


Previously, we addressed a number of the obstacles that we must overcome to be successful as practitioners and industry as a whole. In this installment, we’ll discuss some of the keys to ortho-k success.
There have likely been hundreds of articles claiming to have the secrets to fitting ortho-k. Some of them have great information, others don’t. That’s just the nature of the modality. The goal of this article is to familiarize you with some recent ortho-k concepts developed in order to take your lens fitting from basic to a little bit less basic. Expert status can’t be granted to any one at this point. I have yet to have one of the “experts” in the field explain to me why a patient with identical keratometric readings and identical refractions in each eye is only successful in only one of the two identical lenses. But it happens. We can only shake our heads and try our best to adjust lens fit to achieve better treatment. Here are some things to think about to help you along the way.
Treatment Zone Size
Nearly every commercially available lens has an “optical zone” diameter of around 6.0 mm. In orthokeratology, we still call it an optical zone because that’s the convention when referring to GP lenses; however, it’s really the central base curve diameter that provides the treatment. I’ll refer to it as the treatment zone diameter from here on out. Here’s a review of the ortho-k lens anatomy.

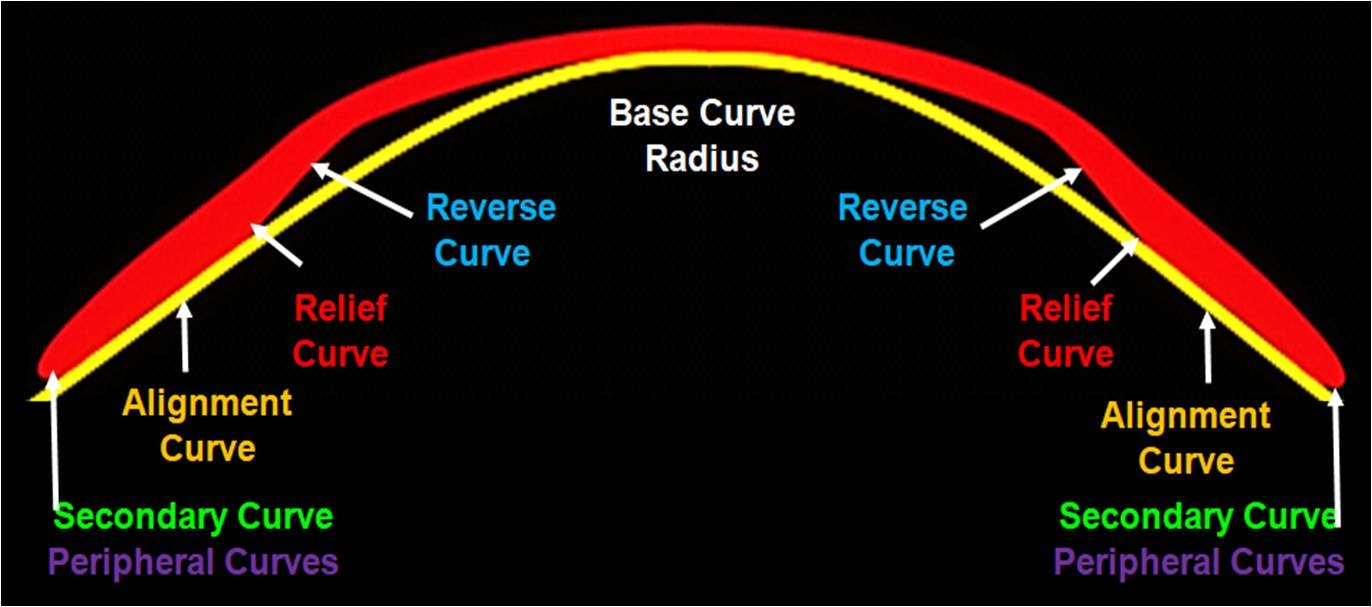
Anatomy of an ortho-k lens
The 6.0 mm treatment diameter is in the goldilocks zone for ortho-k lenses. Any bigger and you end up with inconsistent or incomplete treatments. Any smaller and you end up with more glare and halos. The phenomenon occurs because more light passes through the untreated cornea and enters the pupil. Our hands are a bit tied when it comes to deviating from the normal treatment zone size. However, as our understanding of myopia control increases, that glare and halo associated with smaller optical zones may be advantageous.
