




Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in childhood, and of JIA extraarticular manifestations, JIA-associated uveitis (JIA-U) is the most common.1 Uncontrolled JIA-U can lead to blindness. Therefore, emphasis is placed on screening and treatment of JIA-U. This article will review the fundamentals of JIA and JIA-U, the screening guidelines for JIA-U, and the recommended consensus treatment algorithm.
Juvenile idiopathic arthritis subtypes and uveitis risk
There are several subtypes of JIA, including systemic, polyarthritis, oligoarthritic, enthesitis-related arthritis, psoriatic arthritis, and undifferentiated arthritis. The three most common types of these subtypes are systemic JIA, oligoarticular JIA, and polyarticular JIA. Of patients with oligoarticular JIA, up to 10-20% will develop uveitis, and those that are ANA positive are at higher risk of developing uveitis.
Uveitis in JIA can present as either acute or chronic anterior uveitis. Acute anterior uveitis is associated with patients that are HLA-B27+ and is unilateral, episodic, and painful. Conversely, chronic anterior uveitis is often asymptomatic, painless, and vision-threatening, leading to complications such as synechiae, cataracts, band keratopathy, and glaucoma in 25-50% of patients and vision loss in 10-20%.2
Risk factors for vision-threatening uveitis include:1
- Male gender
- Young age of onset
- Short duration between onset of arthritis and uveitis
- Presence of synechiae at initial diagnosis
Screening and monitoring guidelines
The often asymptomatic nature of chronic anterior uveitis associated with JIA make it important to routinely evaluate and screen patients with JIA for signs of uveitis. Two hallmark guidelines together offer cohesive guidance for uveitis in patients with JIA. The first is the 2006 guidelines by the British Society for Paediatric and Adolescent Rheumatology (BSPAR) used by the Royal College of Ophthalmologists in the United Kingdom, and the second is the 2019 guidelines proposed by the American College of Rheumatology (ACR) and the Arthritis Foundation.2,3 The 2006 BSPAR guidelines advise initial screening in JIA suspect or recently diagnosed JIA patients, whereas the 2019 ACR guidelines describe further screening and monitoring in diagnosed JIA or JIA-U patients.
