Now, you should have a good foundation on the nomenclature and various forms of age-related macular degeneration (AMD)—see
AMD: A Preamble if you haven’t already! So, we can dive a little more in-depth into neovascular AMD.
The neovascular form of AMD is responsible for 90% of AMD-related severe vision loss, though only 20% of AMD patients develop neovascularization.1,2 This disproportionate burden of vision loss is the reason why billions of dollars and doctor-hours are spent treating and researching neovascular AMD. This is also the reason why all eyecare providers must stay hyper-vigilant when managing AMD patients, identifying neovascularization early, and treating promptly.
Macular neovascularization (MNV), formerly known as choroidal neovascularization, is a late form of AMD characterized by pathological macular angiogenesis, hemorrhage, subretinal fluid, intraretinal fluid, and/or exudation. The latest nomenclature has renamed choroidal neovascularization to MNV because not all neovascular AMD originates from the choroid. The three subtypes of MNV (refer to Table 1) all have the potential to cause profound vision loss secondary to hemorrhage, fluid, exudation, and secondary retinal atrophy; though their pathophysiology differs slightly.
Table 1
| MNV Subtype | Description |
|---|
| Type 1 MNV | Pathological macular angiogenesis, originating from the choriocapillaris, within the subRPE space |
| Type 2 MNV | Pathological macular angiogenesis, originating from the choriocapillaris, within the subretinal space |
| Type 3 MNV | Pathological macular angiogenesis, originating from the retinal circulation, often grows towards the RPE |
Pathological macular angiogenesis, originating from the retinal circulation, often grows towards the RPE
All three subtypes of MNV are funduscopically similar, possessing a combination of fibrovascular proliferation, hemorrhage, subretinal fluid, intraretinal fluid, exudation, and/or retinal thickening. In rare cases, subretinal/intraretinal hemorrhage may break through the retina and lead to preretinal or vitreous hemorrhage. Disciform scarring, the end-stage of neovascular AMD, contains fibrous material without any significant fluid or hemorrhage. Vision is usually severely reduced and further treatment is not necessary.
Using a combination of clinical and OCT cues, it is important to discern active neovascularization from disciform scarring to prevent erroneous referral and treatment. Whereas treatment naïve MNV may grow at a rate of 26 μm per day, disciform scars remain relatively stable over the course of years.
3 Though mild disease activity such as new hemorrhage and fluid may persist in patients with disciform scarring, significant quick growth rarely occurs in these lesions.
OCTA can be used to determine if lesions contain neovascularization and if there is continued angiogenesis that may require treatment.
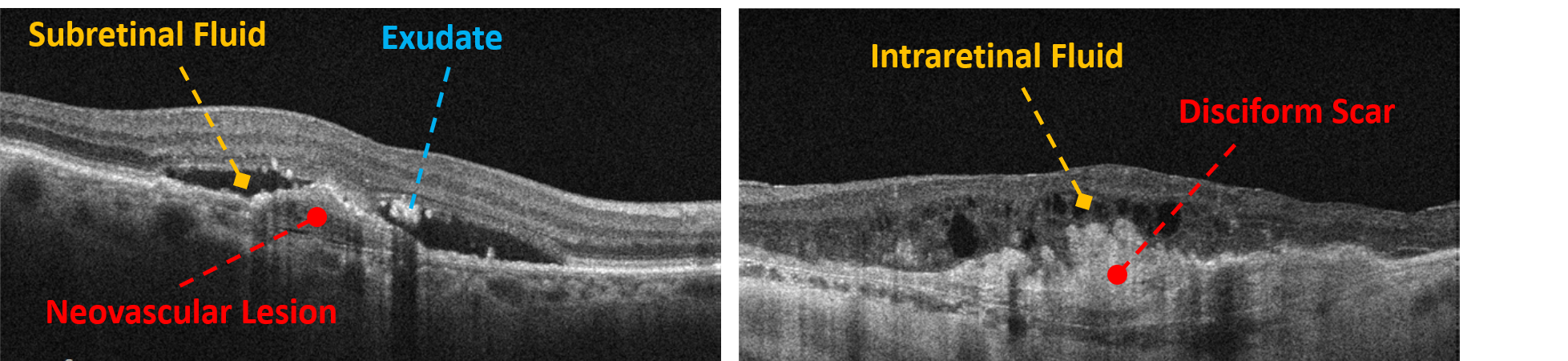
In Image 1, below: On the left, exudative MNV with subretinal fluid and exudate. On the right, a disciform scar with persistent intraretinal fluid. Intraretinal fluid occurs more often in chronic lesions.
