


Most eye doctors likely don’t go a day without seeing a patient with dry eye disease. It is one of the most commonly encountered conditions we come across in clinic, with approximately 1 in 8 Americans, the same number that will develop breast cancer, suffering from dry eye symptoms.
We know dry eye is multifactorial and can be exacerbated by external and environmental factors. One major factor that is often overlooked by both doctors and patients is cosmetic use. A study performed by O’Dell and Periman et. al. found SPEED scores in current makeup users to be 8.19 ± 5.18 (a score > 5 indicates dry eye symptoms). There are a number of ways cosmetics can both cause and exacerbate existing dry eye, including the ingredients themselves being toxic or irritating, technique and area of application, use of shared and expired products, and improper hygiene and removal.
Cosmetics comprise a massive $532 billion dollar global industry that isn’t going away anytime soon. The FDA defines cosmetics as "articles intended to be rubbed, poured, sprinkled, or sprayed on, introduced into, or otherwise applied to the human body . . . for cleansing, beautifying, promoting attractiveness, or altering the appearance." This includes products used around the eye such as moisturizing or anti-aging creams, gels, serums, false lashes, lash extensions, and eye and facial makeup like concealer, mascara, eyeshadow, and eyeliner.
According to one survey, 66% of women report using makeup at least some of the time. While use of cosmetics by men has increased over the years, women still buy and use more products than men, and as Dr. Cynthia Matossian discusses in her article about dry eye and gender, this may play some role in why women are disproportionately affected by dry eye. However, this doesn’t mean we should ignore cosmetics in our male or non-binary patients.
In the last decade with the rising use of social media like youtube, instagram, and tiktok, makeup and skincare influencers have surged in popularity, and have been encouraging people of all ages and genders to experiment with cosmetic techniques and products. While this has been wonderful for creativity and personal expression, if done improperly can be absolutely devastating for the ocular area and surface.
Lack of FDA Regulation
Many assume cosmetics are heavily regulated by the FDA similarly to pharmaceuticals, and are therefore safe to use on their face and on the delicate skin around their eyes. This is far from the truth: in actuality, there is almost no regulation of makeup and skincare in the United States, and the laws that govern the cosmetic industry have not been updated since 1938. Cosmetics do not need FDA approval before they go on the market, and very few ingredients are banned in the US (unlike in Europe where the EU has banned over 1,328 harmful ingredients). This puts the onus of evaluating the safety of cosmetics on the consumer, and on us as eye care professionals when investigating potential causes of our patient’s ocular surface issues.
Ingredients to Avoid
Unfortunately, knowing which ingredients to avoid is not just a simple matter of recommending certain brands over others, but instead requires thorough evaluation of the entire ingredient list of each product for specific ingredients that may be toxic or irritating. Even some of the most expensive brands have products with questionable ingredients. You may find that the same brand has some products that are okay, and others that are not. Be very wary of any cosmetics that do not list their ingredients on the package or their website.
Keep in mind individual sensitivities as well, as some patients may be allergic to ingredients that are totally fine for others. In addition, formulations of products change frequently, so just because someone has been able to tolerate a product for a while, doesn’t mean they will always be able to tolerate it. Check the ingredient list each time before purchasing, and encourage spot or patch testing products to help in determining offending agents before major reactions occur.
Non-Exhaustive List of Ingredients to Avoid
| Ingredients | Why they include them and why we should avoid them |
|---|---|
| Benzalkonium chloride (BAK) | Preservative, toxic to epithelial and goblet cells, disrupts tear film |
| Cinnamates | Fragrance, pro-inflammatory, activates TRPV1 and TRPA1 receptors on dendritic cells and corneal nerves |
| DMDM hydantoin | Formaldehyde donating preservative |
| EDTA | Preservative, prevents divalent cations Ca2+, Mg2+, disrupts tear film stability |
| Formaldehyde | Preservative, irritant to corneal nerves, causes burning, itching, redness, tearing, dose dependent meibomian and epithelial cell death |
| Fragrance | Fragrance, irritant, can cause allergic reaction, contact dermatitis |
| Hydroxymethylglycinate | Formaldehyde donating preservative |
| Nylon fibers | Lengthening agent in mascara, foreign body induced conjunctivitis |
| Parabens (methyl-, isobutyl-, propyl-) | Preservative, toxic to meibomian cells, xenoestrogens can potentially disrupt hormone function |
| Phenoxyethanol | Non formaldehyde donating preservative (often marketed as “paraben-free”, meibomian cell death even at low concentrations |
| Phthalates | Plasticizer and solvent, decreased cell proliferation of corneal endothelial cells, pro-inflammatory |
| Prostaglandins (anything with -prost) | Lash growth, aerodynamic compromise, hyperpigmentation, periorbital fat changes (1) |
| Quaternium 15 | Formaldehyde donating preservative |
| Vitamin A metabolites | Anti-aging skin products, in high concentrations can alter meibomian glands |
| Sodium laureth sulfates | Surfactant in many makeup removers, detergent that strips natural oils |
| Toluene | Solvent, pro-inflammmatory, aberrant activation of TRP receptors (1) |
| Triclosan and Triclocarban | Preservative and stabilizer, pro-inflammatory, activation of TRPA1 receptors |
| Urea (anything with urea in the name) | Formaldehyde donating preservative |
To make it even more confusing, words like “hypoallergenic”, “ophthalmologist or dermatologist tested,” “natural,” “organic,” “gentle for sensitive eyes,” and “clinically proven” are not regulated by the FDA and are thus essentially meaningless buzzwords. Patients may think they are doing their due diligence only buying products that are “ophthalmologist approved,” but in actuality these could be the very cause of their eye irritation.