Figures 1 and 2 represent screening and monitoring workflow from the 2019 ACR Guidelines.2

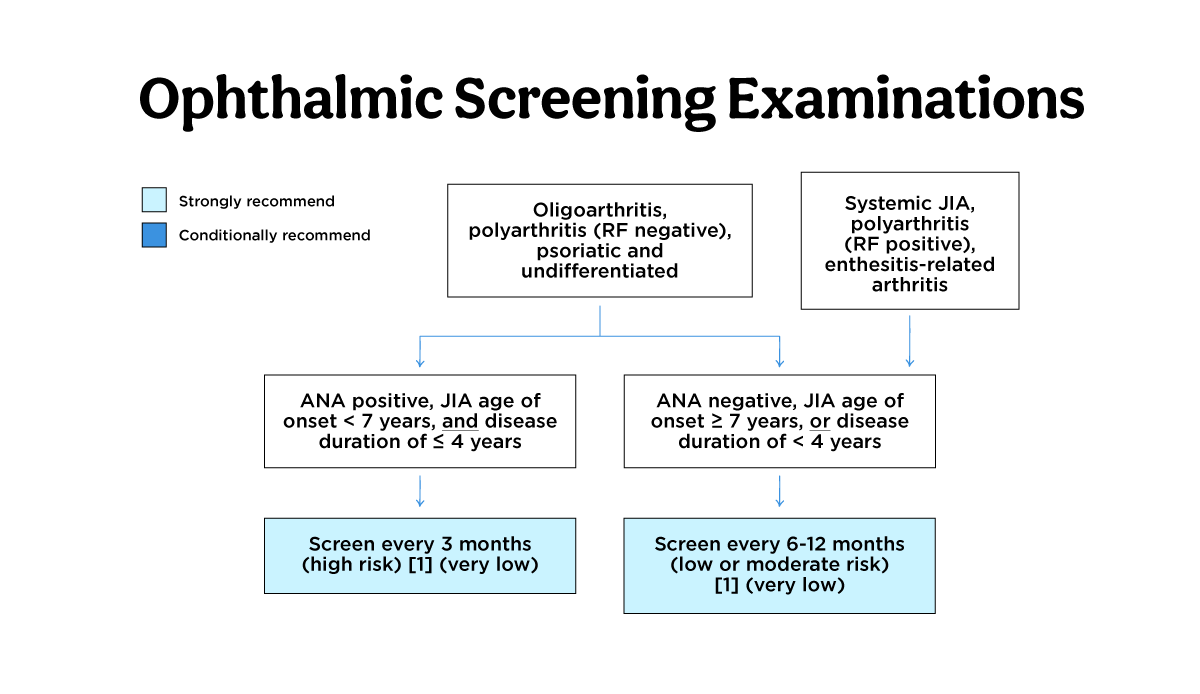
Figure 1

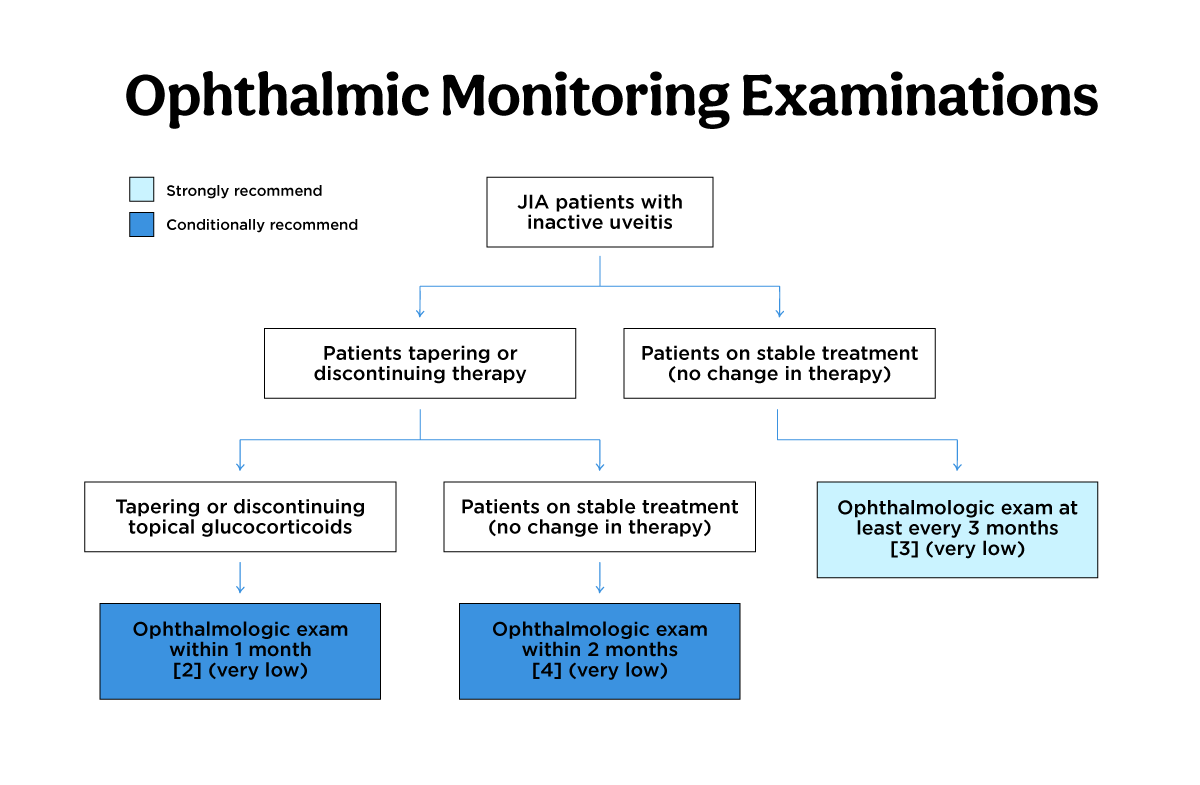
Figure 2
Patients should be referred to a uveitis specialist at the diagnosis or suspicion of JIA. An initial screening examination should occur no later than 1 week after referral for patients with visual symptoms. For asymptomatic patients, screening should occur no more than 6 weeks after referral.
Following diagnosis, risk stratification for the development of uveitis in JIA patients must be done; this helps determine future screening intervals.
Risk stratification for development
High-risk patients match the following:
- Antinuclear antibody (ANA) positive with oligoarthritis, polyarthritis (rheumatoid factor negative), psoriatic arthritis, or undifferentiated arthritis.
- Younger than 7 years of age at JIA onset
- Have JIA duration of 4 years, or less
These patients should be screened every 3 months.
Moderate and low-risk patients are those who match any of the following:
- High-risk JIA subcategories but ANA negative
- Older than 7 years at JIA onset
- Have JIA duration of more than 3 years
- Those with systemic JIA, polyarthritis (rheumatoid factor positive and enthesitis-related arthritis)
These patients should be screened every 6-12 months.
At presentation, it is also important to check for ocular complications. A large cohort study showed that 67% of patients with JIA-U had ocular complications at presentation.4 The most prominent ocular complication was band keratopathy at 31.5%, posterior synechiae at 27.5%, and cataracts at 22.5%.4
Following an initial uveitis diagnosis and treatment, the 2019 ACR paper offers monitoring guidelines during treatment. Patients with JIA and controlled uveitis who are tapering or discontinuing topical steroids should be evaluated in 1 month’s time after every change. On the other hand, those on stable therapy with controlled uveitis do not need monitoring more frequently than 3-month intervals. Finally, those tapering or discontinuing systemic therapy should be seen within 3 months of systemic change.
