



Technology you need to diagnose and manage glaucoma
If you want to get started in the management of glaucoma, you have to have some of the basic tools.
- Goldmann tonometer to measure IOP
- Gonio lens to check whether the drainage angle is open or closed and to identify abnormal blood vessels
- 90 diopter lens to check the fundus
Then we get into the more high-tech options. Most optometrists have an optical coherence tomography (OCT) machine to generate a picture of the back of the eye, as well as some sort of visual field testing. Then we get into measuring corneal thickness with a pachymeter as well as the fundus camera to show the retina, retinal vasculature, optic disc, and macula.
Newer technologies include an optical coherence tomography angiography (OCT-A) to image the microvasculature of the retina and choroid, as well as measuring corneal hysteresis, which reflects the ability of the cornea to absorb and dissipate energy,1 and can determine the pressure in the eye.
You need to have diagnostic equipment to get started. In my practice, we use multiple ZEISS diagnostic instruments, including the OCT, Humphrey Field Analyzer, the CLARUS fundus camera, and we also have a pachymeter to measure corneal thickness.
After I’ve diagnosed a patient with primary open angle glaucoma, I like to discuss treatment options with them. Our first-line treatment is typically an SLT. I also like to talk about new advancements in treatment options, such as the Durysta® dissolvable implant to help reduce ocular hypertension. In terms of topical medications, I typically prescribe a preservative-free prostaglandin to help decrease the benzalkonium chloride (BAK) load on the surface.
An integrated ZEISS workflow for diagnosing and managing glaucoma
It’s important to have a workflow to diagnose and manage glaucoma. In my practice, my follow-up schedule for newly diagnosed glaucoma patients is slightly different from patients that we’ve managed for many years, and who are stable.
My routine for stable and managed patients
We typically see stable patients every four months. We will alternate between a dilation with an OCT or disc photos. On the next visit we will do a visual field test — usually a SITA Faster visual field test to improve the efficiency. Four months later, we will do a gonioscopy to check their angles. During each of those visits we will also perform a tonometry to check their pressures.
My workflow for newly diagnosed patients that includes risk factors
I always start with a case history and review the risk factors associated with glaucoma, such as high myopia. Then I will perform a very thorough examination using a slit lamp to check their optic nerve and their IOP. If my technician knows that this is a potential glaucoma suspect, he or she will perform a perimetry screening. After I’ve confirmed a diagnosis of glaucoma or glaucoma suspicion, then I will order additional testing.
Some tests I order include:
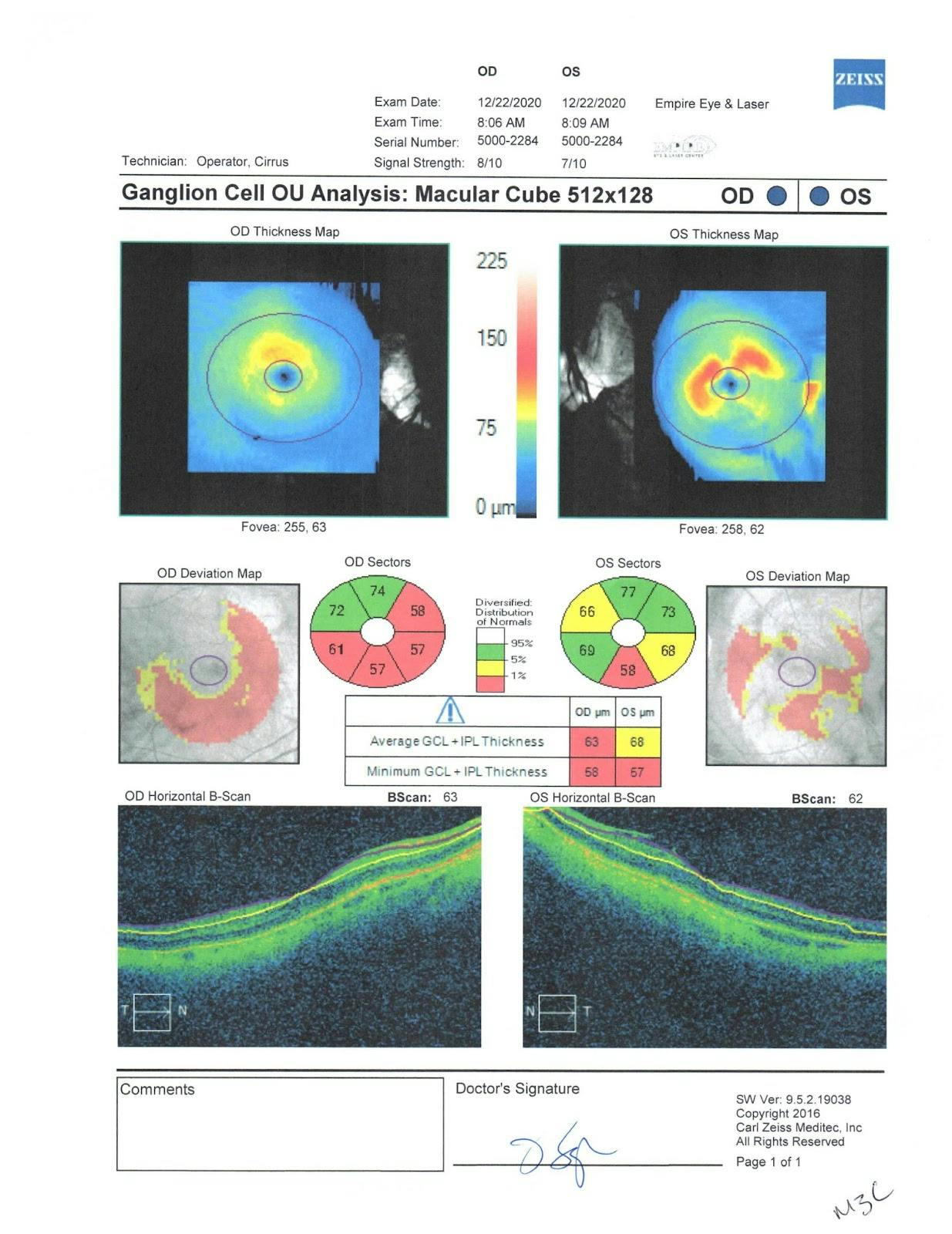
- OCT with a ganglion cell analysis
- 24-2 SITA Faster visual field test
- Stereoscopic optic disc photos using our CLARUS fundus camera
After I get printouts from the OCT and visual field analyzer, I review that information with my patients in the exam room during their appointment time. Later in the day, we will upload that information into our electronic medical records system, which will allow me to review that information for future and past visits.
Practice tips to enhance your glaucoma workflows
- In my practice, I have an electronic medical records system that allows us to upload OCT scans and visual field results directly into our system. This means I can review that information with our patients in the exam lanes. It’s powerful because even if they are experiencing no symptoms, they can see the damage.
- I like to keep the visual field test in its own room. This eliminates patients becoming distracted when there are other patients near them. Reliability is extremely important in the management of glaucoma, so a quiet, calm space to conduct visual field testing is essential.
Case study of 46-year old male glaucoma suspect
Case history
I was referred a 46-year old Hispanic male by one of the local optometrists for a second opinion. His optometrist suspected he might have glaucoma and suggested I see him for a second opinion. He had already been given a sample of Travatan Z to get started on lowering his pressure. The patient did have a history of LASIK back in the late 1990’s.
- 46 year old hispanic male
- Referred for second opinion
- Glaucoma suspect, given sample of Travatan
History of LASIK in 90s
OCT exam
During his glaucoma evaluation, we performed pachymetry. His right eye was 460 and his left eye was 463 - we suspected his corneas were thinner than average due to history of LASIK. His entering IOPs onTravatan Z was 14mmHg in the right eye and 16mmHg in the left eye.
When I evaluated him using the slit lamp and my 90-diopter fundus lens, I noticed an enlarged cup to disc ratio in the left eye, greater than the right eye, with a 0.85 on the left and an 0.70 on the right.
Baseline fundus photos were taken.

