



One of the first vitreoretinal conditions an ophthalmology resident will encounter will be a retinal detachment. Retinal detachment occurs when the neurosensory retina separates from the retinal pigment epithelium (RPE). It is an urgent diagnosis and, without timely intervention, there is significant risk of permanent vision loss.
Broadly, there are five types of retinal detachments: rhegmatogenous, tractional, exudative, combined rhegmatogenous-tractional, and macular hole-associated. The most common type is rhegmatogenous where a retinal break (e.g., horseshoe tear) occurs leading to the accumulation of subretinal fluid and separation of the neurosensory retina from the underlying RPE. Management of rhegmatogenous retinal detachment commonly involves surgical retinal reattachment and we will focus on this type of pathology for the remainder of this communication.
Finding the Break
To confirm a rhegmatogenous retinal detachment, one must first find the retinal break (or breaks in rhegmatogenous cases with multiple retina tears). Luckily, this paramount part of the diagnostic challenge is facilitated by the Lincoff retinal detachment rules. The Lincoff rules are a set of guidelines on finding the retinal break based on the configuration of the retinal detachment.1 It is based on a retrospective analysis of 1000 retinal detachment cases where 96% of included cases conformed to these rules.1


Figure 1: The Lincoff rules
The four Lincoff rules, summarized in Figure 1, are as follows:
- Superior temporal or nasal retinal detachments that do not cross the midline. Retinal break is found 98% of the time within one-and-a-half clock hours from the side with higher subretinal fluid.
- Total or superior retinal detachments that cross the vertical midline. The retinal break is superior 93% of the time, within a triangle with its apex at 12:00 (at ora serrata) and base at 11:00 and 1:00 (at equator).
- Inferior retinal detachments. Retinal break is found 95% of the time, located on the inferior side with the highest level of subretinal fluid.
- Inferior bullous retinal detachment (also known as a “gutter” detachment). Retinal break is found on the higher side of the retinal detachment, above the horizontal meridian, with subretinal fluid tracking inferiorly.
To help with the diagnosis of retinal detachment, ophthalmology residents should be well versed in risk factors associated with increased risk of retinal detachment. These risk factors can be summarized as follows: age, history of retinal detachment in fellow eye, high myopia, family history of retinal detachment, lattice degeneration, history of trauma, previous cataract surgery (0.6-1.7% annual risk) and previous laser posterior capsulotomy.2
Finally, one should always be cognizant of situations where retinal breaks cannot be identified on careful dilated scleral depressed exam. Typically, there are four scenarios where this may occur:
- Chronic retinal detachments where retinal break has sealed.
- High myope with very small retinal breaks that are difficult to locate on dilated depressed exam (e.g., blonde fundi).
- Retinoschisis, in which case the retina is “splitting” and not actually separated from the underlying RPE.
- Exudative or inflammatory pathology.
Management of Rhegmatogenous Retinal Detachment
Rhegmatogenous retinal detachment repair is one of the most common indications for retinal surgery. As one can survey from the discussion above, a multitude of anatomical presentations exist; thus, retinal re-attachment is best managed with an individualized approach as opposed to one standardized procedure. Over the past 25 years, pars plana vitrectomy (PPV) has gained favor with vitreoretinal surgeons and is being increasingly utilized over scleral buckling (SB) for retinal detachment repair.3
PPV has gained favoritism due to a variety of elements including the increased availability of small gauge instrumentation, improved viewing, and lighting systems as well as economic factors. However, primary SB surgery should remain the treatment of choice for certain types of retinal detachments. Although some retinal detachments can be repaired with laser retinopexy or pneumatic retinopexy in the clinic, we will focus our discussion on primary SB, PPV, and cases of advanced pathology.
Primary Scleral Buckling for Retinal Detachment Repair
SB was first described in 1949 by Ernst Custodis and further popularized by Charles Schepens and Harvey Lincoff in the 1950s. SB principles and techniques have remained relatively unchanged over the past six decades. The technique favorably alters the geometry and physiology of the eye to help close and maintain closure of retinal breaks. Inward indentation of the eye, along with externally applied cryotherapy or laser photocoagulation, aid in creating a permanent adhesion between the neurosensory retina and the RPE. Furthermore, SB-induced indentation helps overcome the forces tending to detach the retina including cellular epiretinal proliferation and the magnitude and direction of vitreous traction on the neurosensory retina.4
SB is advantageous because it not only treats any existing retinal breaks but also supports the vitreous base, minimizing the likelihood of new retinal tears from developing.5 Additional advantages of SB over PPV include a lower incidence of cataract which may help preserve accommodation in younger patients, reduced complications associated with intraocular surgery such as endophthalmitis or choroidal hemorrhage, and eliminating the need for post-operative positioning or travel restrictions.6
Want more info on primary scleral buckling? Check out the first installment of our surgical video series, where three experienced surgeons walk you through the procedure and offer clinical pearls!