The 6.0 mm treatment diameter is in the goldilocks zone for ortho-k lenses. Any bigger and you end up with inconsistent or incomplete treatments. Any smaller and you end up with more glare and halos. The phenomenon occurs because more light passes through the untreated cornea and enters the pupil. Our hands are a bit tied when it comes to deviating from the normal treatment zone size. However, as our understanding of myopia control increases, that glare and halo associated with smaller optical zones may be advantageous.
The 6.0 mm treatment diameter is in the goldilocks zone for ortho-k lenses. Any bigger and you end up with inconsistent or incomplete treatments. Any smaller and you end up with more glare and halos. The phenomenon occurs because more light passes through the untreated cornea and enters the pupil. Our hands are a bit tied when it comes to deviating from the normal treatment zone size. However, as our understanding of myopia control increases, that glare and halo associated with smaller optical zones may be advantageous.
The theory of myopic defocus reducing myopic progression is based on the idea that images “focused” in front of the retina provide a signal for the eye to stop growing. We’ve determined that it doesn’t matter where the defocus falls on the retina, just that there’s enough of it. What we haven’t determined is what is “enough?” Some studies suggest that once a critical amount of defocus is presented, anything exceeding it doesn’t have much of an effect. Others suggest that it’s a dose dependent response and therefore the more the better. The discrepancy doesn’t appear as though it’s going to be resolved anytime soon.
Given the circumstances, it seems to make the most sense to present the eye with as much myopic defocus as possible without reducing the patients acuity or increasing their higher order aberrations to a level that crosses from their unconscious to their conscious mind. That would manifest as excessive glare from lights that might distract a child from learning in the classroom. Decreasing the size of the treatment zone gives you the best shot to reach that “critical” amount of defocus (if it exists) or maximize the myopia controlling stimulus if it is dose dependent. Intuitively, it would then make sense that a smaller treatment zone size would provide more myopic defocus as less of the cornea is being treated. Remember, a fully untreated myopic eye is presented with 100% myopic defocus.
This remains a point of contention as well. Leading experts in the myopia control field argue that treatment zone size of ortho-k lenses have no effect on how well they control myopia. Other’s point to data, unpublished at the moment of writing, that suggest that lenses with smaller treatment zones do a better job of controlling myopia than standard lens designs. The jury is still out.
If you are seriously considering using ortho-k as a myopia controlling modality, you should certainly consider looking into custom lens design software (Wave, OrthoTool, etc.) that allows you to change the treatment zone diameter. Or you can wait a few years until the proprietary smaller treatment zone size lenses become available on the market. Or you can wait until the controversy has more solid evidence one way or another before making a decision, it’s your choice.
Corneal Topography
If you plan to get very serious fitting ortho-k lenses, you’re going to need a topographer. Empirical fitting from a few data points (K’s, Rx, HVID) is very simple, but more difficult to troubleshoot when it doesn’t work. Remember, we are designing lenses that will be making corneal thickness changes as small as 5 microns. With a margin of error so small, wouldn’t you want detailed information about the entire ocular surface before starting the lens design process? That’s the information corneal topography gives you.
We could spend days discussing all the detailed features of all of the commercially available topographers, but we don’t have that kind of time. So instead we’ll highlight some features of corneal topography that help us design better ortho-k lenses.
Visible Iris Diameter
Arguably one of the most important measurements given to us by the topographer is the visible iris diameter (VID). We say visible iris diameter because some topographers do the measurement horizontally (HVID) and some do it diagonally (DVID) which are two different measurements as most corneas are not perfectly spherical and tend be longer horizontally than vertically. However, the difference generally isn’t large enough to warrant a different lens selection. But, some individuals get worked up when you refer to the DVID as the HVID. So we will just say VID.
Regardless of what others tell you, any lens fitting be it ortho-k, soft, GP, or even scleral should start with considering the visible iris diameter because it is a very accurate predictor of the corneal diameter. We choose lens diameters that are a specific distant from the edge of the cornea or limbus depending on what type of lens we are fitting. It’s the same with ortho-k. Larger lenses tend to be more stable. Most of the time, our goal is to maximize the size of the lens without crossing the limbus in any areas. That’s why that measurement is part of the empirical fitting equation.
The nice thing about obtaining the VID measurement from the topographer is the degree of accuracy that you get. That’s important when 0.1 mm differences in VID influence our lens selection. When compared to handheld HVID rulers, corneal topography is more repeatable and accurate.