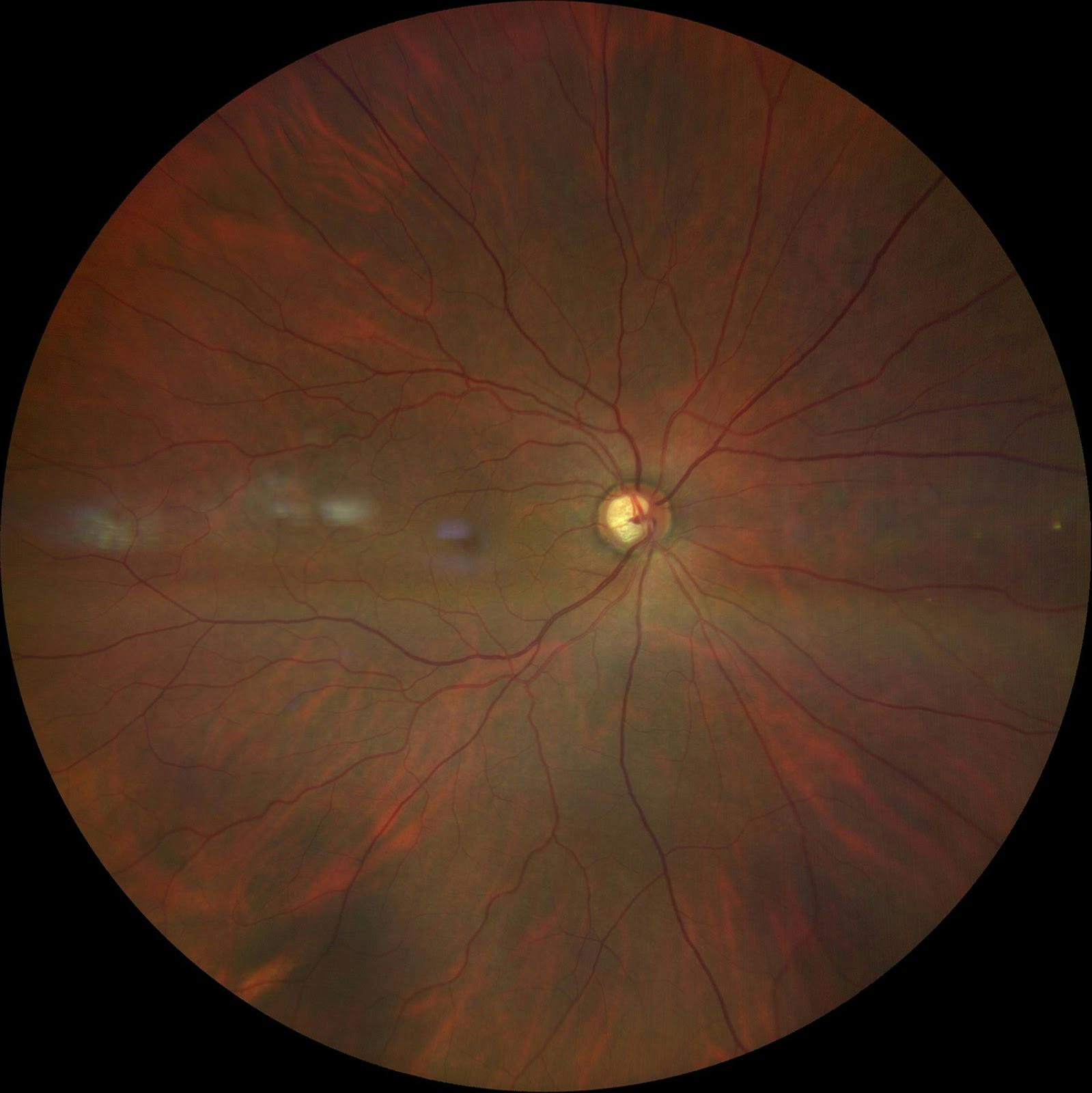
Fundus photo: OD
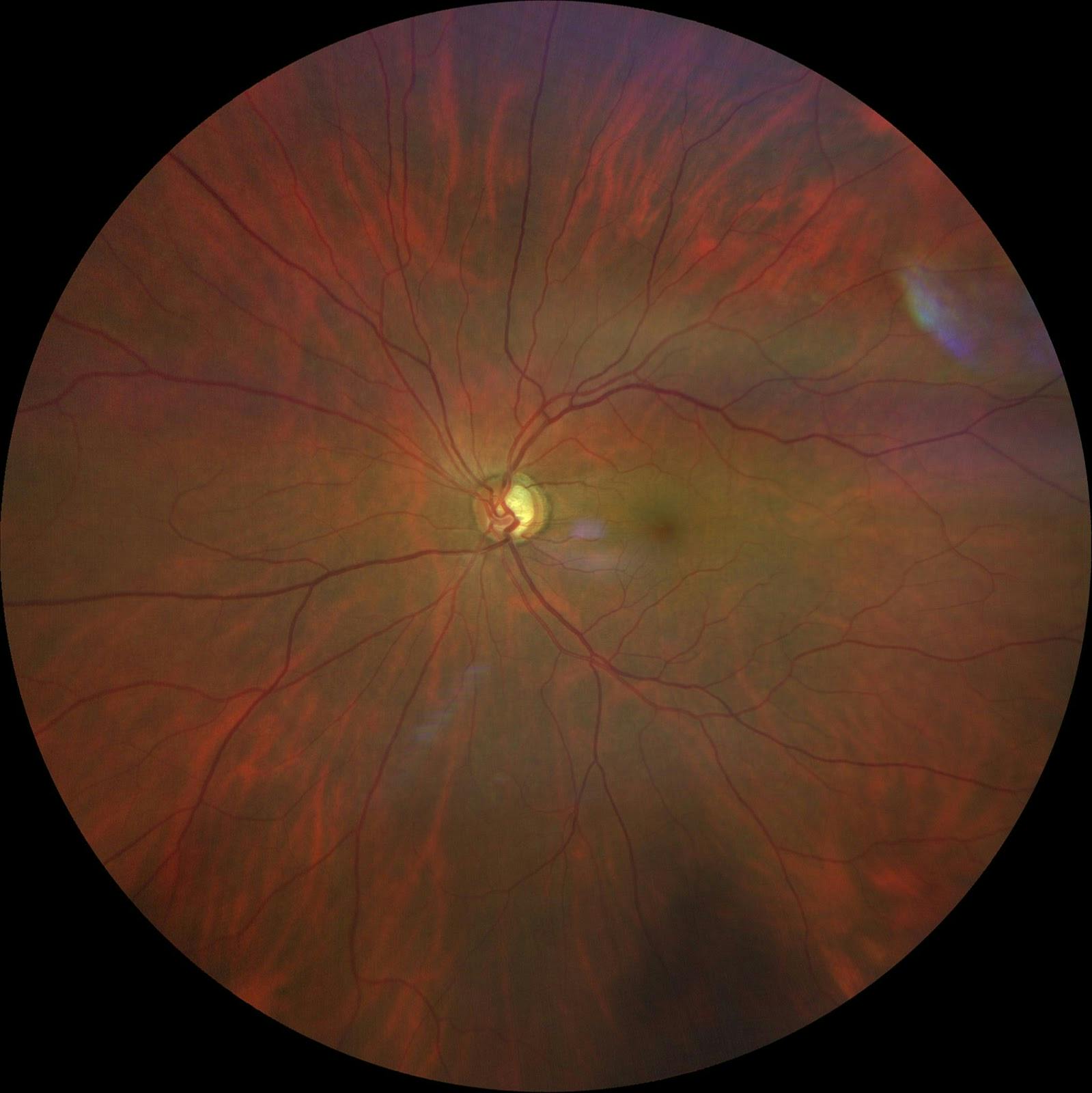
Fundus Photo: OS
We also performed an OCT analysis of the optic nerve, which confirmed my clinical examination that he had some nerve fiber loss inferiorly in the left eye while his right eye was perfectly healthy. At that time, I agreed with the referring optometrists that this patient was a high-risk glaucoma suspect for primary open angle glaucoma, and I made a follow up appointment for the patient to come back for a 24-2 visual field test within a month at which point, we kept him on Travatan.
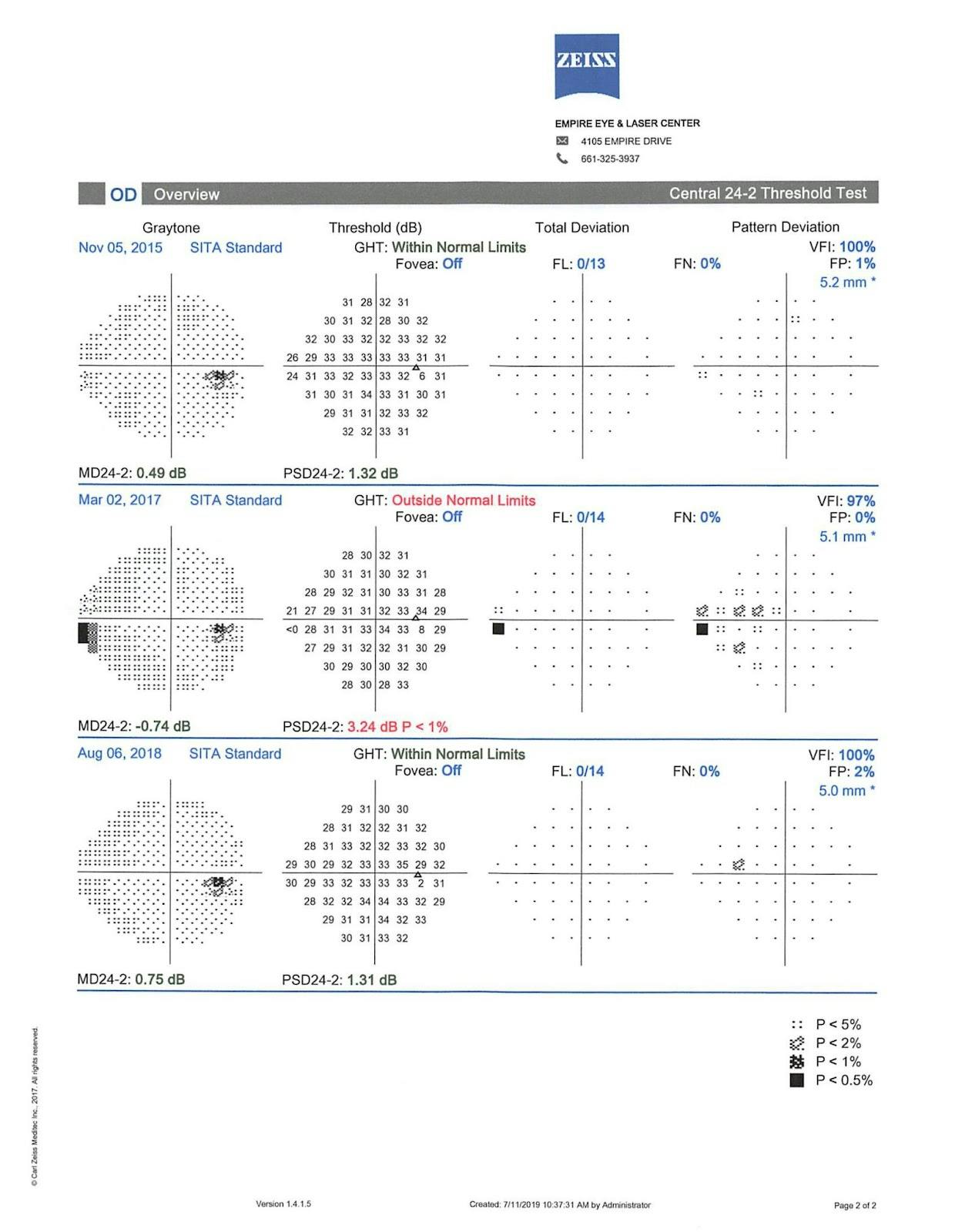
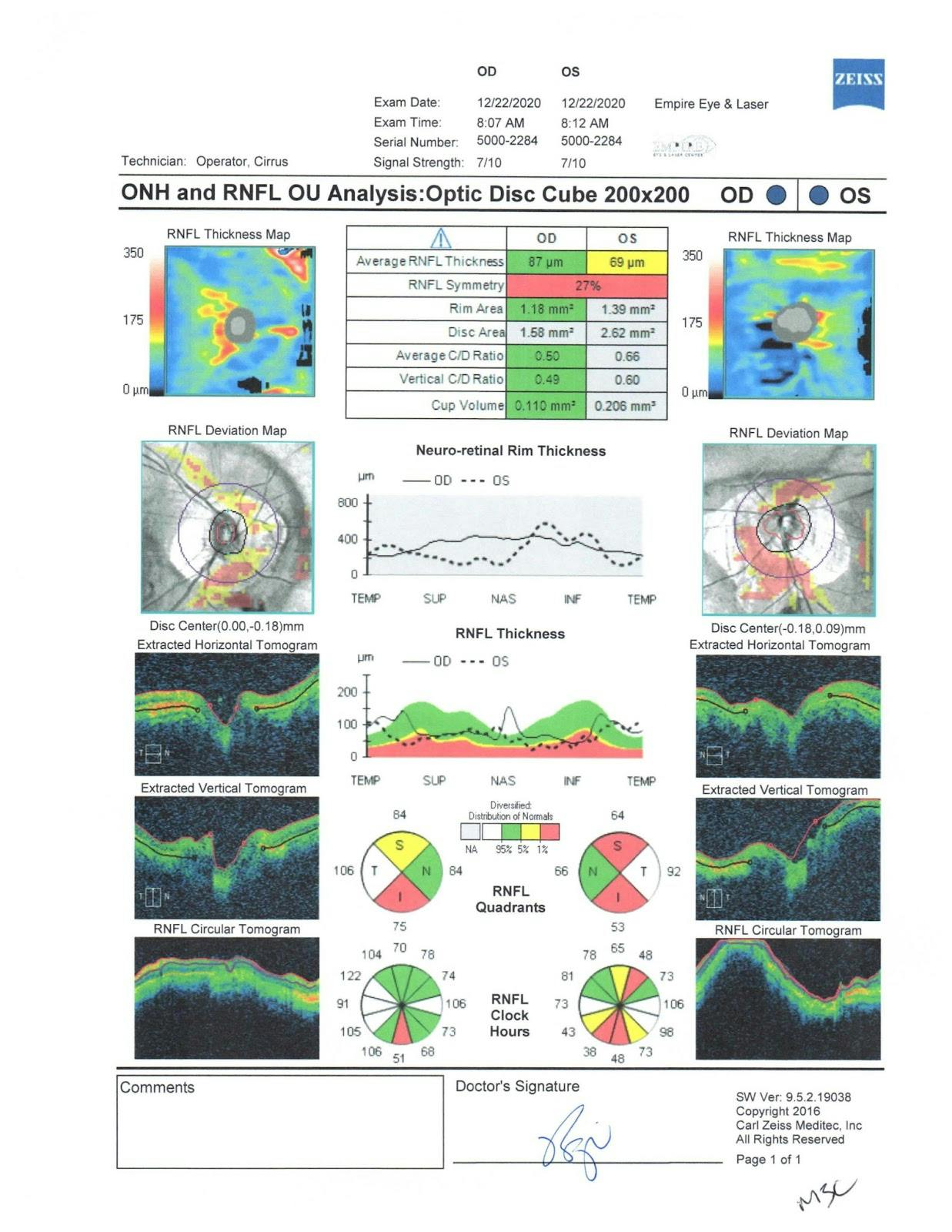
In 2019, after being treated with Travatan Z for 4 years, we noticed some progression on his optic nerve head during an OCT exam.