Importantly, the guidelines strongly recommend educating patients regarding the warning signs of acute anterior uveitis to decrease the delay in treatment, duration of symptoms, and complications of iritis.
Treatment guidelines
Treatment guidelines offered by the 2019 ACR and 2022 Multinational Interdisciplinary Working Group for Uveitis in Childhood (MIWGUC) present a standard workflow for treatment and escalation gave patient symptoms.5 Below we have described a general workflow derived from a review of both guidelines. We recommend eye health professionals review the cited guidelines as further nuances are addressed in the cited papers.
General workflow for uveitis treatment
Topical steroids, prednisolone acetate 1% or dexamethasone 0.1%, are the first-line treatment for JIA-U. While topical steroids are recommended for short-term control, systemic therapy can be considered for several reasons. These include poor prognostic factors, persistent disease, and clinical inactivity that could not be achieved with 3 drops or less of topical steroids. Poor prognostic factors are defined by ocular complications, male sex, and uveitis preceding arthritis, and persistent disease is defined as active uveitis lasting more than 3 months.
Moreover, the duration and frequency of topical steroid use are also considered. Per the ACR guidelines, if patients persistently require 1-2 drops of prednisolone acetate 1% per day for uveitis control, it is recommended to start systemic therapy to taper the topical steroids. In patients still requiring 1-2 drops of prednisolone acetate 1% per day, in addition to systemic therapy, consider escalating systemic therapy.
If starting systemic therapy, systemic steroids are recommended as a bridging therapy to synthetic DMARDS. Of note, systemic steroid monotherapy should not last longer than 3 months. When transitioning to DMARDS, methotrexate is recommended as the first-line agent. Subcutaneous methotrexate is recommended over oral methotrexate. If methotrexate fails, adalimumab should be used.
In patients with severe chronic anterior uveitis and sight-threatening complications, it is recommended to start methotrexate and a monoclonal TNFI over methotrexate monotherapy immediately.
If increasing dosing and frequency of adalimumab fail, tocilizumab or other TNF inhibitors, including infliximab, golimumab, and certolizumab, can be considered. Therapies such as abatacept, JAK-inhibitors, and rituximab can be considered in patients refractory to TNFis and tocilizumab. Other therapies that could be considered include mycophenolate, leflunomide, and cyclosporine. Etanercept should not be considered for uveitis.
Conclusion
In conclusion, JIA-U is a serious condition that all eye health professionals should be aware of. Untreated JIA-U can result in cataracts, glaucoma, and vision loss. Therefore, screening and monitoring of patients with JIA or JIA-suspect is of utmost importance and should be done at intervals dictated by the published guidelines. Coordination with a patient’s rheumatologist from referral and diagnosis to uveitis treatment and management is necessary to ensure the delivery of high-quality care.
References
- Clarke SLN, Sen ES, Ramanan A v. Juvenile idiopathic arthritis-associated uveitis. Pediatr Rheumatol Online J 2016;14. Available at: https://pubmed.ncbi.nlm.nih.gov/27121190/ [Accessed July 21, 2022].
- Angeles-Han ST, Ringold S, Beukelman T, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring, and Treatment of Juvenile Idiopathic Arthritis–Associated Uveitis. Arthritis Care and Research 2019;71:703–716. Available at: https://onlinelibrary.wiley.com/doi/full/10.1002/acr.23871 [Accessed July 21, 2022].
- Anon. Guidelines for Screening for Uveitis in Juvenile Idiopathic Arthritis (JIA) | The Royal College of Ophthalmologists. Available at: https://www.rcophth.ac.uk/resources-listing/guidelines-for-screening-for-uveitis-in-juvenile-idiopathic-arthritis-jia/ [Accessed July 21, 2022].
- Thorne JE, Woreta F, Kedhar SR, et al. Juvenile Idiopathic Arthritis-Associated Uveitis: Incidence of Ocular Complications and Visual Acuity Loss. American Journal of Ophthalmology 2007;143:840-846.e2. Available at: http://www.ajo.com/article/S0002939407001031/fulltext [Accessed July 23, 2022].
- Foeldvari I, Maccora I, Petrushkin H, et al. New and updated recommendations for the treatment of juvenile idiopathic arthritis associated uveitis and idiopathic chronic anterior uveitis. Arthritis Care Res (Hoboken) 2022. Available at: https://pubmed.ncbi.nlm.nih.gov/35638697/ [Accessed July 21, 2022].