Image 1
As MNV progresses, retinal anatomy is altered, and oftentimes a pigment epithelial detachment (PED) forms. PEDs are used to describe any separation of the RPE from the underlying Bruch’s membrane and are named by their etiology (see Table 2 for a summary of various PEDs). In all cases of PEDs, not just AMD-related PEDs, it is important to rule out neovascularization.
Though
dye-based fluorescein angiography (FA) or indocyanine green angiography (ICGA)are the gold standards for detecting or ruling out neovascularization, they are often reserved for patients in which there is a relatively high suspicion of neovascularization. Both FA and ICGA are minimally invasive techniques, though rare serious complications do occur. For this reason, dye-based angiography is not used as a neovascularization screening modality.
But in some cases, it is important to screen for neovascularization, and for this purpose we have
OCT angiography (OCTA).
Table 2
| PED Subtype | Description |
|---|
| Serous PED | Elevation of the RPE from the underlying Bruch’s membrane caused by serous fluid. Cases of AMD-related serous PED are often associated with neovascularization |
| Fibrovascular PED | Elevation of the RPE from the underlying Bruch’s membrane caused by neovascular infiltration |
| Hemorrhagic PED | Elevation of the RPE from the underlying Bruch’s membrane containing hemorrhage |
| Drusenoid PED | Elevation of the RPE from the underlying Bruch’s membrane caused by confluent drusen structures >350μm in base diameter |
The Quickest Introduction to OCTA Ever
OCTA takes advantage of the motion-based variance in sequential OCT images to create noninvasive high-resolution images of retinal and choroidal vasculature. Using eye-tracking technology, each OCT scan is repeated in rapid succession at the same location in order to create a “map” of moving structures.
Because retinal tissue doesn’t move over the course of a few milliseconds, for each set of OCT images, the only difference should be the movement of red blood cells within vessels. The location of moving red blood cells is then used to create vasculature images called OCT angiograms.
Unlike standard retinal OCT scans which are analyzed in a cross-sectional manner, OCTA scans are presented as enface slabs. A single OCTA scan provides both vascular OCTA data and structural OCT data that can be analyzed together at the same time. This allows for visualization of neovascular lesions along with the resultant structural OCT changes that we are accustomed to seeing.
When we think of AMD, we often think of it as a spectrum. First, you have a few drusen, then a lot of drusen, and then you develop neovascularization and/or geographic atrophy. In this simplified world of AMD, we have two jobs: try to prevent neovascularization and detect neovascularization as early as possible so that proper treatment can be initiated. As with most diseases, earlier treatment of neovascular AMD produces better outcomes in both vision improvement and anatomical remediation.
As clinicians, neovascular AMD seems like an easy condition to detect. Patients present with acute vision loss and we see hemorrhage, fluid, and significant structural changes on OCT. But new technology has taught us that maybe we aren’t as good at detecting neovascular AMD as we thought. In studies of patients with neovascular AMD in one eye and intermediate AMD in the fellow eye, 5.5%-27% of intermediate AMD eyes harbored MNV.4.5 This subclinical form of neovascularization was dubbed nonexudative MNV and is most easily detected with OCTA.
Nonexudative MNV is an asymptomatic form of neovascularization without fluid, hemorrhage, or exudation and generally causes minimal disruption to retinal architecture and vision. Possibly a precursor to exudative MNV (the classic type of MNV with fluid, hemorrhage, and exudation), up to 80% of nonexudative MNV will convert to exudative disease within two years.5 For this reason, I image all intermediate AMD patients and all PEDs with OCTA. This way I can ensure that I am not failing to diagnose neovascular AMD in its earliest form.