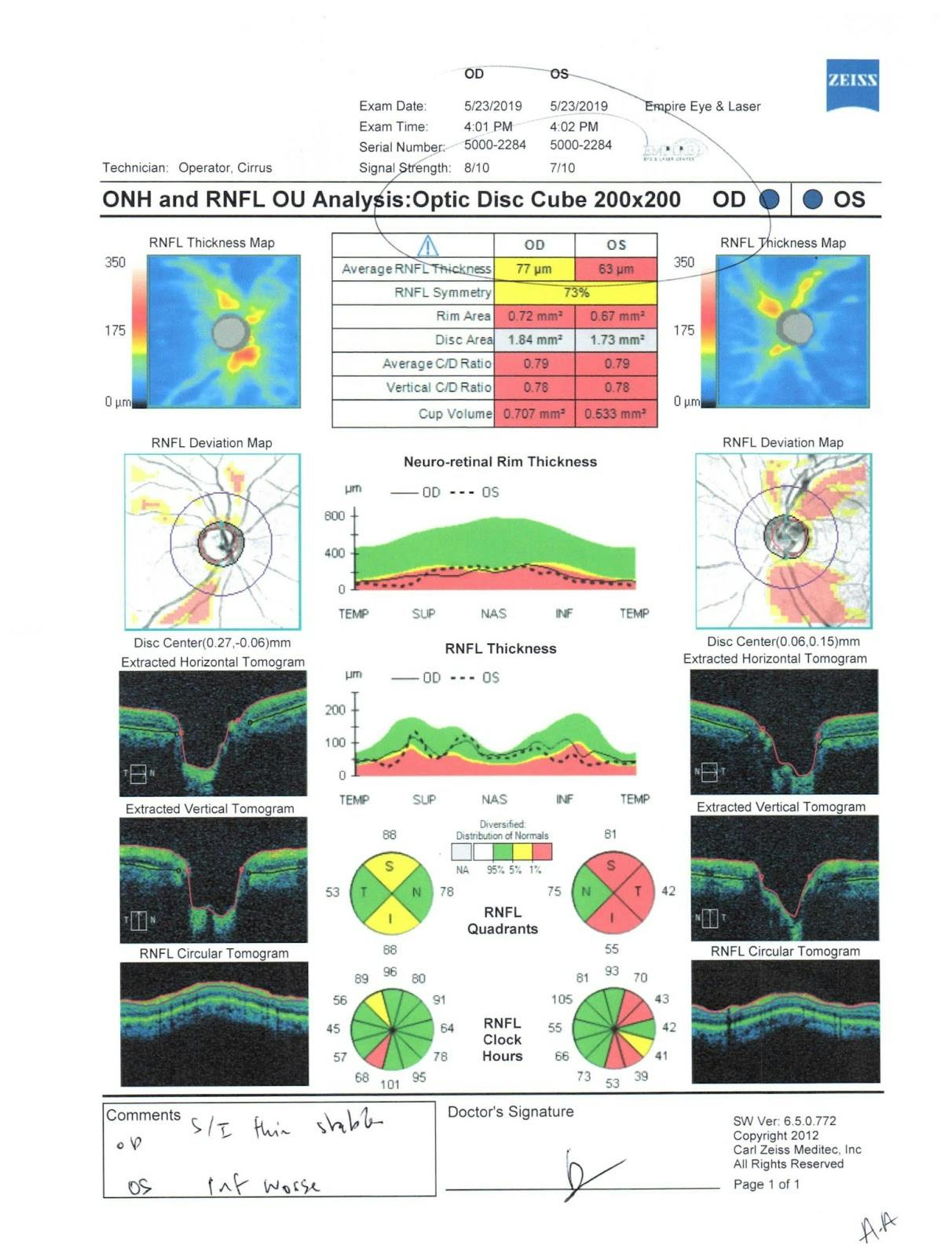
OCT RNFL
Visual field test
When the patient returned for his visual field test, we were following COVID-19 protocols and had recently switched over from doing a 24-2 SITA Standard test to a SITA Faster test. We implemented this protocol for two reasons:
- Even though the literature indicates that the SITA Standard is the gold standard, the Sita faster delivers comparable results.2
- The SITA Standard test takes about five minutes per eye whereas the SITA Faster takes about half the time, which helps with patients who may have fatigue and issues testing properly. It also helped with extra sanitation necessary during COVID protocols.
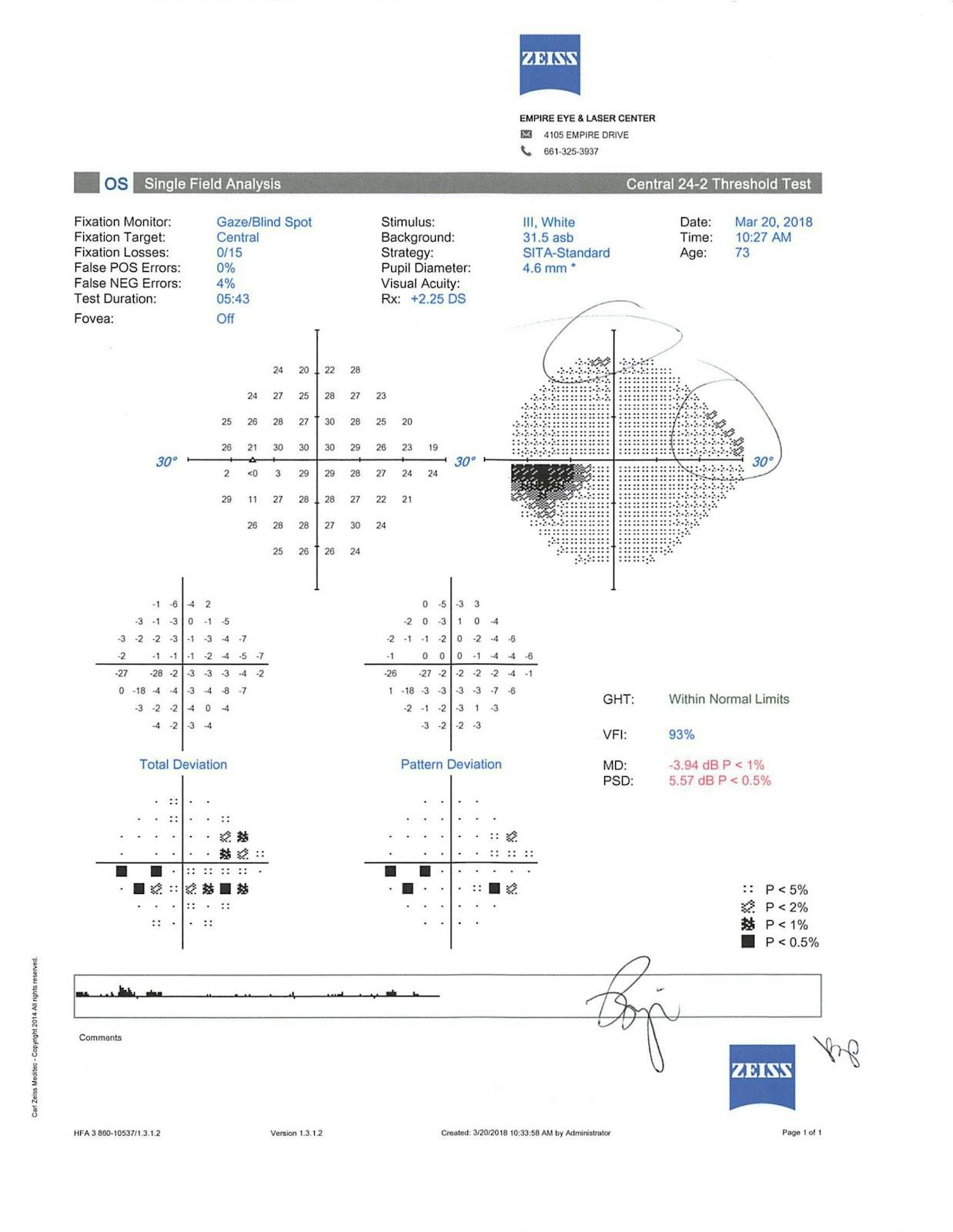
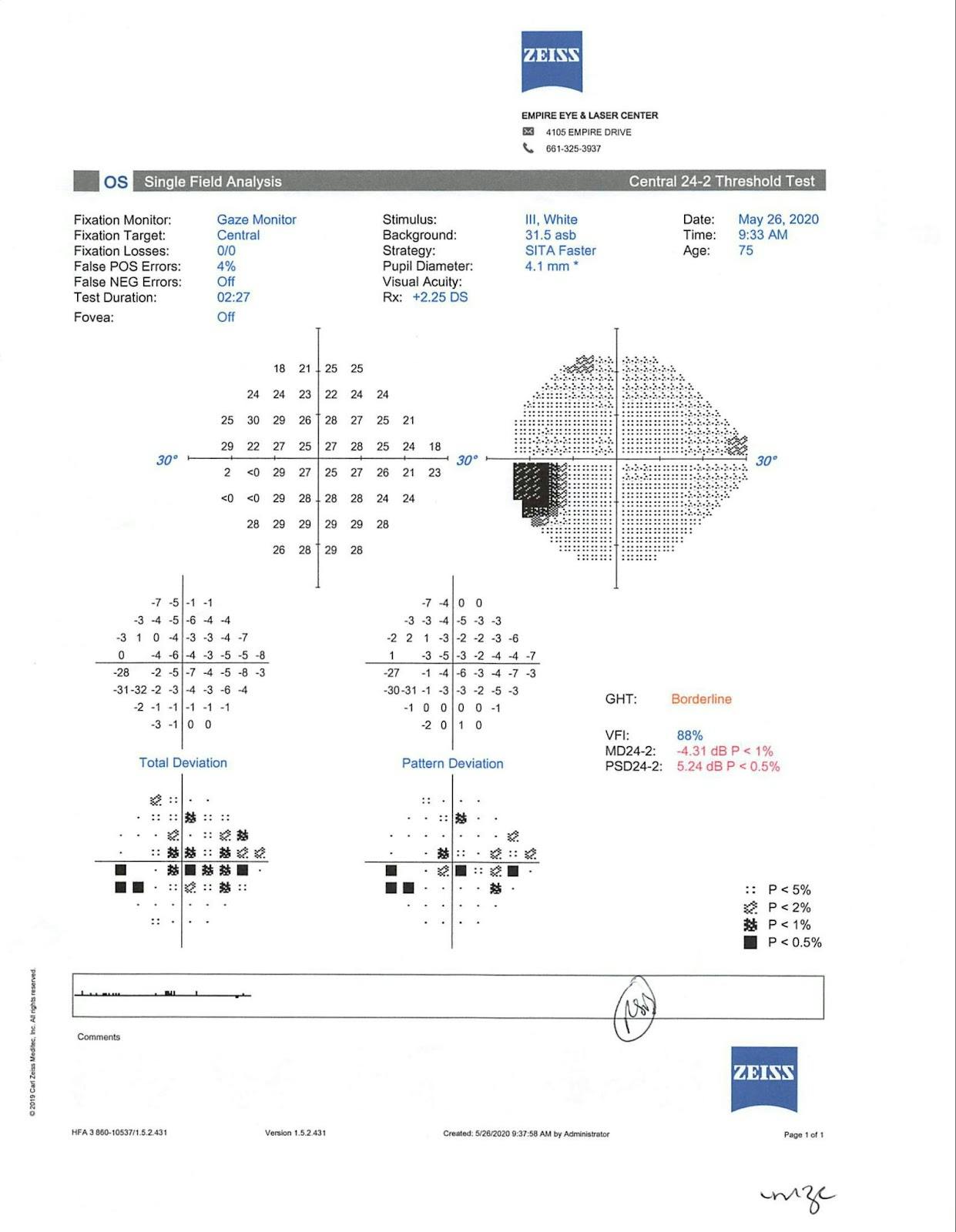
