



Case Study: AMD Management with Progression to Geographic Atrophy
Presented by Jessica Haynes, OD
Case history
The patient was a 70-year-old white female who presented to clinic for an age-related macular degeneration (AMD) presentation. Her first evaluation was in 2012, when she was seen by a colleague of mine while I was a second-year optometry student. In her 2012 appointment this patient had 20/20 best corrected vision in both eyes, with essentially no visual complaints at that time. She was a very healthy patient, wore sunglasses, focused on her health and diet, exercised, took AREDS-recommended vitamins, and was using her Amsler Grid to detect problems in her central visual field.
2012 imaging
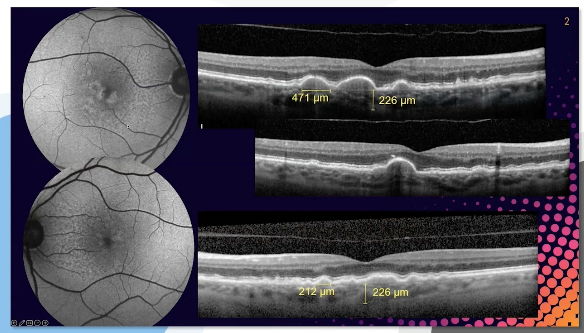
On the right you can see a few representative OCT cross-section scans, and on the left are her fundus autofluorescence (FAS) images. What stands out on her OCT scans are her drusen. In this case, the patient has some very large-size drusen pigment epithelial detachments (PED) (because they are over 125 μm in size), which can be visualized in the hyperreflective band through the retinal pigment epithelium (RPE). The patient also has subretinal deposits—aka reticular pseudo drusen—which show up on FAS, but at this point, no other signs of geographic atrophy. And it should be noted she is focused on AREDS recommendations as well as not smoking, adhering to dietary modifications, and avoiding UV light.
Risk:
Size of the drusen and pigment showcase risk towards executive AMD (wet AMD), with a risk of about 50% at five years, which is not trivial. Typically, it’s common for large drusenoid pigment epithelial detachments to collapse, and one of the prognostic indicators is the hyperreflective foci, which may be the first spot to collapse. Pseudo drusen, in particular. have a high risk of developing advanced AMD as well as geographic atrophy (GA). At this point, the patient has intermediate AMD that is at higher risk for developing advanced AMD and geographic atrophy.

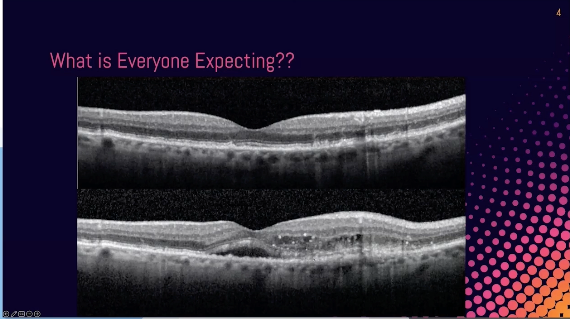
Case presentation: 2021 visit
Now the patient is 79 years old and is referred back to the clinic with sudden changes to vision in her right eye. Her right eye is now 20/80 while her left eye remains 20/20. She has positive metamorphopsia on her Amsler Grid and notices that her vision is worsening in her right eye because she is having difficulty with reading and driving at night. She is still a healthy, active patient, but now her vision is interfering with her lifestyle.

As a clinician we are witnessing her drusen deposits transform into choroidal neovascularization. So while the drusen loads collapse, the patient is likely developing geographic atrophy as seen by fewer drusen but with more hyper-reflective columns. And if you look at the fundus autofluorescence, the hypo-autofluorescence images are all geographic atrophy. Again, any drusen over 125µ is considered large-scale drusen.
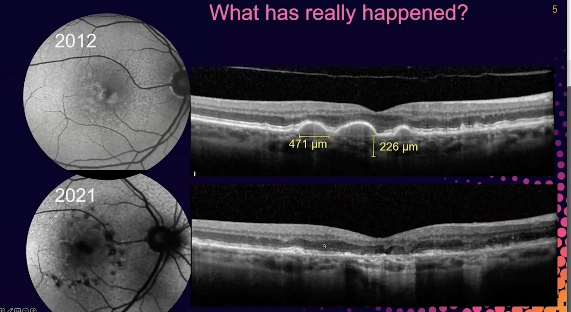
What really happened?
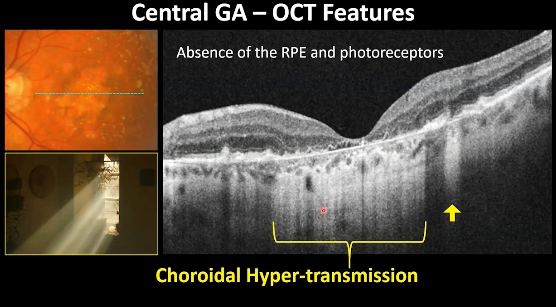
What's happening is the patient is developing geographic atrophy. So we have fewer drusen, but what we have instead are these hyper reflective columns. So light is cascading through the retinal pigment epithelium into the choroid. You see how bright it is here versus less bright here because the RPE is blocking the light here. We also have in this area loss of our outer retina bands—in particular the retinal pigment, epithelium, photoreceptor integrity line, and external limiting membrane.
But if you look in this photo, those are absent. So this is a patient who's developing geographic atrophy or who has developed geographic atrophy. If you look at the fundus autofluorescence, these hypo-autofluorescent lesions are all geographic atrophy.