SB surgery should be strongly considered in patients presenting with the following scenarios: (i) young, phakic patients with no posterior vitreous detachment (SB avoids cataract formation and induction of a posterior vitreous detachment during PPV can be technically challenging and create iatrogenic retinal breaks in younger patients); (ii) retinal dialysis (commonly there is no associated posterior vitreous detachment with an anterior retinal dialysis and SB allows better support of the anterior location which can be difficult to visualize in phakic patients) (Figure 2); (iii) patients with extensive lattice degeneration or multiple retinal breaks (SB with an encircling segment provides 360-degrees of support to the vitreous base and peripheral retina thereby reducing the likelihood of new subsequent retinal tears); (iv) high myopia in phakic patients (SB will not cause significant cataract acceleration, whereas PPV will accelerate the formation of cataract).

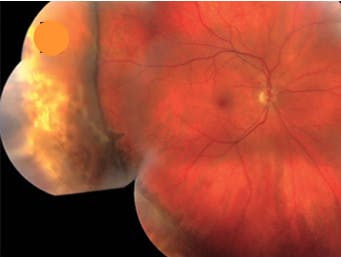
Figure 2: Scleral buckle indent
Fundamentally, primary principles of SB involve closing all retinal breaks by apposing the RPE to the neurosensory retina and reducing the dynamic vitreoretinal traction at sites of vitreoretinal adhesion. To accomplish this, most SB procedures fall into one of three categories:
- Encircling circumferential buckle (i.e., 360-degree buckle). This is used in cases with retinal breaks in three or more quadrants, diffuse retinal pathology (e.g., lattice degeneration) or when there is concern about possible unidentified retinal breaks. These buckles are placed parallel to the limbus.
- Segmental circumferential buckle. The SB are used in cases where the retinal breaks span less than six clock hours and all breaks are identifiable and treatable with cryotherapy or laser retinopexy. These buckles are placed in parallel to the limbus.
- Radial buckle. Radial SB are typical in cases with a single retinal break in an easily accessible location. These buckles are placed perpendicular to the limbus. A radial buckle may also be added to an encircling buckle in cases where the retinal tear is irregular or exhibits rolled edges.
SB surgical technique can be summarized as follows: Conjunctival peritomy and isolation of the rectus muscles. Be aware of key anatomical landmarks such as vortex veins. Eyes typically have anywhere from four to eight vortex veins present. Although number of vortex veins is variable, there is at least one vein in each quadrant of the sclera. Knowledge of vortex vein location is important because damage to these veins during eye surgery could produce potential complications, namely choroidal detachment (Figure 3). External localization of all retinal breaks using indirect ophthalmoscopy and a scleral depressor to mark each break on the external sclera. At this time, possible external drainage of subretinal fluid can be performed in detachment cases where subretinal fluid prevents adequate cryotherapy or photocoagulation treatment (e.g., bullous detachment, chronic detachment, detachment with inferior retinal breaks).

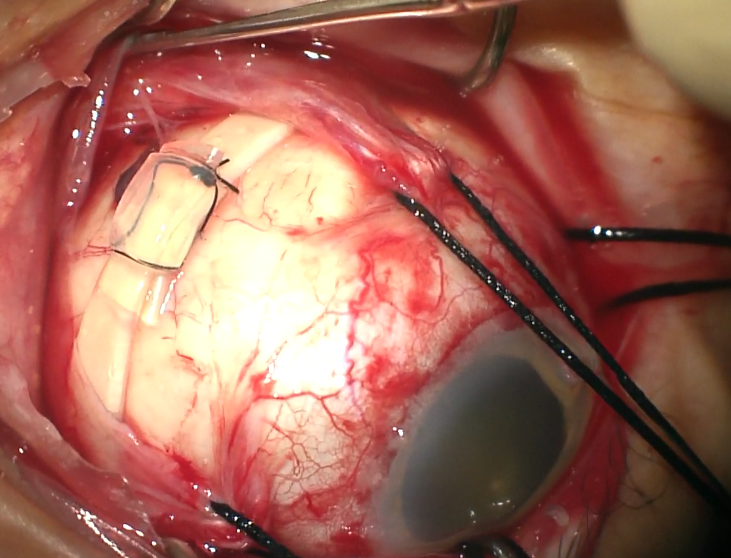
Figure 2: Vortex vein
Once subretinal fluid has been drained, treatment of retinal breaks with cryotherapy and/or photocoagulation can be performed followed by placement of the SB components. Once the SB has been placed, confirmation that all retinal breaks are treated and supported via scleral indentation and direct visualization (typically with indirect ophthalmoscopy), and that the central retinal artery is perfused is necessary. Finally closure of Tenon’s capsule and conjunctiva is accomplished with primary suture closure (e.g., 6-0 plain gut or 7-0 Vicryl suture).