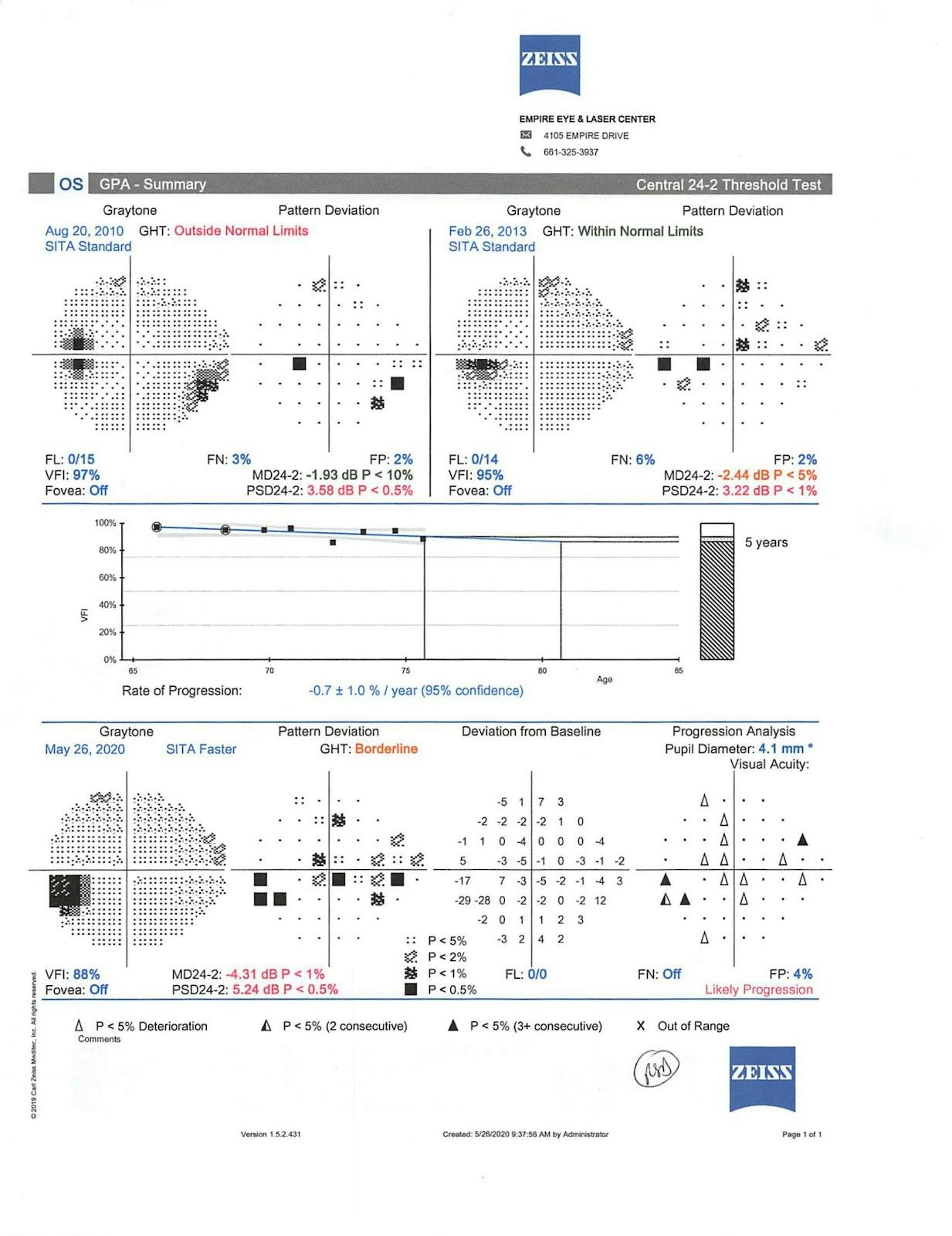
The visual field test indicated that the patient’s right eye was full, whereas his left eye had a superior nasal step with a superior arcuate defect.

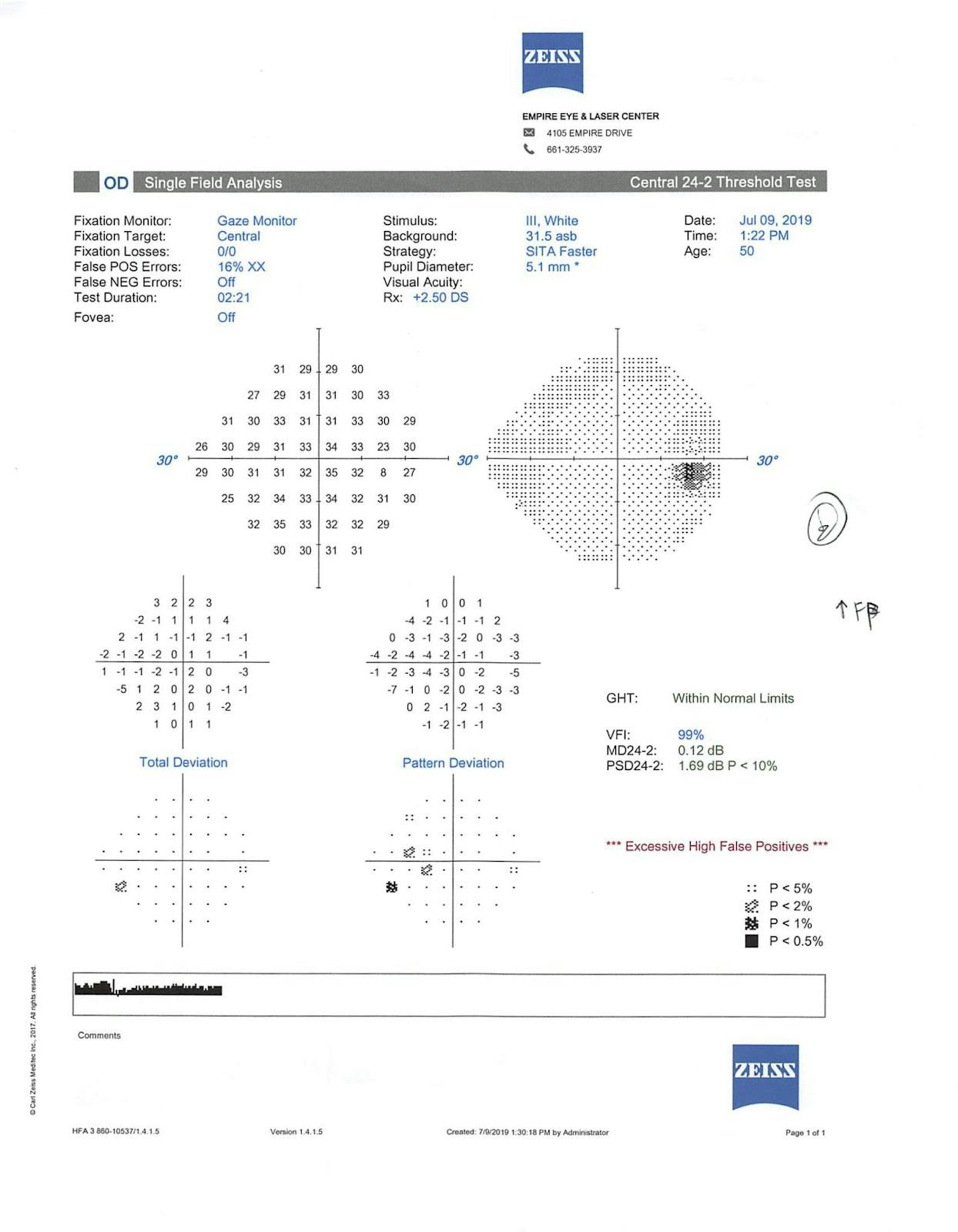


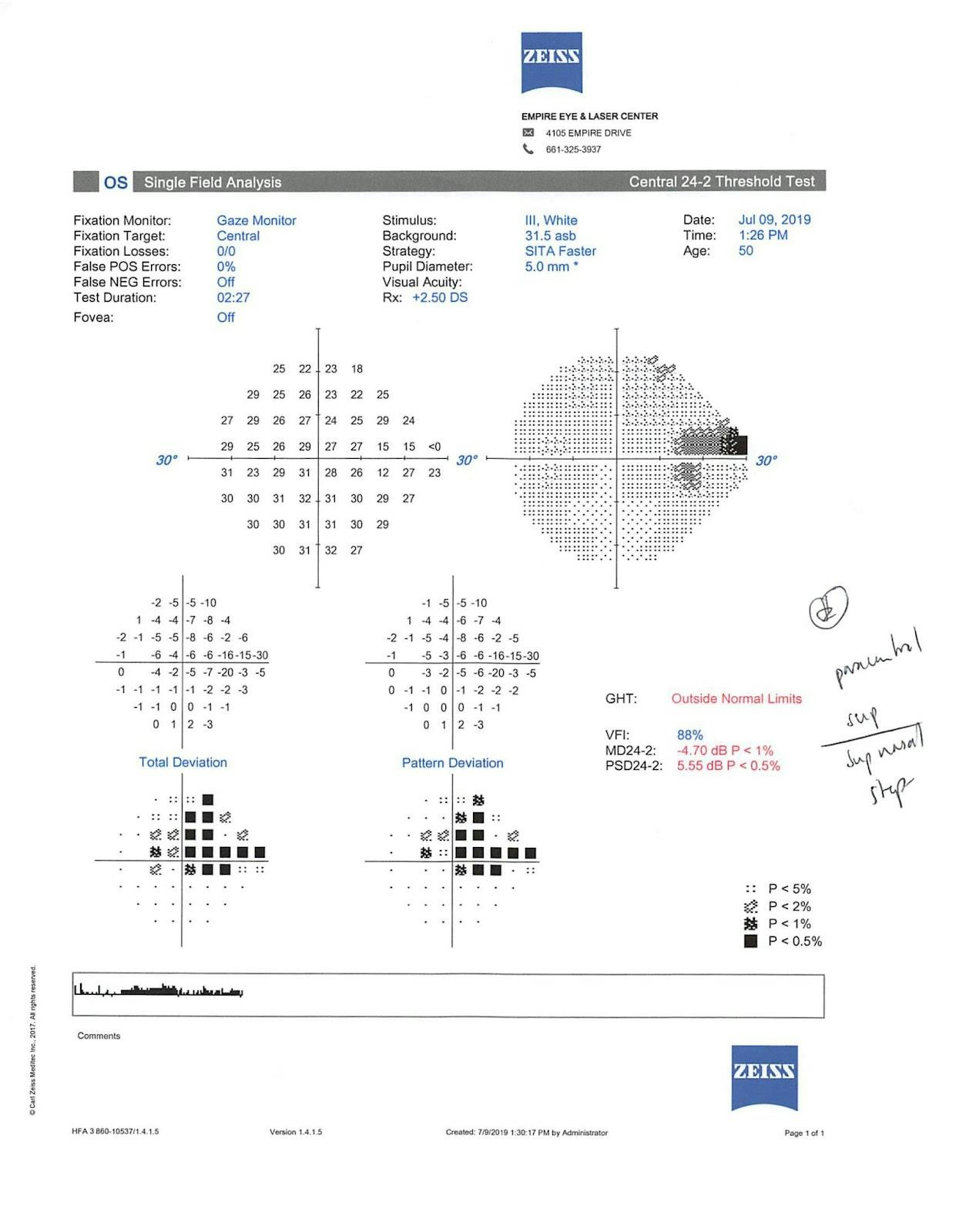

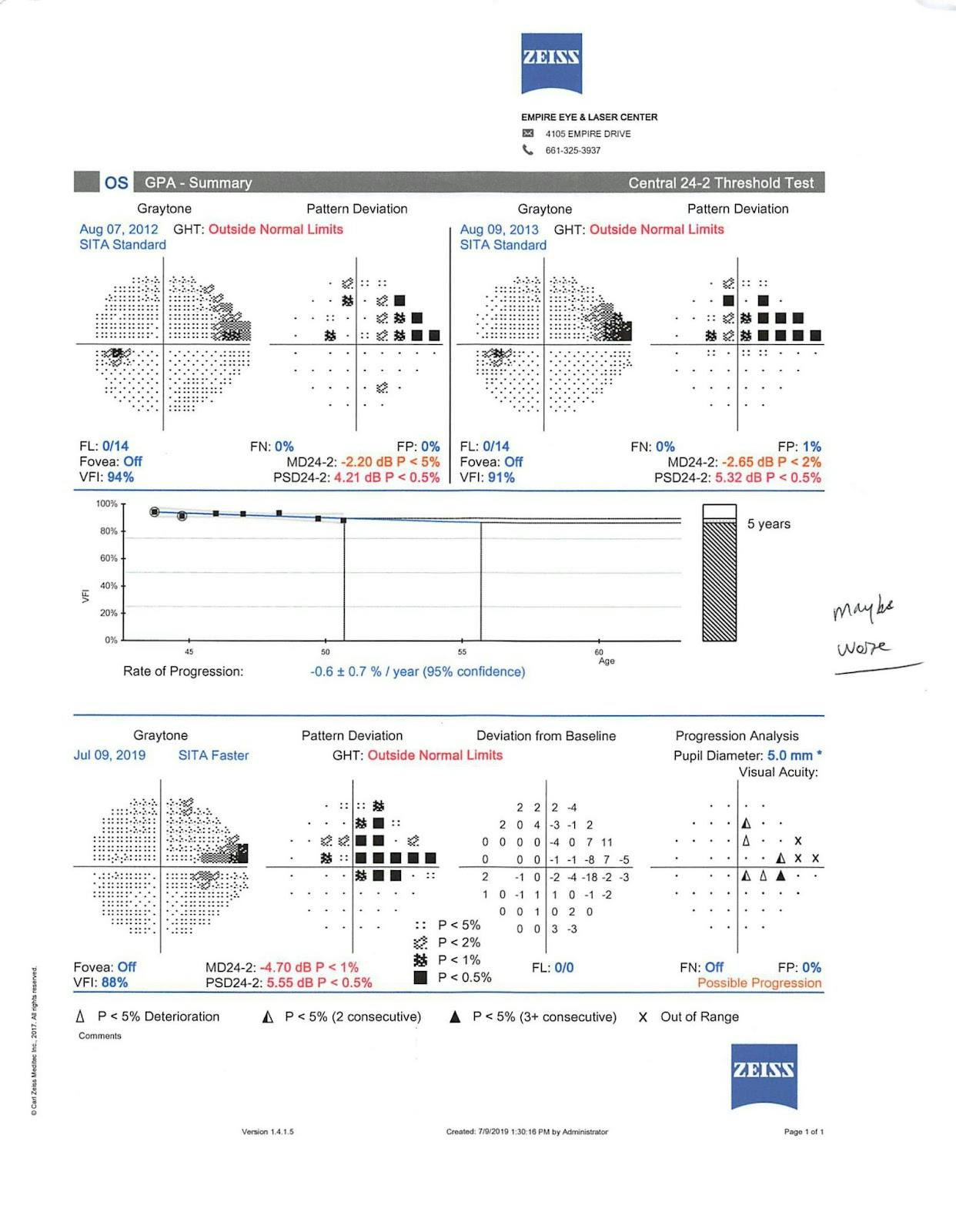
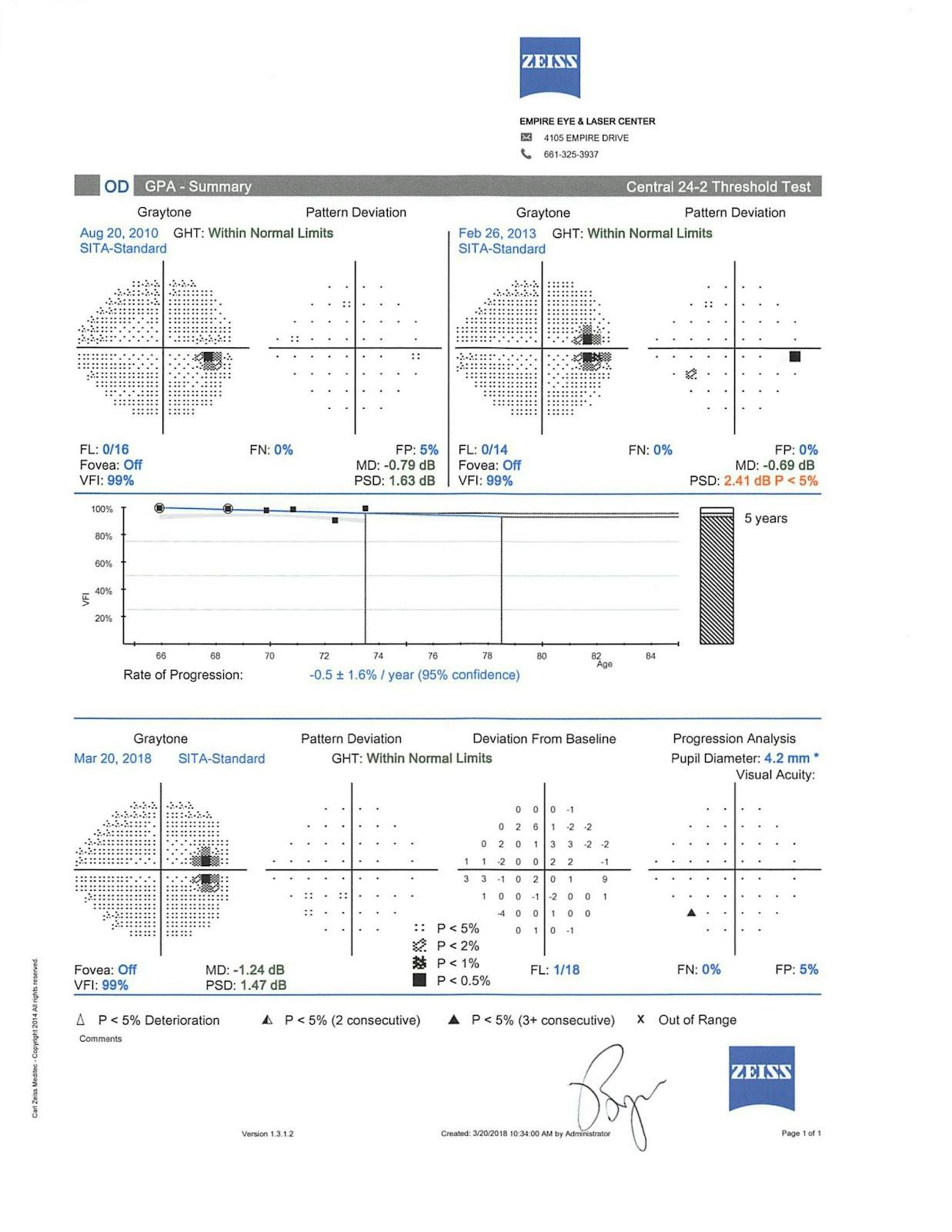
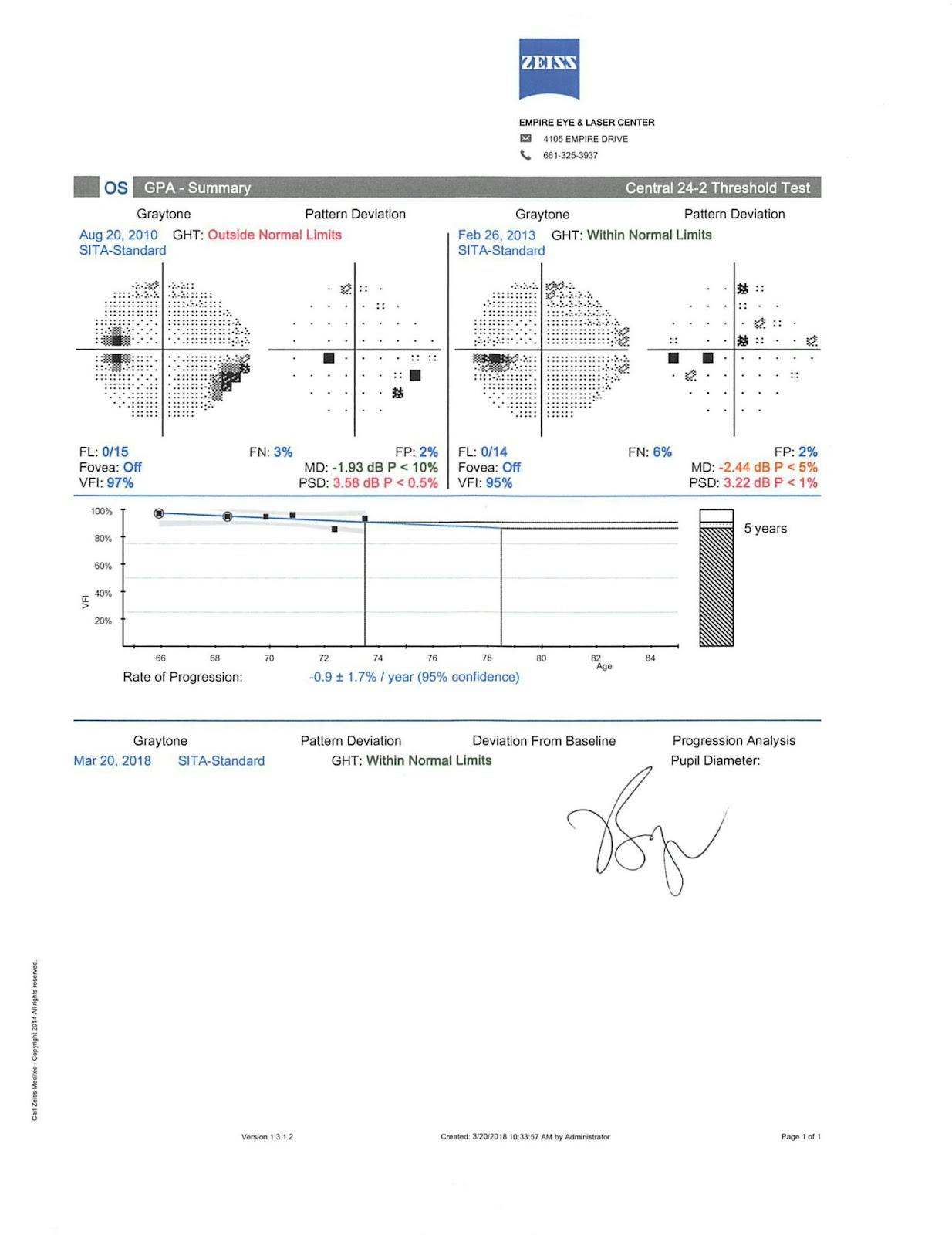
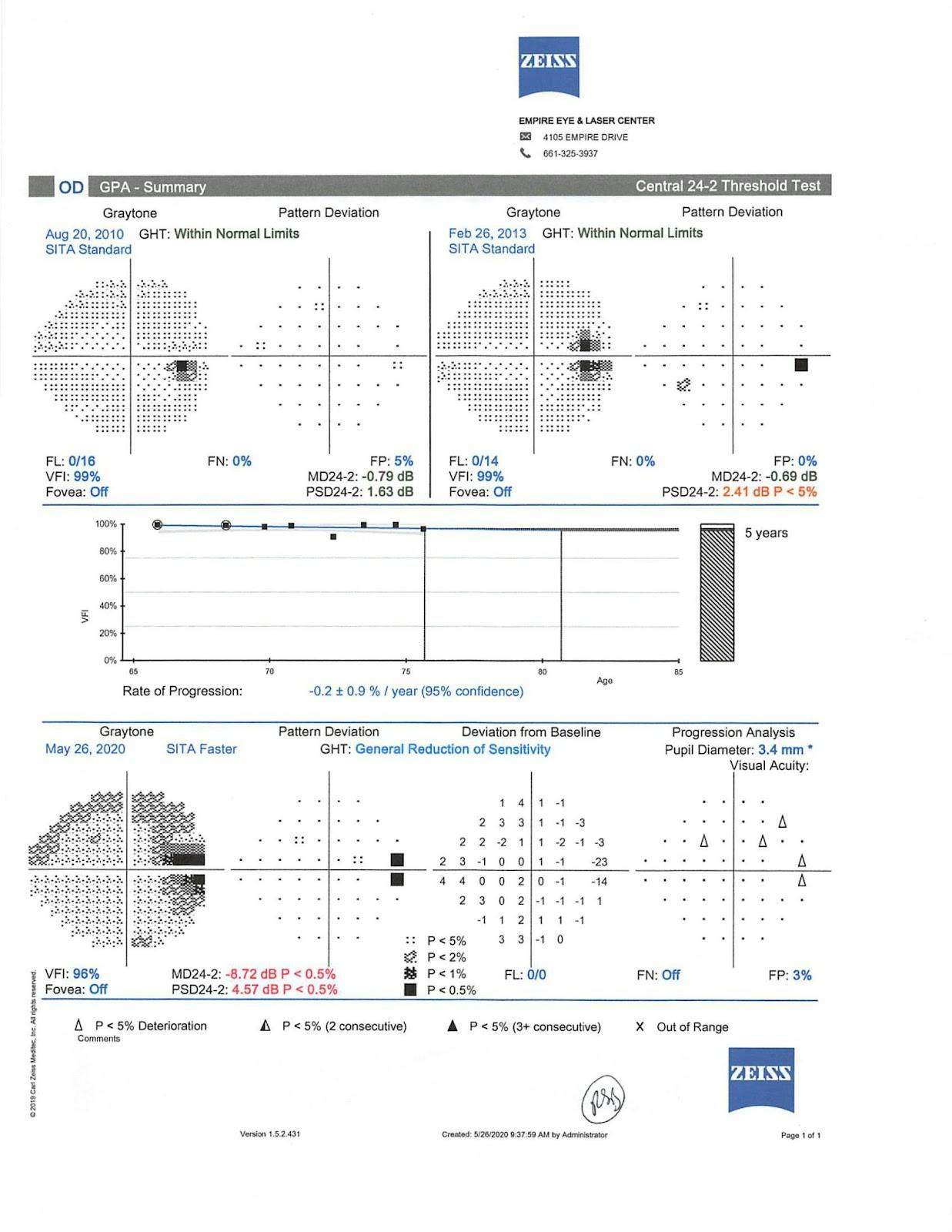
Visual Field OD+OS with GPA Summary
His IOPs had always been in the mid-teens, but gonioscopy confirmed that he had open angles. At that point, I decided his pressure was too high and I switched him from a prostaglandin eye drop to a prostaglandin with a rock inhibitor.

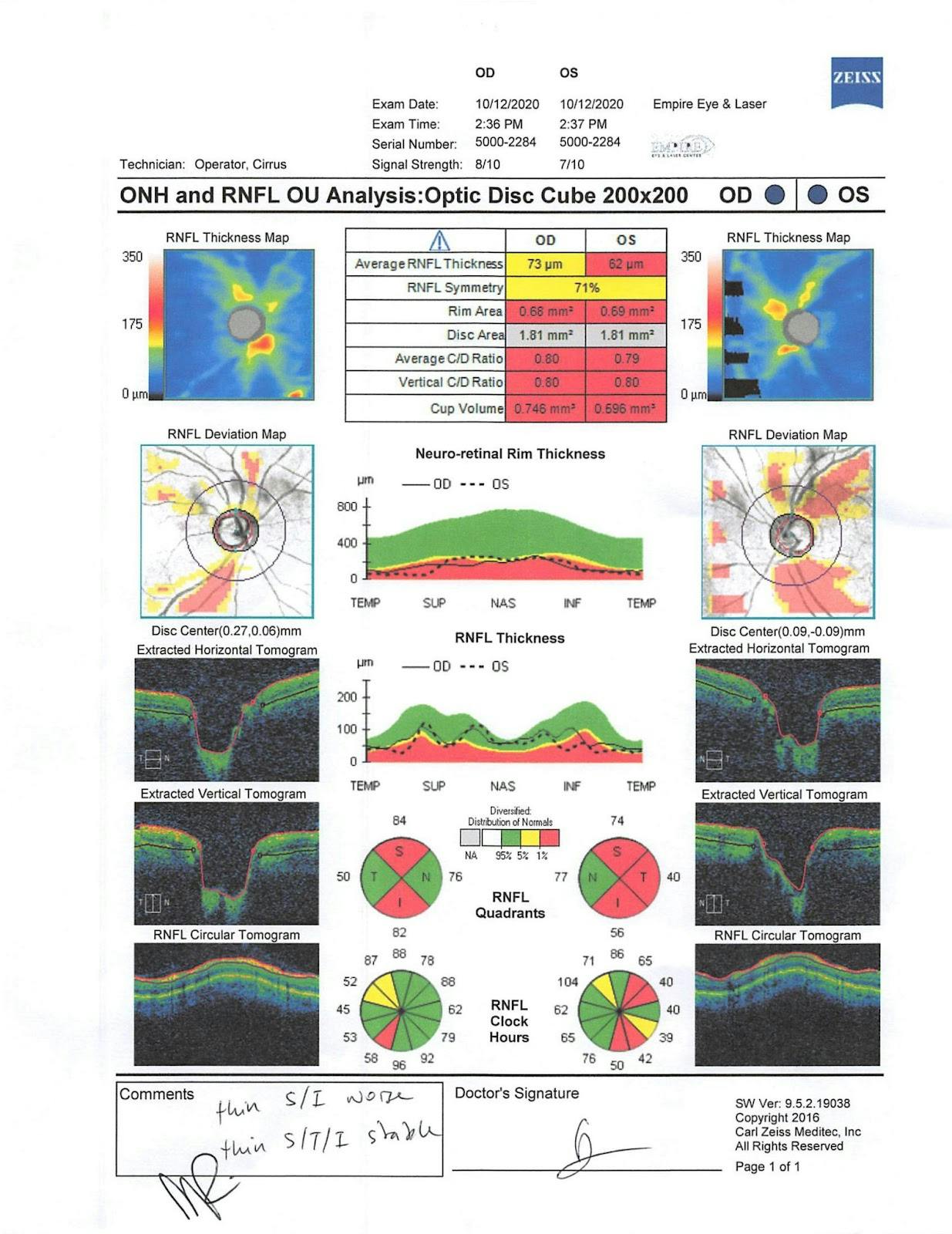

