



There are common errors in billing and coding that are actually simple to avoid. If we understand where to look, we can see what types of mistakes providers make when billing and coding and we can also take steps to avoid making these mistakes.
Where can we find the data?
The Centers for Medicare & Medicaid Services (CMS) monitors improper payments through a program called Comprehensive Error Rate Testing (CERT). The CERT program monitors a random sample of Medicare fees for service claims annually to determine if proper payment occurred. To think of this another way, consider the CERT data as an indicator of the most likely areas that providers will fail audits.
To evaluate the impact of improper payment on the health care system, consider that in the year 2020 Medicare CERT estimated that 6.27 percent of claims were improperly paid. This represents nearly $26 billion in improper payments. The table below expands on this information for the year 2020.
| Claim Type | Improper Payment Rate | Improper Payment Amount (2) |
|---|---|---|
| Overall | 6.27% | $25.74 B |
| Part A Providers (Excluding Hospital Inpatient Prospective Payment System (IPPS)) | 6.15% | $10.92 B |
| Part B Providers | 8.09% | $8.44 B |
| Hospital IPPS | 3.00% | $3.61 B |
| Durable Medical Equipment, Prosthetics, Orthotics, and Supplies | 31.80% | $2.77 B |
What does the data tell us?
First of all we can see that Part B and DMERC providers are the worst offenders. It is also staggering to consider that nearly 1 in 3 claims for durable medical equipment and 1 in 12 office visits result in improper payments.
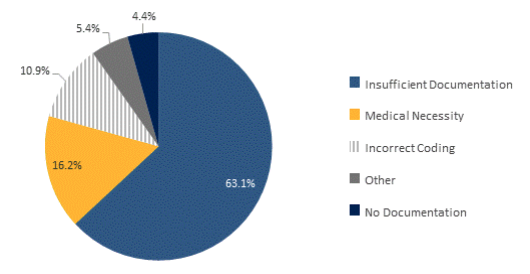
The main reasons leading to improper payments are due to insufficient documentation.
Sixty-three percent of improper payments fall under the category of insufficient documentation. This means that:
- the medical documentation does not support payment for the services that were billed; or
- the CERT reviewers could not determine that the billed services were actually provided, were provided at the level billed, and/or were medically necessary; or
- a specific documentation element that is required as a condition of payment is missing, such as a physician signature on an order, or a form that is required to be completed in its entirety
The table below shows us the impact of each area of improper billing related to the total.

What mistakes should we avoid?
If we break down that sixty-three percent of the pie we will find that the most common reasons for these improper payments include:
Missing or inadequate records
49.2% of failures for insufficient documentation were due to missing or inadequate records. This means that when records were requested by the reviewers, they were either not sent or did not contain the full information.
The simple way to avoid this mistake is to review and ensure that records are sent in full when they are requested.
Certification/Recertification requirements are not met
8.1% of failures for insufficient documentation were due to certification or recertification errors. This means that the physician or health care organizations that want to participate in and receive payment from Medicare have not been properly certified as complying with the Conditions of Participation (CoPs) as set forth in federal regulations.
A simple way to avoid this mistake is to be sure to fully enroll and participate in the insurance plans you wish to be a provider for.
Missing or inadequate orders
2% of failures for insufficient documentation were due to missing or inadequate orders for special testing. This means that a valid provider’s order for the service was not submitted or did not meet the required elements for the order.
A simple way to avoid this mistake is to follow the requirements for ordering and interpreting tests.
Multiple universal errors
38.1% of failures for insufficient documentation were due to multiple issues with missing records, orders, or certification requirements.
If you avoid the first three mistakes you will likely also avoid this fourth common mistake as well.
The bottom line for avoiding common billing and coding mistakes is to be diligent.
If you document every encounter for every specific patient appropriately, order and interpret tests you bill for appropriately, provide timely responses to records requests and recertify you are highly unlikely to fail an audit. Putting redundant systems in place for these common tasks can help you ensure that you will not make unnecessary billing and coding errors.
Eyes On Eyecare has partnered with EyeCode Education to bring our members the best in coding and billing education!

