



Ocular Disease Case Study Week—created in partnership with ZEISS Professional Education—brought together optometrists across the globe to increase disease knowledge through the sharing of unique case studies, diagnostic scans, and workflow protocols.
After sharing the top four cases on the @eyesoneyecare.optometry channel from December 5th-9th, 2022, followers voted on their top picks.
Below is the second-place case study. Keep reading to see what made Cassondra Lux-O'Callaghan, OD, stand out.
Second place: Cassondra Lux-O’Callaghan, OD
Case Study: Corneal melt secondary to herpes viral keratitis
Patient:
A 62-year old African female presented with her translator as a referral for a recurrent corneal erosion, left eye, on November 3, 2022. The patient had been seen on and off for corneal ulcers since 2015 at our clinic and through a corneal specialist elsewhere. Her vision in the past was hand motion and was stable.
Exam:
During the exam, the patient presented with an almost 360-degree epithelial defect, diffuse edema, dense central corneal scarring with neovascularization, central thinning approximately 30%, and 1 mm inferior hypopyon. She was Seidel negative. She was started on oral Valacyclovir 1g TID, Vitamin C 500 mg BID, and Doxycycline 100 mg QD, Moxifloxacin one drop eight times daily, and Bacitracin ointment qpm.
Diagnosis:
She was diagnosed with herpes viral keratitis (B00.42), corneal ulcer with hypopyon, left eye (H16.032), and neurotrophic keratoconjunctivitis, left eye (H16.232). The patient was monitored closely due to the epithelial defect and hypopyon, and for potential perforation.
10-day follow-up:
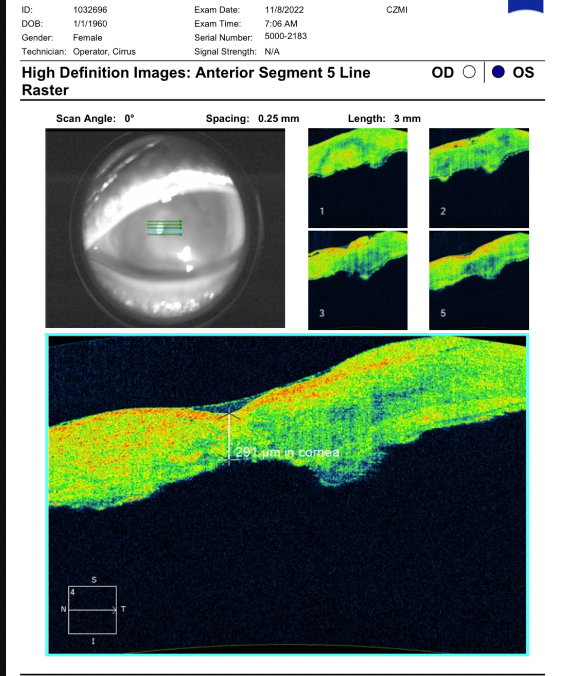
After 10 days, the epithelial defect and hypopyon had mostly resolved, and there were no signs of perforation. An anterior segment 5-line raster was performed to measure the amount of corneal thickness present over the thinnest area of the cornea.

Three-week follow-up:
At the three-week follow-up, the patient presented to another doctor in the office and was Seidel positive. Dermabond/glue was attempted to be located to stabilize the cornea, but none was found. A bandage contact lens was placed and the patient was referred to a medical center in another city for possible same day surgery.
Discussion and conclusion:
After review of past records and patient history, we determined the patient originally presented to our office from a primary care doctor’s referral for a corneal abrasion in 2015. She was diagnosed with an infectious corneal ulcer at that time and prescribed fortified vancomycin and tobramycin q1h while awake. The patient was followed daily for one week with little improvement and referred to a local corneal specialist where she was diagnosed with corneal melt secondary to herpes viral keratitis and started on Valtrex.
She continued to be monitored there and was eventually lost to care in 2017 until she presented again to our office. Corneal stromal disease from the herpes virus can present with recurrent infections, can lead to corneal thinning, and eventually, corneal melt. This patient has a history of corneal disease. With the onset of a hypopyon, a large epithelial defect, and corneal thinning, close care was warranted. Due to perforation presenting at the last follow-up, the patient needed further care and treatment with possible surgical intervention.
As an observation, cultural and language barriers make it difficult to provide care when you cannot educate patients directly. It is also difficult when patients need surgical intervention earlier in the disease process but are financially limited. Hopefully, we will be able to surgically intervene at this time to help the patient, limit their recurrences, and prevent worsening disease.