OCT From Follow-Up Visit
Follow-up
When he came back for his follow-up appointment, the pressure had dropped to about 12mmHg in the right eye and 13mmHg in the left eye. However, the patient admitted to unpleasant side effects and asked about alternative medications. We then switched him to Lumigan prostaglandin drops. Currently, the patient is being successfully treated with Lumigan drops and selective laser trabeculoplasty (SLT).
Case study of a 72-year old caucasian female
Case history
A 72-year old caucasian female who presented to our office with a previous diagnosis of potential ocular hypertension came to our office. She had cataract surgery back in 2004 with a yag capsulotomy a few years after that. She also had a history of previous SLT in both eyes in 2013. We had seen her in 2016 when she established care at our office. Her entering IOPs were 15mmHg in the right eye and 16mmHg in the left eye during the slit lamp examination.
-72 year old White Female
- History of Ocular HTN
- Cataract SX x 2004, s/p YAG
- SLT x 2013
Exam
During the exam, I noticed she had a myopic fundus. During my discussion with her, I asked her if she had been nearsighted prior to cataract surgery. She indicated that she had worn glasses up until she had cataract surgery at a very young age. The myopic fundus causes a peripapillary atrophy area around the optic nerve, which made it more difficult to judge the cup to disc ratio, which at that time was said to be about 0.3 in both eyes.