Eyeliner Dos and Don’ts
Another factor to consider beyond just the components of the products themselves is how they are being applied. Remind patients not to tightline or apply eyeliner to the delicate waterline of the eyelid to avoid impacting meibomian glands and disrupting the tear film. A study by the University of Waterloo showed that makeup applied to the inner eye margin migrated into the tear film 15-30% more than that applied outside the lash line. Another observational study found reduced tear film layer thickness in those that used eye cosmetics like eyeliner.
Tattoo eyeliner and other permanent makeup around the ocular area have also been shown to cause a number of potential complications such as dermatitis, tear film instability, and meibomian gland atrophy. The ink used is not regulated by the FDA and can contain harmful metals and pigments like lead, titanium dioxide, chromium, nickel, etc.1 Improper technique by the tattoo artist or aesthetician can also cause corneal or conjunctival injury.
Lashes, Lashes, Lashes
Eyelash lengthening through means like serums, false lashes, and extensions is all the rage right now, and many patients do not realize how tampering with the normal lash can affect their ocular surface. Optimal lash length has been shown to be one third of the width of the eye. Lashes this length best filter dust particles, minimize tear film evaporation, and redirect flow of air. Shorter lashes don’t stop the air flow, and longer ones (such as those created by serums, false lashes, and extensions) direct the flow to the ocular surface increasing evaporation and worsening dry eye symptoms. Add on regular mask wearing right now during the COVID-19 pandemic and mask associated dry eye (MADE), and you’ve got a recipe for a dry and unhappy ocular surface.
Lash serums with prostaglandin analogs like Latisse are very effective at growing long lashes, and thus very popular. However, they have all the same side effects that we are familiar with in our glaucoma patients using this class of medications. These include hyperpigmentation of the eyelid skin and iris, altering of the aerodynamics of the lashes, dermatitis, orbital fat atrophy, and obstructive meibomian gland dysfunction.1 A study by Mocan showed that 92% of glaucoma patients using only prostaglandin analogs had MGD compared 58.3% in those using a different class of medication. Approximately 1 in 3 over the counter lash serums have prostaglandin analogs as their main ingredient.1
The glues used to adhere false lashes and extensions can cause contact dermatitis and inflammation due to their cyanoacrylate-like adhesives. These glues contain formaldehyde-emitting compounds known to be irritating to the ocular surface. In addition people with fake lashes are less likely to perform proper eyelid hygiene and thus more likely to develop blepharitis and demodex. Recent studies have shown that 73.3% of patients experienced ocular side effects like itching, redness, and pain after application of eyelash extensions.
Lash tinting and dyeing isn’t a much better alternative either; they have been shown to cause acute inflammation, edema, watering, and conjunctival reactions. Also watch out for nylon fibers in mascaras, used to improve their lengthening effect, at least one case study has shown the lengthening fibers (some over 1mm in length) can actually embed into the conjunctiva causing extreme irritation. You may want to suggest alternatives like non-waterproof mascaras and mechanical eyelash curlers that do not use any chemicals instead.
Keep Clean and Don’t Share
A study out of the UK showed that 1 in 4 women do not remove their makeup at night. We must encourage patients to remove their makeup every night, no matter how late or tired they are to decrease build up of product which can encourage growth of microbes and demodex, cause infection, and clog meibomian glands. A study by O’Dell and Periman et al showed SPEED scores were higher in makeup users that did not use makeup removers (Mean:10.5 ±6.75) than those who did (Mean 7.6±4.62). However, we also need to be careful with what types of products are used as makeup removers. Many contain detergents that are known to to strip and break up the lipid layer of the tear film. Oil based products like argan or jojoba oil are better options.