Given the recent technological advances excellent success rate of PPV, there are specific scenarios in which a SB is relatively contraindicated: cases with difficult visualization (e.g., media opacity such as vitreous hemorrhage limit ability to treat with cryotherapy and/or laser retinopexy), posterior breaks (difficult for external drainage of fluid and placement of SB), scleral thinning (increased risk of globe rupture), significant vitreoretinal traction (e.g., cases with tractional membranes, proliferative vitreoretinopathy, proliferative diabetic retinopathy), or cases with significant macular pathology (e.g., macular hole, epiretinal membrane, vitreomacular traction).
Pars Plana Vitrectomy for Retinal Detachment Repair
With the advent and adoption of small-gauge (25- and 27-gauge) vitrectomy platforms, PPV is the most commonly performed surgical procedure for retinal re-attachment. Generally, PPV consists of internal drainage of subretinal fluid through the retinal break(s) or a drainage retinotomy at the time of air-fluid exchange, sealing of retinal breaks with endolaser, and placement of tamponade (e.g., air, gas, silicone oil).
Specifically, setup for PPV involves the placement of three trocar/cannulas by marking a point 3.5 to 4 mm posterior the limbus; typical positions are inferotemporal for the infusion (position and function of the infusion cannula must always be confirmed prior to use to avoid incorrect placement of the trocar in the subretinal or choroidal space). Similar cannulas are placed in the superotemporal and superonasal quadrants for the endoilluminator and the vitrectomy handpiece. Visualization is commonly done with a binocular indirect viewing system.
The core vitrectomy procedure involves removal of all unopacified vitreous and any vitreous membranes present. Many surgeons use a diluted mixture of triamcinolone to better visualize the vitreous and confirm the presence of a posterior vitreous detachment (technique known as chromovitrectomy). Triamcinolone can identify posterior vitreous or proliferative membranes present which must be removed (Figure 4). Peripheral vitreous can be removed with the vitreous cutter and scleral indentation; scleral indentation allows the peripheral vitreous, as well vitreous from retinal breaks, to be carefully removed while avoiding traction at the vitreous base. Once core and peripheral vitrectomy have been completed, inspection should be carefully executed for 360-degrees to ensure no additional peripheral retinal breaks are missed. Intraocular cautery can be used at this time to mark the retinal breaks.

Figure 4: Triamcinolone staining
Next, whereas drainage of subretinal fluid in SB is usually performed externally, with PPV, air-fluid exchange involves internal drainage of subretinal fluid through retinal break(s) or a drainage retinotomy, while concurrently introducing air via the infusion cannula. This can be performed using a silicone-tipped cannula, tilting the eye and removing subretinal fluid through the retinal break(s). Sealing of retinal breaks can now be accomplished with endolaser to encircle and demarcate the pathologic areas.
Finally, intraocular tamponade is performed with gas-air exchange. Short-acting isovolumetric gas tamponade (e.g., 20-24% SF6) lasts approximately four weeks; in comparison, long-acting gas tamponade (e.g., 14-16% C3F8) will provide gas support to the retinal breaks for about eight weeks. Gas-air exchange involves injecting the desired non-expansile gas concentration through the infusion cannula while allowing air to escape through one of the superior cannulas. The cannulas can then removed. Small gauge vitrectomy wounds are typically self-sealing, but one should ensure that they are watertight and confirm no leaks are present. Any leaking sclerotomy wounds should be closed with suture (e.g., 7-0 Vicryl).
Interested in pursuing a retina fellowship? Check out our ultimate guide!
Management of Complex Retinal Detachments
Complex retinal detachments secondary to proliferative vitreoretinopathy, proliferative diabetic retinopathy and uveitis represent challenging cases for the vitreoretinal surgeon and learning ophthalmology resident. In these patients, it is appropriate to consider a combined PPV and SB procedure.7,8 Think of this approach as a “belt and suspender” approach which may optimize the likelihood of successful re-attachment of the retina.