Fundus Photo: OD
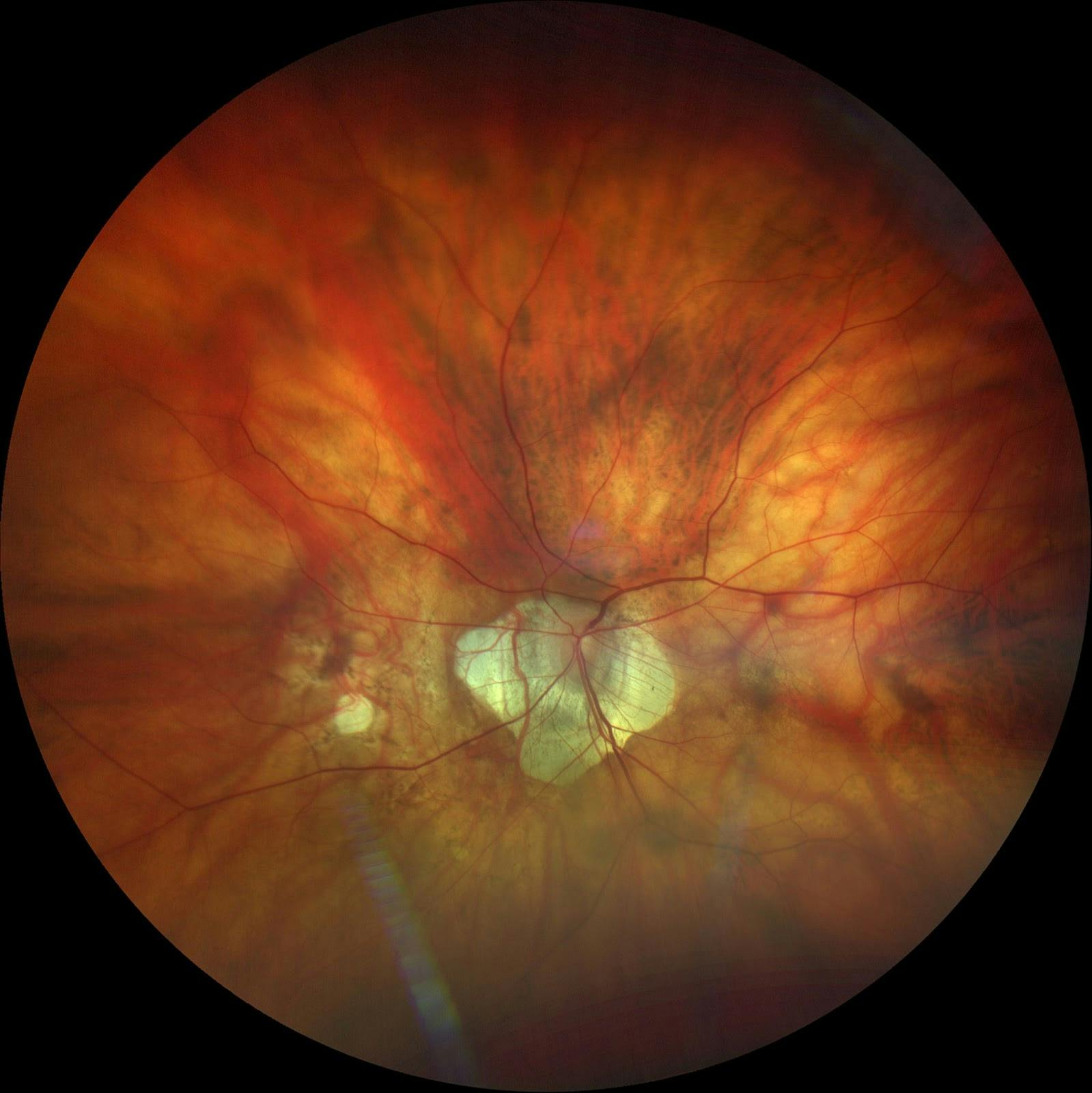
Fundus Photo: OS
As you can see, the fundus photos show that the optic nerve is definitely a bit lighter in contrast to the peripapillary atrophy. It is also a bit tilted which makes it even more difficult to assess the cup to disc ratio. At this point, you have to depend on your own clinical skills to manage a patient.
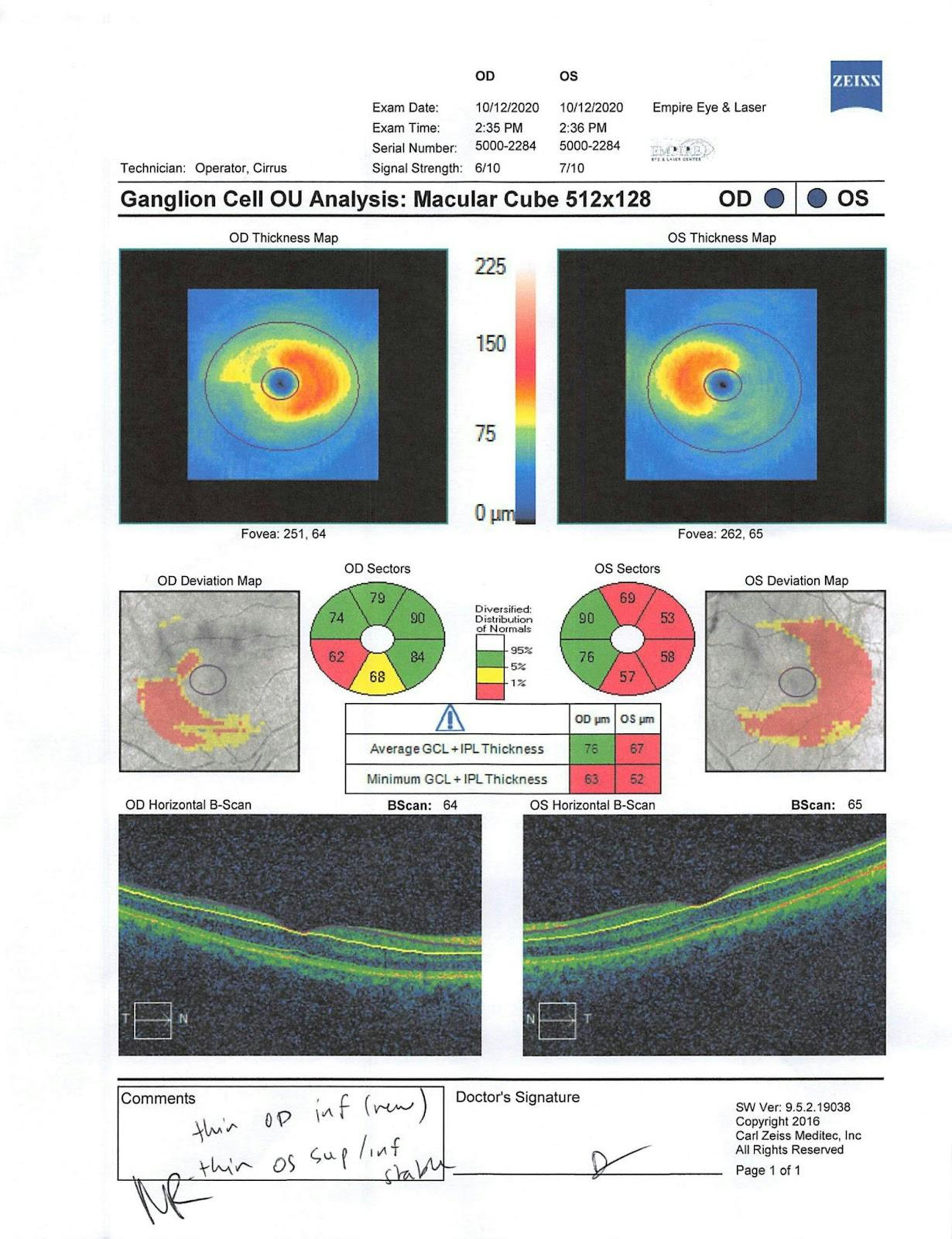
When we performed the optic nerve head OCT analysis, it had a very difficult time measuring the nerve fiber layer around the optic nerve because of the peripapillary atrophy.

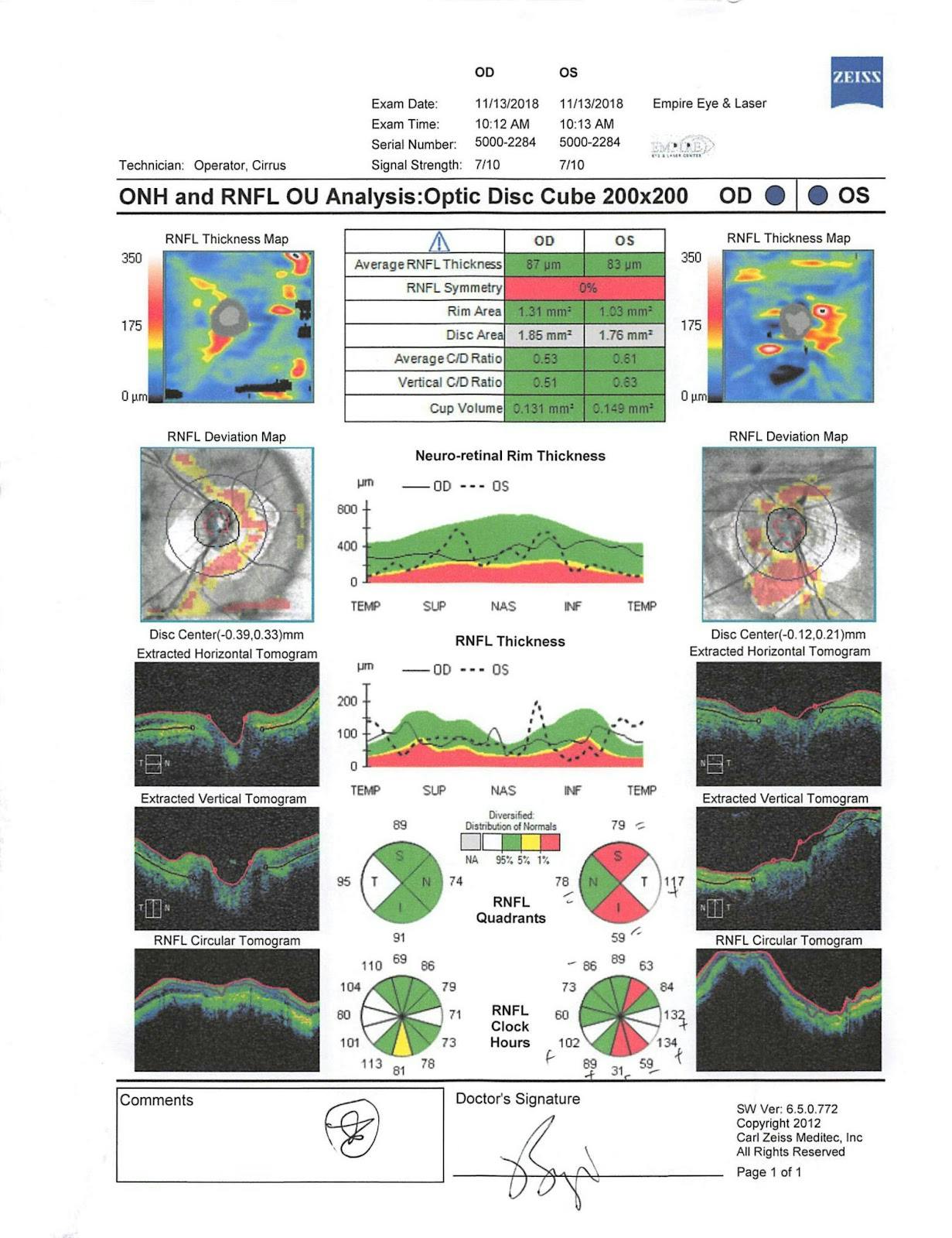



Follow-Up OCT + Visual Field Tests
So this case demonstrates how certain variables like a myopic fundus can make it more difficult to diagnose patients whether or not they are ocular hypertensive, or primary open angle glaucoma, or even potentially glaucoma suspect.