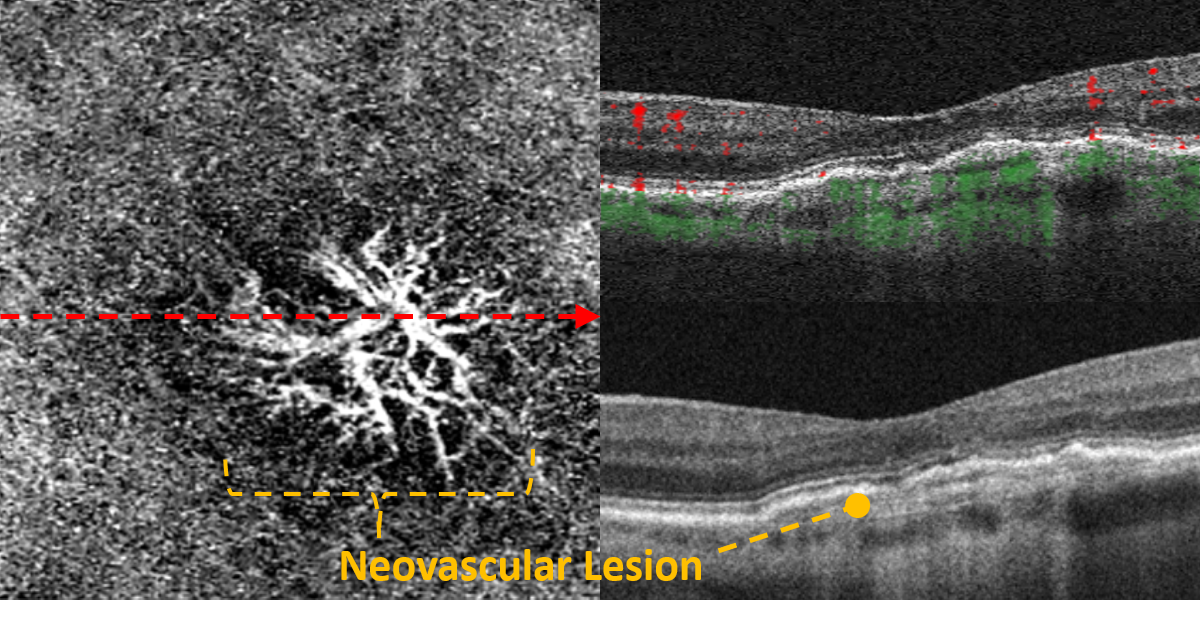
In Image 2, we see, on the left, an OCTA image of nonexudative MNV. On the right, structural OCT images correlating to the OCTA on the left. The top right image has the OCTA perfusion signal overlaid on the structural OCT. The green and red areas represent blood flow.
Image 2
Currently, nonexudative MNV is considered a high-risk neovascular lesion that does not require treatment. No preferred practice guidelines for the management of nonexudative MNV exist, but I usually follow these patients every one to two months to monitor for exudative conversion. I acquire an OCTA image, a standard macular structural OCT image, and a high-definition raster structural OCT image to check for signs of exudative conversion or growth of the nonexudative MNV lesion.
