics for the patient's lifestyle. While fitting patients with ocular albinism, the goal is to reduce symptoms of light sensitivity and vision rehabilitation.
In cases of congenital/traumatic/surgical iris pathology, it is important to achieve a good cosmetic result while addressing visual complaints of photophobia and glare.2
Step 2: Tint selection
There are a variety of different options available for soft prosthetic contact lenses:
- Transparent or enhancement tints: These are translucent lenses that overlap the natural iris and provide an enhancement of the natural eye color.1,2
- Opaque lenses: These are computer-generated printed lenses that allow for reproducibility and offer customizations, such as dark or light underprints (color on the back surface of the lens), pupil occlusion vs. clear pupil, double color application, and limbal rings.1,2,4
- Handprinted lenses: These are fully custom lenses to match the patient’s normal eye.1,2
Step 3: Parameter selection2,4
Lens diameter should be appropriately selected to cover the entire area of ocular pathology. Pupil diameter is another crucial parameter. Normally, leaving a clear pupil with a small diameter can aid in limiting incoming light; however, it can also restrict the peripheral field of vision.
Understanding the occupation and lifestyle can aid in appropriately selecting pupil diameter based on patients’ needs.
Other considerations for prosthetic lenses include:
- Base curve: Depending on the corneal health and irregularity, an appropriate base curve will be required to ensure a good fit and good movement on the eye.
- Lens material: Normally, prosthetic contact lenses use 55% hydrogel lenses.
- Power: In cases of patients that require vision correction, a good manifest refraction is important to determine contact lens power.
Step 4: Trial the lens
Normally, prosthetic lenses do not have trials, so it is important to order a clear soft lens with the appropriate parameters to evaluate the fit of the lens prior to ordering the tints.
Step 5: Follow-up
Assess the lens for comfort, vision, comfort, and symptomatic relief. Educating the patient about proper lens care, hygiene, replacement schedule, and disinfection protocol is crucial for long-term success with contact lenses and to reduce the risk of episodes of microbial keratitis.
Long-term monitoring is important for any future modifications that may be required and in routine management of eye health.
Managing ocular conditions with prosthetic lenses
Ocular albinism
Ocular albinism is a genetic condition that is characterized by a lack of pigment in the eyes—mainly the iris and the retina. It results in reduced visual acuity, impaired depth perception, and photophobia (i.e., sensitivity to light).
Soft prosthetic lenses can play a significant role in enhancing visual comfort and cosmesis and improving quality of life.
Iris occlusion lenses for ocular albinism
Opaque tints such as iris occlusion lenses can provide an excellent benefit of reducing photophobia in addition to providing excellent cosmesis and color match. For patients with ocular albinism, the use of iris occlusion lenses can help alleviate the patient’s symptoms while providing visual rehabilitation.
These opaque lenses have a dark underprint, preferably black backing on the back surface of the lens, with iris pigmentation on the front portion. The black backing offers a great solution for blocking light and reduces the symptoms of glare and photophobia for patients.1,2
A clear pupil in the middle with a small pupil diameter can control the aperture and, hence, the amount of light entering the eye. It provides a great solution for both improving cosmesis and light sensitivity for the patients.
Surgical or congenital iris pathology
Patients with congenital aniridia, iris colobomas, surgical irides, or traumatic iris defects have a lasting impact on their overall quality of life and psychological well-being. While providing visual rehabilitation to patients with the above-mentioned conditions, it is important to understand the cause of the iris defect and tailor the fitting process accordingly.
For patients with traumatic irides or congenital iris defects, color matching to the normal eye is important for a successful cosmetic result. In such cases, the severity of pathology can play an important role in determining which prosthetic soft lens to use.
Of note, both opaque (computer-generated) and hand-painted soft prostheses can help in achieving successful color match options.1-4
Corneal opacities
Patients with corneal opacities or strabismus can become self-conscious of their appearance. In such cases, where the primary goal is masking the opacification, as the eye has minimum vision, the use of soft prosthetics can be ideal for achieving good aesthetic outcomes.
For patients with corneal opacification, the use of an iris occlusion lens with dark underprinting and a black pupil can completely mask the opacification on the corneal surface. Similarly, handprinted lenses can also provide an excellent option and greater customization to match the color of the normal eye.1
Prosthetic lens case presentation
A 4-year-old patient with a Peters anomaly with unilateral corneal opacity on the left eye and incomplete bilateral aniridia presented to the clinic.
The patient was fitted with an iris occlusion lens with black backing and a clear pupil. Subsequently, the patient reported significant improvement in light sensitivity and glare symptoms.
Figures 1 and 2 highlight an example of an iris occlusion lens in a 4-year-old patient with a Peters anomaly.


Figure 1: Courtesy of Manveen Bedi, OD, FAAO, FSLS.