Follow up
Because of her history of ocular hypertension, we decided to monitor this patient closely. In 2017, she came in for a glaucoma follow-up, at which point we had diagnosed a drance heme. Her pressure was still in the mid-teens, but it was creeping up to the 18mmHg-19mmHg range. Then we decided because of her age, she would be a good candidate to monitor. It had been many years since she had a previous SLT done and we thought if her pressure creeped to the low-20 range, we would consider doing a repeat SLT to help lower her eye pressure without having to start her on medication.
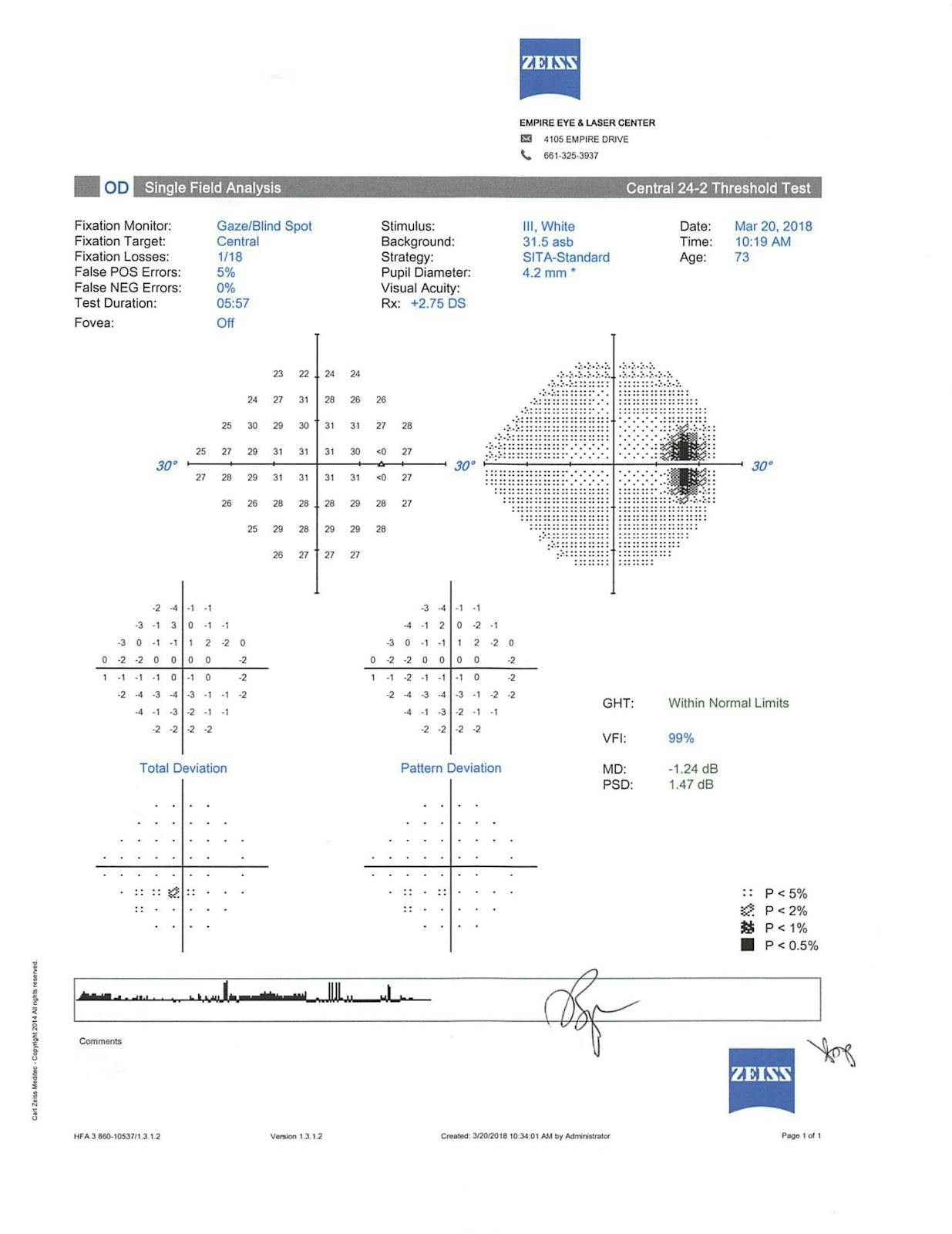
Visual field test
We had the patient return for visual field testing with the HFA. We started with the SITA Standard but then switched to the SITA Faster because this particular patient was having some difficulty in terms of the reliability of the test results.
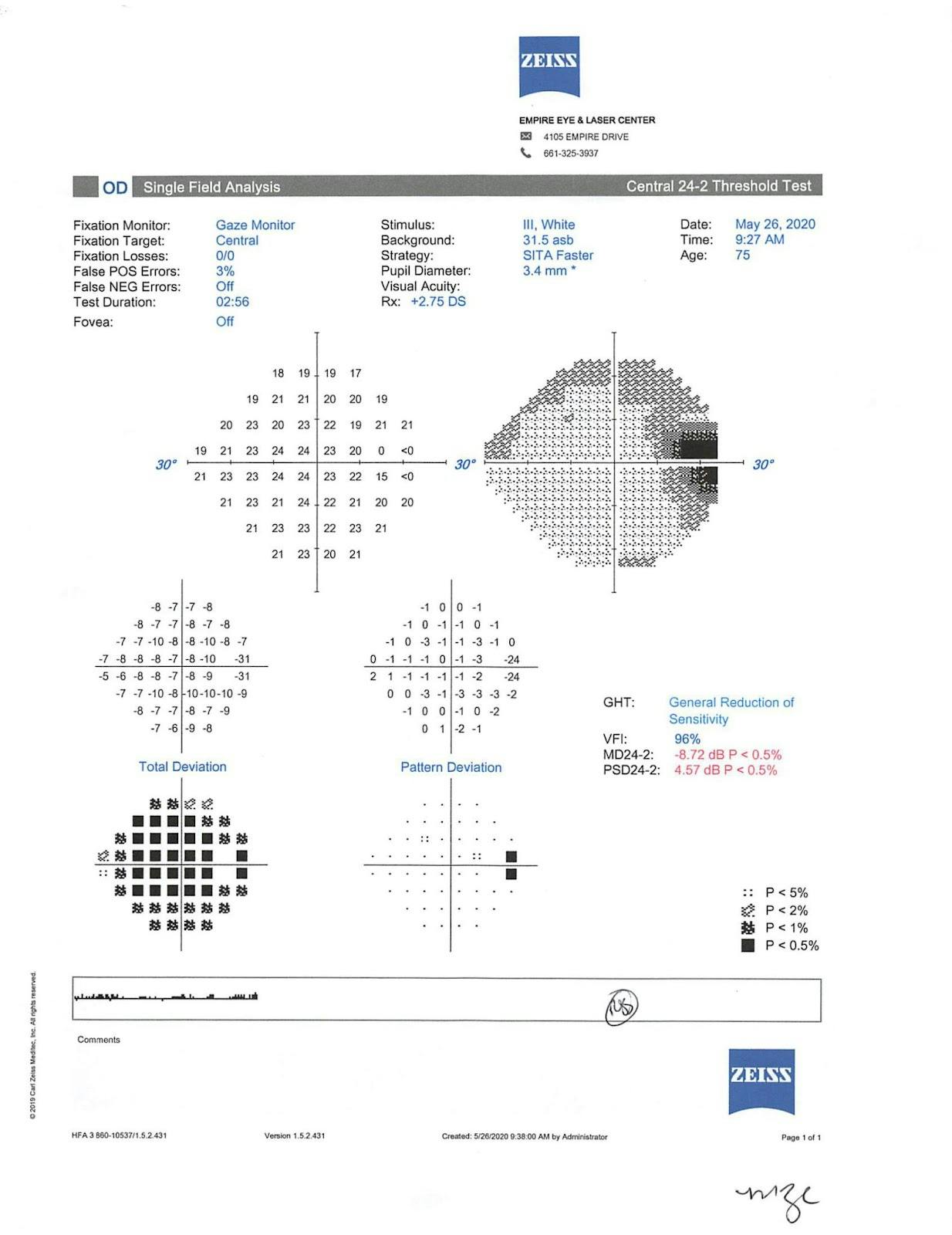

Follow-Up OCT + Visual Field Tests
One noticeable finding is that likely due to the myopic fundus, the patient has an enlarged blind spot, especially in her left eye, which is noted in one of the visual field test results. Currently, we are monitoring her very closely on a 4-6 month basis to make sure we don’t see additional episodes of optic disc hemorrhage.
As you can see, the myopic fundus is also a potential masquerader that can make it more challenging to manage and treat a day-to-day primary open angle glaucoma.
Clinical pearls on integrated glaucoma management
When talking about glaucoma management, there are three things to keep in mind:
- Risk factors
- Diagnostics
- Treatment and management
When I’m talking to my patients about glaucoma, I tell them that it’s a chronic disease that is treatable but not curable. And it really is a summation of risk factors, such as:
- Age
- Ethnicity
- Elevated IOP
- Increased cup to disc ratio
- Genetics
- Corneal thickness
- High myopia
The factor that isn’t discussed often is high myopia. With high myopia you sometimes have a bit of a myopic disc that sometimes makes it difficult for some of your diagnostics to reliably measure the optic nerve fiber layer, which can cause a much more difficult task for you as the primary care optometrist to decide if this patient has glaucoma—or is merely a glaucoma suspect.
I tell patients that it’s never black and white. If it’s black and white then a patient has end-stage glaucoma and no one wants that.
It’s our job as primary care optometrists to educate these patients and explain risk factors, because most are out of their control. I always have patients asking if there is anything they can do. And truly there isn’t, unfortunately. What they can do is come in and get their eyes checked on a regular basis and ensure they are compliant with their drops and/or treatment protocols.
References
- Murphy ML, Pokrovskaya O, Galligan M, O’Brien C. Corneal hysteresis in patients with glaucoma-like optic discs, ocular hypertension and glaucoma. BMC Ophthalmol. 2017;17(1):1.
- Heijl A, Patella VM, Chong LX, et al. A New SITA Perimetric Threshold Testing Algorithm: Construction and a Multicenter Clinical Study. Am J Ophthalmol. 2019;198:154-165.