What is the approach?
This is a patient who might benefit from complement inhibition therapies—and this might be a good point where this patient can be referred to retinal specialists. The left eye is more critical in terms of treatment because there is more vision to save. And it’s really important to mention that in terms of complement inhibition, there are two FDA-approved drugs that are designed to slow the progression of geographic atrophy. At this point, it’s important to determine the benefit of complement inhibition therapies compared to the risk. However, this patient case occurred in 2021, without the benefit of today’s therapies. The 2023 imaging shows how quickly disease progression occurs.
Case Study: AMD Management: The Warning Signs to Recognize, Diagnose, and Refer GA
Presented by Carolyn Majcher, OD, FAAO
Case presentation
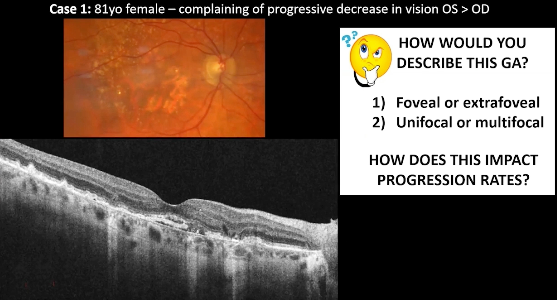
The patient is an 81-year-old female who is complaining of progressive disease in vision in the right eye and even more in the left eye. She correspondingly has reduced visual acuity commensurate to that complaint. Her vision in the left eye is reduced to 20/100 and her vision in the right eye is reduced to 20/40.

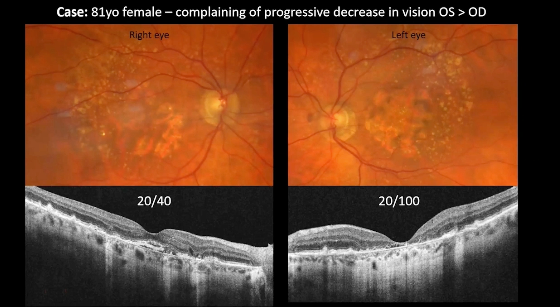
At first, just looking at her color fundus photographs in both eyes, geographic atrophy is obvious. There are well-demarcated regions of hypopigmentation or retinal pigmented epithelium (RPE) loss, typically revealing large underlying choroidal blood vessels as well.
With regards to her OCT findings, I want to start with the left eye first, which displays severe RPE loss at the center of the fovea.

In terms of the right eye, geographic atrophy doesn’t seem to be affecting the fovea yet, although fundus autofluorescence shows a fairly large lesion with multiple foci of disease, which is an indicator of progression.
And the fact that it's bilateral as well puts it at a higher progression rate compared to a unilateral lesion. So just based on the presentation thus far, we know that the progression rate for the size is probably going to be faster than compared to perhaps other phenotypes of geographic atrophy.