These complicated retinal detachments are analogous to onions with multiple layers of pathology that need to be addressed. Successful outcomes in these cases require that, much like you “peel” an onion, you “peel” or remove each layer of pathology. Conceptually, there are three planes or layers—with respect to the neurosensory retina—that need to be addressed: pre-retinal adherent posterior hyaloid, proliferative vitreoretinopathy membranes, epiretinal membranes and internal limiting membranes, and subretinal bands.
Not uncommonly, a triamcinolone-stained residual layer of vitreous can be found over the posterior pole and peripheral retina in many eyes with complex retinal detachments; these includes some eyes with a pre-existing posterior vitreous detachment or Weiss ring.9 Utilizing a Tano diamond-dusted membrane brush (Figure 4, above), Flexloop, forceps or the vitreous cutter on aspiration, the adherent posterior hyaloid needs to be removed.10 The adherent posterior hyaloid is likely part of a spectrum of proliferative pathology related to incomplete posterior vitreous detachment, vitreoschisis, and immature membrane formation.
On and within the neurosensory retina, frank membrane formation, in the form of epiretinal membranes, leads to traction and foreshortening of the retina; consequently, these need to be removed.11 The presence of epiretinal membrane is 8.00 times (crude odds ratio, 95% CI: 1.43 - 44.92, p = 0.0182) more likely to have development of proliferative vitreoretinopathy).12 Similarly, presence of cystoid macular edema in complex retinal detachment is 8.33 times (crude odds ratio, COR, 95% CI: 1.23 - 56.67, p = 0.0302) more likely to have subsequent proliferative membrane formation. Internal limiting membrane removal can minimize occurrence of cystoid macular edema.12 Membranectomy can be efficiently achieved with forceps (Figure 5) or by using a small-gauge vitrector handpiece on aspiration.

Figure 5: Membranectomy
Beneath the neurosensory retina, subretinal proliferative membranes and bands can form. Contrary to proliferative epiretinal membranes, not all subretinal bands need to be removed. Figure 6 exemplifies a young phakic patient who underwent primary scleral buckle repair with a shallow chronic retinal detachment. The patient had profound subretinal bands posteriorly near the nerve and anteriorly towards the vitreous base. Sometimes subretinal bands involving the macula or limiting the ability to re-attach the retina need to be removed. A small retinotomy with endothermy followed by forceps-assisted removal allows for access and removal of this subretinal pathology.13-15

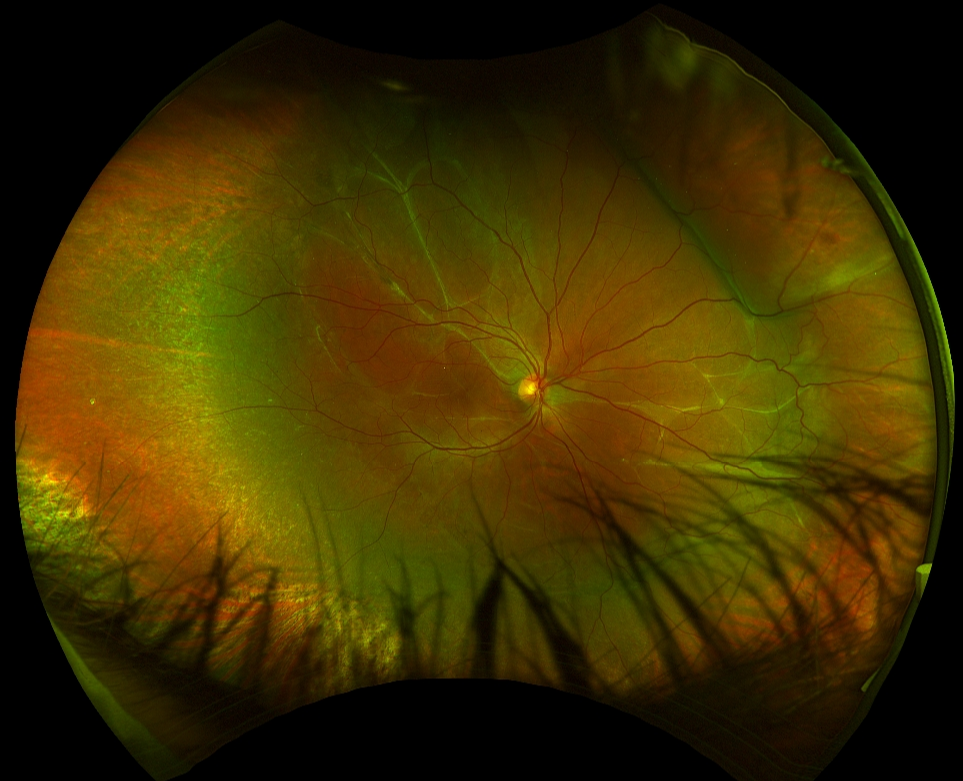
Figure 6: Primary SB with subretinal bands
Conclusions
Retinal detachment repair is a challenging topic for many ophthalmology residents. However, by remembering the five types of retinal detachments (rhegmatogenous, tractional, exudative, combined rhegmatogenous-tractional, macular hole-associated), trainees must first rule in a rhegmatogenous retinal detachment which is best accomplished by finding the retinal break. Rhegmatogenous retinal detachment repair is one of the most common indications for retinal surgery and timing may be critical. When deciding on procedure or surgical technique for retinal re-attachment, optimal management occurs with an individualized approach primarily achieved with primary SB, PPV, or a combined SB and PPV procedure.