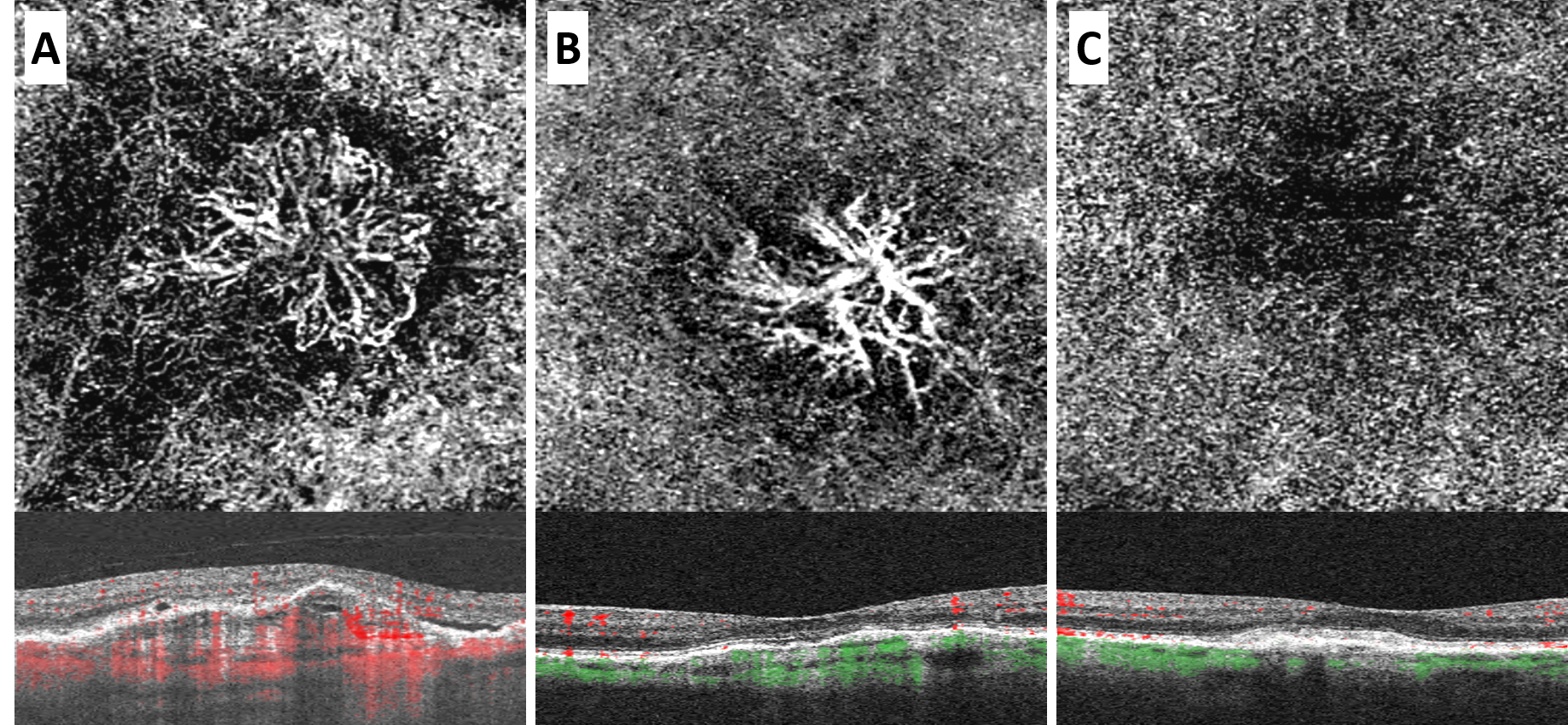
Image 3 represents, from the left, OCTA images and corresponding structural OCT images of exudative MNV, nonexudative MNV, and a disciform scar. Note the small pockets of subretinal fluid in Image A. Perfusion is noted in A and B but not in C.
Image 3
Much the same way that anti-VEGF therapy has revolutionized AMD treatment, OCT and OCTA have redeveloped how we manage AMD. From monitoring drusen to confirming exudative neovascularization to detecting asymptomatic nonexudative neovascularization,
OCT has become integral to the management of all forms of AMD.
Resources
- Ambati J, Ambati BK, Yoo SH, Ianchulev S, Adamis AP. Age-related macular degeneration: etiology, pathogenesis, and therapeutic strategies. Surv Ophthalmol. 2003;48(3):257-293. 21. Ferris FL, III, Fine SL,
- Hyman L. Age-related macular degeneration and blindness due to neovascular maculopathy. Arch Ophthalmol. 1984;102(11):1640-1642.
- Liu, Tin Yan A., Ankoor R. Shah, and Lucian V. Del Priore. "Progression of lesion size in untreated eyes with exudative age-related macular degeneration: a meta-analysis using Lineweaver-Burk plots." JAMA ophthalmology 131.3 (2013): 335-340.
- Or, Chris, et al. "Vascularized drusen: a cross-sectional study." International journal of retina and vitreous 5.1 (2019): 1-6.
- Laiginhas, Rita, et al. "Nonexudative macular neovascularization–a systematic review of prevalence, natural history, and recent insights from OCT angiography." Ophthalmology Retina 4.7 (2020): 651-661.
We have a direct partnership with ZEISS!