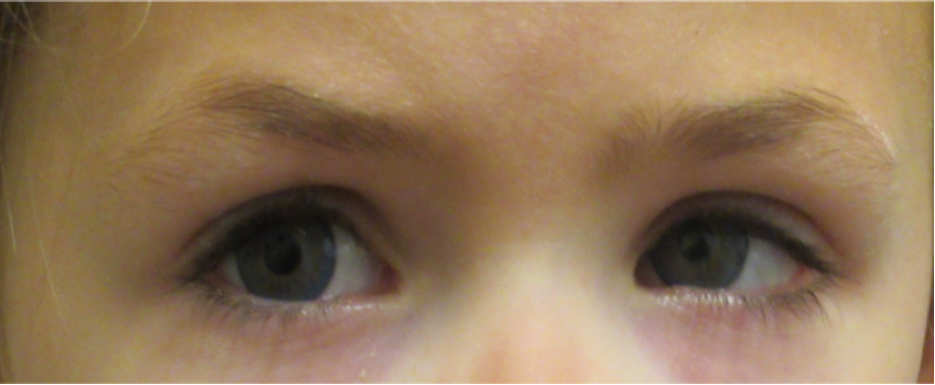
Figure 2: Courtesy of Manveen Bedi, OD, FAAO, FSLS.
Color vision deficiency
Patients with color vision deficiency can also benefit from soft prosthetics in enhancing color perception. The use of a red-tinted lens on one eye can enhance color discrimination for patients with red-green color deficiency. Usually, the red tint is limited to the central 5 to 7mm portion of the lens and is available in varying degrees of hues and color densities.
The red tint of the contact lens effectively acts as a red filter that increases the contrast for the wavelengths of undistinguishable colors, namely red and green. With less color overlap, it makes it easier for the brain to discern the problem colors.5
Fitting a soft prosthetic contact lens
During the fitting process for a soft prosthetic contact lens, firstly, it is important to determine the non-dominant eye, as the lens is applied to the non-seeing eye. Normally, Ishihara plates are used to evaluate the efficacy of the red filter.
While holding different red filters in front of the non-dominant eye, the patient is asked to assess the normally missed Ishihara slides and decide which filter intensity helps make the plate easier to see.
Scleral shells and full prostheses
For patients with atrophy of the globe or enucleation, there are scleral shells, reforms, and full-thickness prostheses. The main difference between a scleral shell and a full prosthetic eye is that the scleral shell is much thinner and is fitted over the surface of the eye.
However, in cases of a full prosthetic eye, it is normally much thicker and is used in cases of enucleation in the patient’s eye socket.
Phthisical/Atrophic eye
Patients with advanced diseases resulting in atrophy of the eye, or in cases of evisceration or microphthalmia, normally present with a smaller eye in comparison to the fellow eye.
The main goals of the scleral shell are to replace the volume deficiency, support the superior eyelid to prevent the narrowing of the vertical fissure, and provide a natural cosmetic appearance.
Enucleation
In cases of enucleation, a full prosthetic eye can improve the appearance of the socket and prevent volume loss of the eye socket. Similar to the scleral shell, this prosthetic device is normally designed by an ocularist to match the other eye.
In some cases, an eyecare professional can fit the scleral shell and finalize the shape and fit of the prosthetic in the clinic with a fitting set and then request hand painting of the prostheses from an ocularist through color swatch matches and high-resolution digital photography.
Pearls for prosthetic lens patient follow-ups
When a patient presents with a scleral shell, it is important to remove the prosthetic device to evaluate the anterior segment/eye socket thoroughly. Dryness and mild discharge on the prosthetic are possible due to mechanical irritation, however, if the patient complains of socket pain, sensitivity, or presence of blood, the eye/socket should be carefully evaluated.
One of the common concerns with a prosthetic is giant papillary conjunctivitis (GPC) due to mechanical irritation. Application of fluorescein can allow for the detection of any signs of conjunctival tissue irritation/staining, and as such, treatment can be initiated.
One tip to provide patients wearing prosthetic devices is to keep the eye/socket lubricated. The use of lubricants such as ointments can be advantageous as it is highly viscous, providing prolonged relief. Additionally, routinely evaluating prostheses is important to rule out any chips or wear and tear on the surface that might abrade the ocular surface.
Prosthetic lens care and maintenance
Similar to the care of gas permeable (GP) lenses, these rigid prosthetic devices require at-home disinfection with a non-abrasive GP lens cleaner. For patients wearing scleral shells, daily cleaning of the shell is recommended unless recommended otherwise.
Routine polishing of the prosthetic is also helpful to remove minor surface scratches on the prosthetic surface and lens deposits and to improve patient comfort. The polishing schedule can vary between 6 months to annually, depending on the condition of the shell and ocular health.
Long-term care and considerations
Long-term management is required to prevent infections and monitor eye health. While dispensing prosthetics, it is important to discuss the need for safety glasses to reduce the risk of vision loss in the good eye in case of an unforeseen accident.
Disinfection protocol should be thoroughly discussed with the patients to ensure they are well aware of the care and handling of the lenses to prevent frequent replacement of these customized devices. Routine monitoring of patients with soft and rigid prosthetics is crucial to overall eye health.
Ongoing advancements in prosthetic lenses
There are ongoing advancements in materials, techniques, and technology used for ocular prosthetics. From utilizing 3D printing for precision to incorporating high-definition imagery for enhanced realism, there are a lot of exciting possibilities to further improve the aesthetics and functionality of both scleral shells and full ocular prosthetics.
Closing thoughts
There is a wide range of options when it comes to prosthetic contact lenses. When managing patients who may require a specialty fit, it is important to understand the goal of the fitting and symptom management that needs to be achieved with the fit.
In addition, setting realistic expectations in terms of fit, maintenance, ocular health, and long-term monitoring is key to ensuring ocular surface health and therapeutic success.