References
- Lincoff H, Gieser R. Finding the Retinal Hole. Arch Ophthalmol. 1971;85(5):565
- Pseudophakic Retinal Detachment. Surv Ophthalmol 2003;48:467
- Adelman RA, Parnes AJ, Sipperley JO, et al. European vitreo-retinal society (EVRS) retinal detachment study group. Strategy for the management of complex retinal detachments: the European vitreo-retinal society retinal detachment study report 2. Ophthalmology. 2013;120: 1809-1813.
- Bloch D, O’Connor P, Lincoff H. The mechanism of the cryosurgical adhesion. III. Statistical analysis. Am J Ophthalmol 1971; 71:666–673.
- D'Amico DJ. Clinical practice. Primary retinal detachment. N Engl J Med. 2008;359(22):2346–2354.
- Conart JB, Hubert I, Casillas M, Berrod JP. Results of scleral buckling for rhegmatogenous retinal detachment in phakic eyes. J Fr Ophtalmol 2013;36(3):255-260.
- Storey P, Alshareef R, Khuthaila M, et al; Wills PVR Study Group. Pars plana vitrectomy and scleral buckle versus pars plana vitrectomy alone for patients with rhegmatogenous retinal detachment at high risk for proliferative vitreoretinopathy. Retina. 2014;34:1945-1051
- Totsuka K, Inui H, Roggia MF, Hirasawa K, Noda Y, Ueta T. Supplemental scleral buckling in vitrectomy for the repair of retinal detachment: A systematic review of literature and meta-analysis. Retina. 2015;35:2423-2431
- Eric K Chin, David RP Almeida & James C Folk, Posterior Hyaloid Removal, Ophthalmic Surgery, Lasers & Imaging Retina 2015, 46(4):404
- Almeida DR, Chin EK, Roybal CN, Elshatory CN & Gehrs KM. Multiplane peripheral dissection with perfluoro-n-octane and triamcinolone acetonide. Retina 2015, 35(4):827
- Xu K, Chin EK, Mahajan VB & Almeida DRP. Intravitreal foscarnet with concurrent silicone oil tamponade for rhegmatogenous retinal detachment secondary to viral retinitis. Retina 2016, 36(11):2236
- Kunyong Xu, Eric K. Chin, D. Wilkin Parke III & David RP Almeida, Epiretinal Membrane and Cystoid Macular Edema as Predictive Factors of Recurrent Proliferative Vitreoretinopathy, Clinical Ophthalmology 2017, 11:1819
- Xu K, Chin EK & Almeida DRP. Five-port combined limbal and pars plana vitrectomy for infectious endophthalmitis. Case Rep Ophthalmol 2016, 7(3):289-291
- Robin K Kuriakose, Kunyong Xu, Eric K Chin MD & David RP Almeida, Proliferative Vitreoretinopathy (PVR) Update: Current Surgical Techniques and Emerging Medical Management, Journal of VitreoRetinal Diseases 2017, 1(4):261
- Kunyong Xu, Eric K Chin, Steven R Bennett, David F Williams, Edwin H Ryan, Sundeep Dev, Robert A Mittra, Polly A Quiram, John B Davies, D. Wilkin Parke III, H Culver Boldt & David RP Almeida, Predictive factors for proliferative vitreoretinopathy formation after uncomplicated primary retinal detachment repair, RETINA 2018, Epub ahead of print