Cleaning makeup brushes and sponges regularly, approximately every 2-3 weeks, is also incredibly important to stop growth and spread of microbes. Encourage patients to clean and never share makeup products or makeup brushes with other people as this can increase potential of microbial contamination and ocular infection. Don’t forget that sharing includes using tester products at stores as well as makeup used by makeup professionals applying the same products on multiple clients. A study by Sedzikowska showed that demodex survived in a mascara sample for 56 hours! If multiple users are dipping into the same tube within that time period there is potential risk of spread of demodex from person to person.
Don’t Forget Skincare
Makeup use during the COVID-19 pandemic has actually decreased due to lack of in person interaction and mask wear, while a focus on skincare has increased. Eye creams used to improve the appearance of wrinkles and dark circles are extremely popular. While retinoids can be great for improving the appearance of the skin, in high concentrations they may impact meibomian gland health. Remind patients to be careful using these products around the ocular area. Also recommend that patients favor products with packaging that prevents constant re-dipping of fingers that can introduce microbes into the products; pumps and tubes are preferred to pots and tubs. In general, avoid eye creams with fragrance.
Expired products
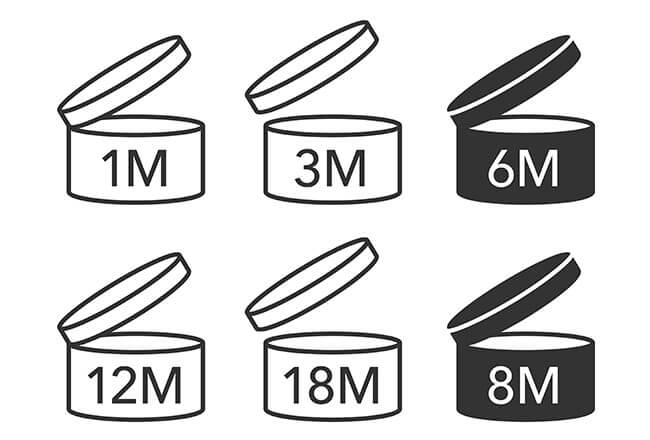
According to one study, over 97% of women reported having used or currently use expired makeup. Many have no idea how to check when products should be disposed of. Cosmetic products will often have these labels on the back to indicate how many months they are safe to use after opening. Recommend patients note the day packages are opened and what date they should be thrown out in order to prevent irritation from broken down products or risk of infection from microbial growth.

JUST RELEASED: The 2024 Dry Eye Report
Unlock insights from 330+ optometrists in the highly-anticipated 2024 Dry Eye Report! Explore cutting-edge trends, treatments, tools, and advice to help you stay ahead in dry eye management, all for FREE! Click here to download!
Clinical Tips
Make sure to evaluate makeup behind the slit lamp. Look for debris from poorly removed mascara and eyeliner, as well as false lashes and fibers in the tear film. It is important to have a discussion with your dry eye patients about their cosmetics. An online study by Periman and O’Dell showed that 88.76% of patients did not discuss cosmetics use with their eye care providers. In our dry eye clinic we routinely ask patients to bring in their makeup and skin care products to their exam so we can help them go through each one and determine which to keep and which to toss. Patients leave with a shopping list of new products with cleaner ingredient lists.
Pay particular attention to any products used around the eye such as eyeliner, mascara, and eyeshadow, as well as concealer, creams, serums and makeup remover. This can be of particular importance for your contact lens patients, as some cosmetic ingredients can become trapped under the lenses and cause corneal abrasions and irritation. A study by Luensmann showed that coating of makeup removers and mascara on soft contact lenses actually warped the physical dimensions of three commonly used silicone hydrogel contact lenses showing change in sagittal depth, diameter, and base curve potentially impacting the fit and comfort of the lenses. Recommend inserting contact lenses before applying makeup, and consider switching patients that use cosmetics regularly to daily disposable contact lenses. Finally, have patients switch to non-waterproof products to decrease the need for harsh chemicals to remove them.
Don’t forget to think about cosmetics when treating your dry eye patients. Most patients are unaware of the location and role of meibomian glands, and how easily the homeostasis of the tear film can be thrown off by external factors like cosmetics. Give them lists of ingredients to avoid, and go over proper care and removal techniques. Websites like The Detox Market do a lot of the work for your patients by vetting products for clean ingredient safety and making it easier to find safer options. Most patients will not be willing to stop using cosmetic products entirely, but we can set them up for success by providing them with useful information to make safer choices that will keep their ocular surface happy.
Special thanks to Laura Periman, MD for her assistance with this article.
There are many different kinds of artificial tears on the market for mild to severe dry eye. Laura Goldberg, OD/MS discusses the different types of artificial tears and shares her insights with a comparative list of the artificial tears on the market with a handy download. Click here to view the list.
References
- Periman, Laura M. Dry Eye Whiplash: The head-turning beauty practices and ingredients of your Chronic Dry Eye patients, your male patients and how doctors can help. Lecture presented at: Canadian Dry Eye Summit 2020; November 2020; Virtual.