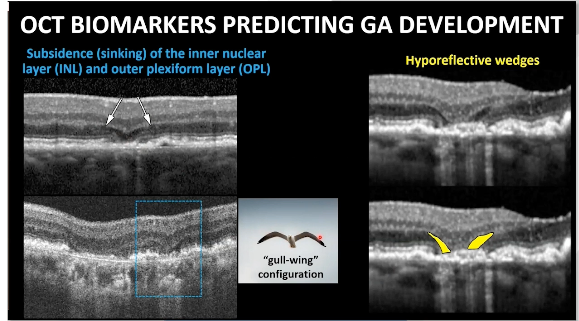
Let’s point out some of the specific OCT features that are associated with early geographic atrophy formation, many of which are high risk biomarkers for future geographic atrophy development or expansion.
The first are hyporeflective wedges, which are the dark triangles where the base rests on the surface of the RPE. They typically border areas of geographic atrophy. The second is the sinking of the outer layer where it’s sort of V-shaped and dropping down into that area of photoreceptor loss.
The next are the subretinal drusen deposits—or reticular pseudo drusen—that are a risk factor for geographic atrophy and advanced AMD, in general. You can also see a unique hyper-reflective crystalline deposit, or sub-RPE plaques, as they are sometimes referred to. This is that hyper-reflective linear line usually associated in the subretinal or sub-RPE space that corresponds to shiny drusen—that is also a risk factor for geographic atrophy.
Overall, OCT images on cross-sections can provide much more clarity in terms of understanding geographic atrophy than fundus photos can.
Risk factors of geographic atrophy to look for
Signs that you should watch closely for geographic atrophy or refer out for consideration of complement therapy:
- Hyper-reflective wedges in a pair on either side of potential geographic atrophy
- Early lesions
- Sinking of subsidence of the outer plexiform layer that tends of form a seagull-wing configuration
- Declining visual function (although many patients with geographic atrophy haven’t had visual decline yet)

The diverse nature of geographic atrophy
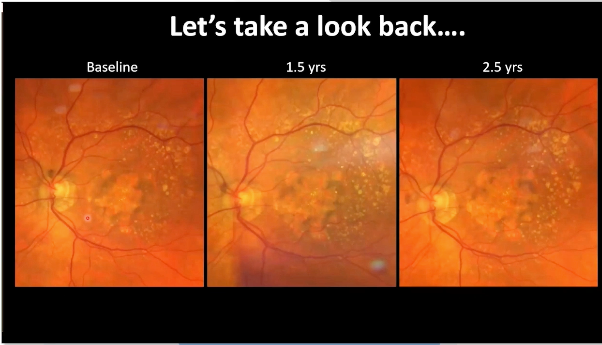
This case really brings home the diverse, unique nature of GA, even in the same individual. If you look at both eyes, when we first saw this patient, her baseline exam is on the left while her most recent is on the right. Even early on in the course of disease in the left eye, she started out central, versus the left eye, which went extra foveal. While we have one patient, each eye is affected very differently, has different patterns, and a unique progression rate.

An interesting thought when treating patients who are already center-involving is that even though the visual acuity may not change as they progress, the size of the scotoma—or blind spot—increases over time, which will eventually lead to a vision decline.
Additionally, this also highlights the shortcomings of fundus photos compared to OCT images on the cross-section. The near-infrared reflectance that accompanies the OCT image can provide a lot of clarity into understanding the progression of geographic atrophy. Color fundus photography alone won’t get you a good story of geographic atrophy. Finally, you can’t use visual acuity as a measure of geographic atrophy as visual acuity only pinpoints the moment in time when the atrophy moves from “foveal” to “central foveal” and directly impacts vision. They may have the same visual acuity they started with, but their visual function may be on the decline.
A better way of looking at GA over time

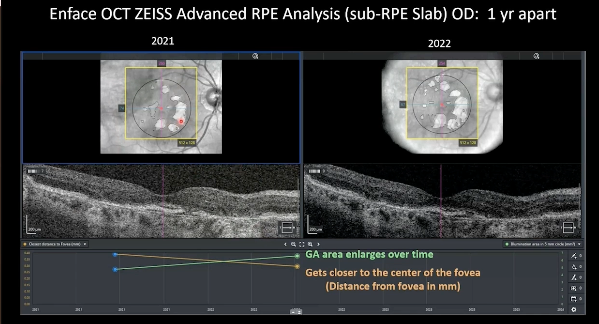
In these photos, OCT analysis —specifically looking at the RPE analysis—what we are looking at is a sub-RPE slab of two D-data just underneath the RPE and mapping our areas of choroidal hyper-transmission. Fundus photos alone are not enough to measure GA progression. What’s really nice is that just looking, you can see it’s enlarged over the course of just one year with two OCTs, but the quantitative data tells us that there has been a trend of GA over time. There is also a trend with the orange line that has been getting closer and closer to the center of the fovea and threatening good vision.
Take-home messages
- Be familiar with color photography and OCT features of geographic atrophy
- Visual acuity often remains stable while extra-foveal GA expands and comes closer to the center of the fovea (VA is a poor indicator of GA expansion)
- Once GA is central, VA is severely and irreversibly affected
- OCT enface imaging is superior to color photography to monitor GA progression
- Multifocal extrafoveal GA tends to have a fast progression rate
- Patient is likely highly motivated to treat OD