Composite Mapping
The central 3 mm of the cornea might just be the least important area of the cornea when it comes to fitting not only ortho-k lenses but all contacts. Coincidentally, that is where keratometric readings are taken. That said, in normal eyes, you can often extrapolate information to get a pretty a good idea of the shape and curvature of the rest of the cornea. But wouldn’t you rather know exactly what it is? That’s where composite corneal topography comes in. Creating a composite topography (stitching together topographical images taken in primary, up, down, left, and right gaze by the patent) ensures that the peripheral cornea is properly measured. It just so happens that the peripheral cornea is the most important area when fitting a corneal lens because that is the area on which the contact lens will land. Remember, an ortho-k lens doesn’t actually touch the cornea anywhere except the alignment zone. So where is that? For most ortho-k lenses, the lens will land 3.5 to 4 mm from the apex of the cornea or peripheral cornea.
Knowing this information 360 degrees around the cornea helps immensely when designing the alignment curve of ortho-k lenses. Unfortunately, you don’t always get accurate information that far out when you capture a single image with the topographer. The topography software is able to align similar points from the 5 images it takes when creating the composite. That means nearly every corneal point is measured at least twice during the stitching process. It is more accurate and precise than just using a single map. And precision is key when design ortho-k lenses.
Corneal Height Differential
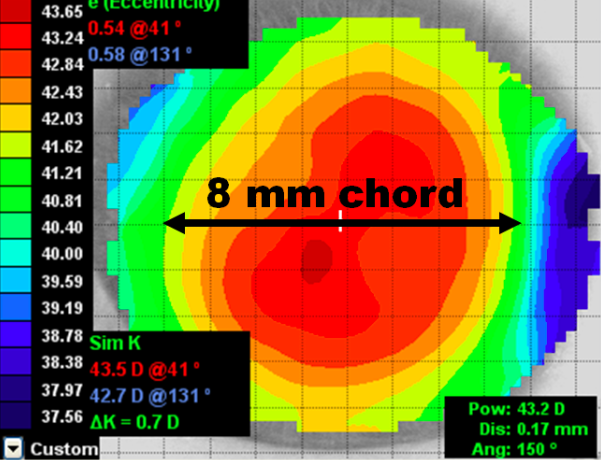
One of the key pieces we get from a quality composite topography is the corneal height differential. It is defined by the difference in mean elevation of the steep and flat meridian. By convention, we usually measure it at a chord of 8 mm.

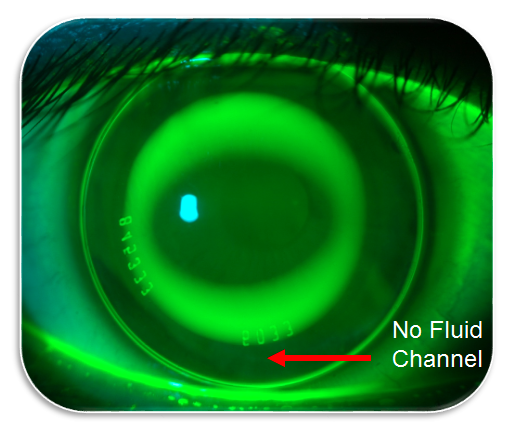
Think about it this way, because the steep meridian is more aggressively curved, it tends to be lower in elevation that the flat meridian. If you put a lens with a spherical alignment curve on an eye with a large height differential, the lens will first land on the flat meridian because it is the often the highest point. The lens will then “float’ above the cornea in the steep meridian because that area is lower relative the flat meridian. In a with the rule cornea, this will manifest as a fluid channel at 12 and 6 where fluorescein can pool as seen below.

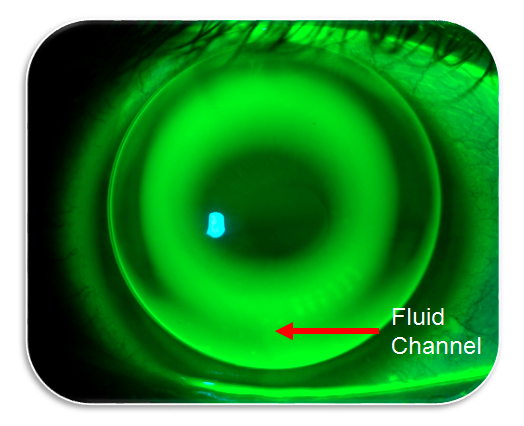
The fluid channel opens the reserve curve reservoir and eliminates the hydraulic forces that provide the treatment effect in ortho-k. In order to prevent this, we can make the alignment curve toric to match the toricity (height differential) of the cornea. The steep meridian of the toric alignment curve of the lens lands on steep meridian of the cornea creating a “closed” fluid reservoir underneath the lens. No fluid channels exist as seen in the image below.

Implementing the toric peripheries on ortho-k lenses has dramatically increased our fitting success.
An extremely important point is that the dioptric value of corneal cylinder has no predictive value of height differential of that same cornea at a chord of 8mm. For example, you may have a patient that has K values of 43.00/44.00. Their height differential at an 8 mm chord could be 0 or it could be 50 microns. The only way to determine whether or not a toric ortho-k lens is indicated is to measure it with the topographer. We choose to use toric peripheries when the corneal height differential is 30 microns or greater.
Even if you only use a few features, you can take your ortho-k fitting to the next level using a corneal topographer. The more often you are successful with the first set of lenses, the less time and money you have to spend on follow ups and remakes. You can see how the relatively small price tag (new topographers can be purchased for less than $15,000) can make a huge impact when you’re able collect a substantial fitting fee ( average $1,200) and not remake lenses.
Clear Communication
Technical tidbits aside, the biggest key to ortho-k fitting is still communication. It feels a bit like beating a dead horse to discuss communication again at this point, but it bears repeating. There is a knowledge barrier here in North America that must be overcome to be successful with ortho-k. Most people have never even heard of ortho-k. Imagine how much more difficult we would perceive prescribing glasses to be if a patient had never seen a pair of specs before. We would look pretty silly trying to explain that this goofy contraption that sits on your face can help you see better. That’s a little bit like explaining what ortho-k is. Here’s some simple steps in the education process.
Highlighting the positives
The biggest advantage of ortho-k is convenience. This is especially true for children. Mom and dad don’t have to worry about sending their kids off to school with glasses or contacts that can get broken or torn. It often gives them a sense of security that their son or daughter will have clear sight all day long without any hassle, especially if they are active in sports or other activities.
The second biggest advantage is arguably the myopia controlling effect. Again, ortho-k is not officially approved for myopia control by the FDA, but that doesn’t mean you can’t educate patients and parents on the current literature. Additionally, that literature brings up an interesting ethical point. Considering all that we know about myopia progression and control strategies, one could argue that putting children in to a single vision spectacle lens is borderline unethical, especially if you don’t present other vision correction options that are proven to slow the rate of progression compared to single vision glasses. So if you have any hang ups about “selling” ortho-k, stop looking at it is selling. Present the patient with the options and information and let them decide.
Acknowledge downsides and unknowns
If you try to skirt past the disadvantages that come with ortho-k you will gain an instant “used car salesman” vibe. It is imperative patients have all the information about ortho-k. Good and bad. If you acknowledge that the lenses are uncomfortable on the first few nights of wear and that patients may experience some glare and halos in low light conditions, you save yourself from a surprise angry phone call about how the lenses aren’t working.
The other issue that always comes up is price. Ortho-k lenses aren’t cheap. If you completely avoid talking about price, you’re going to lose patients. But, it’s not something to start the conversation with either. If you are able to communicate that cost is set due to the relatively high complexity of lens design, number of office visits, and knowledge required to properly fit ortho-k lenses, patients will have a better understanding of the pricing. Another thing to consider is that we often see patients who have worn the same lenses for 3 to 4 years. Obviously, patients must be very careful with their lenses in order to make them last that long, but that’s a significant cost saved in spectacle expenses if your patient is progressing in myopia -0.75 D. a year. Ortho-k lenses can actually be cost effective compared to spectacles and soft lenses over a 2 to 3 year period. The downside is that costs are often out of pocket for ortho-k lenses. But, ortho-k really isn’t as pricey as it may appear from the outside.
Conclusion
We have barely scratched the surface of ortho-k. We’ve discussed a little about the myths, the obstacles, and best practices. There is so much more for us to learn about the modality and the rate of learning is accelerated when more doctors are fitting lenses. By 2050, there will be 45 million myopes in the US, many of them children and young adults. That’s a lot of opportunity. And not a single one of those patients will be getting their ortho-k lenses from online retailers. You can’t say that about soft lenses or glasses. Financials aside, offering ortho-k and other myopia control techniques is truly in the best interest of our young patients. You can choose to acknowledge that now or later. The first step in becoming an ortho-k fitter is personally buying in. You will never be successful if you don’t believe in it. Many manufacturers will comp you lenses if you want to try it yourself or on a staff member. The effect is powerful. With a little practice, you’ll have another tool in your toolbox as you grow into an outstanding clinician.
