


A chief complaint of double vision can be daunting to even the most experienced optometrist. While diplopia can be caused by a wide range of conditions, CN VI palsy is a common etiology.
Cranial nerve VI, or abducens nerve, palsy is the most common ocular nerve paralysis (1). In the US, it affects 2.5 out of 100,000 adults. It is likely that most practicing optometrists will manage this condition at some point in their career. In this course we will discuss what every optometrist should know about CN VI palsy, from anatomy to diagnosis to management.
What is CN VI palsy?
CN VI palsy is a neurologic condition that usually presents with binocular horizontal diplopia. CN VI innervates the lateral rectus of the eye, which is responsible for abducting the eye. This balances the adducting action of the ipsilateral medial rectus. When this balance is lost the eye will turn in, resulting in diplopia. This diplopia is worse at distance than at near. It also increases when the patient is looking towards the affected side (i.e., if the right CN VI is affected the diplopia will be worse when the patient looks to the right) (2,3).
In order to better understand the causes of CN VI palsy, it is important to review the relevant anatomy.
Neuroanatomy of CN VI
CN VI is a purely somatic nerve. Its primary role is to carry efferent axons to the ipsilateral lateral rectus. It also provides some innervation to the contralateral medial rectus via the medial longitudinal fasiculus, to allow for coordinated eye movements. (4)
CN VI has a long course from the pons, where it originates, to the lateral rectus. In fact, it has the longest intracranial course of any cranial nerve! The course of CN VI can be divided into four portions: the nucleus, the cisternal portion, the cavernous sinus portion, and the orbital portion (3-6).
- The CN VI nucleus is located in the dorsal pons
- The nerve fibers exit the brainstem through the pontomedullary groove
- They travel through the subarachnoid space within a fibrous sheath called Dorello’s canal
- The nerve travels over the petrous portion of the temporal bone towards the clivus
- CN VI then enters the cavernous sinus, near the internal carotid artery
- The nerve enters the orbit through the superior orbital fissure

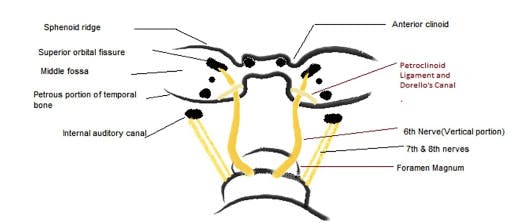
Figure 1: Anatomical landmarks, occipital view. Image credit: "The Six Syndromes of the Sixth Cranial Nerve," Mohsen Azarmina, MD and Hossein Azarmina, MD.

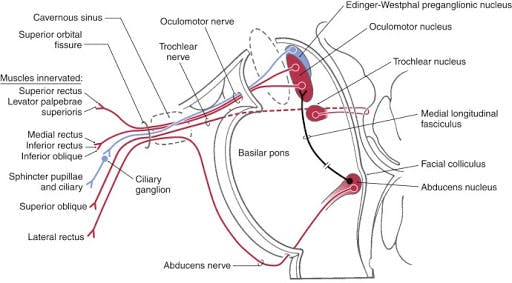
Figure 2: "A Synopsis of Cranial Nerves of the Brainstem," D.E.Haines, G.A.Mihailoff.
Etiology of CN VI palsy
CN VI palsy can be caused by a variety of underlying conditions. While it is rare, a congenital CN VI palsy can be seen. This is usually related to birth trauma and other neurologic conditions (2). Acquired CN VI palsy arises from anything that damages the nerve along its intracranial course. This damage is due to stretching of the nerve, compression of the nerve, or damage to the nerve’s blood supply. Having a general knowledge of the nerve pathway (which you now do!) is helpful to better understand these complications.
In adults, the most common cause of CN VI palsy is microvascular ischemia. Common risk factors of vascular compromise include older age, hypertension, hyperlipidemia, and diabetes mellitus. Diabetes mellitus is most likely to cause microvascular ischemia leading to CN VI palsy.
The CN VI nucleus in the pons may be affected by ischemic stroke, metabolic disease, or demyelinating disease. Intracranial tumors, especially pontine gliomas, are common causes of CN VI palsies in children.
Lesions of the subarachnoid space may also cause CN VI palsies. These may include increased or decreased intracranial pressure, aneurysm, hemorrhage, infection, or inflammation. CN VI is particularly affected by increased intracranial pressure because it is anchored in Dorello’s canal and because of its course along the clivus. Because the nerve travels over the petrous portion of the temporal bone, complicated otitis media or mastoiditis may cause a CN VI palsy.
Within the cavernous sinus, CN VI palsy can be caused by cavernous sinus thrombosis, cavernous sinus fistula, or internal carotid aneurysm or dissection.
Orbital lesions may also cause CN VI palsy. These include trauma, inflammation, infection, and neoplasms. (2-5)

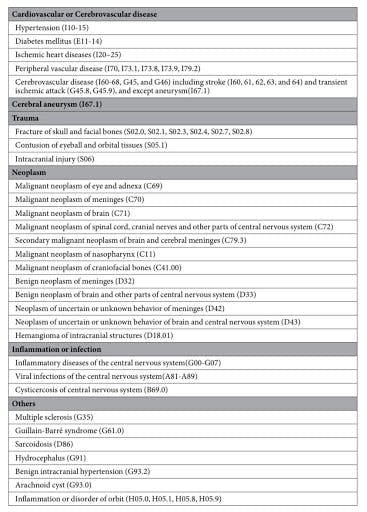
Figure 3: Diagnostic codes for possible comorbid etiologies of CN VI palsy (1).
Diagnosing CN VI palsy
CN VI palsy is diagnosed with a thorough patient history and careful examination. Patients dealing with this condition will often have similar chief complaints and exam findings.
History and physical
As with most conditions, patient history is key to diagnosis. Patients will have a chief complaint of horizontal, binocular diplopia. While most won’t use that exact phrase, they will tell you that they have double vision, the images are side by side, and if they close an eye it goes away. Patients will report that the diplopia is worse during distance tasks, such as watching TV, compared to near tasks, such as using their phone or reading. The diplopia will also be worse when looking to the affected side. Some patients may also develop a head turn toward the affected side to minimize or eliminate their diplopia.
Noting the onset of symptoms is also important for management. Sudden onset suggests a microvascular etiology. A slow onset suggests a compressive etiology. A subacute onset suggests demyelinating disease.
Pertinent medical history includes history of microvascular disease, metabolic disease, infection, inflammatory conditions, trauma, or recent lumbar puncture. Patient’s should also be asked about any other neurologic symptoms. These include headache, vomiting, nausea, hearing loss, and facial numbness.
Any patient with suspected CN VI palsy should have a complete eye exam. Visual acuity, binocular function, ocular motility, and cover testing in cardinal positions of gaze are paramount. If the suspected etiology is trauma, forced ductions should be completed to check for muscle entrapment. Evaluation of the anterior and posterior segment should also be completed. (2,3)
Signs and symptoms
Patients with CN VI palsy will present with an esodeviation in the affected eye. This deviation will be incomitant. The deviation will be greatest when the patient looks toward the affected side, as the eye is unable to abduct. The deviation will also be greater at distance than at near.
Ocular motility testing will show an abduction deficit of the affected eye. Typically the eye is unable to cross the midline. Slow ipsilateral saccades may also be present.
Other signs may be noted, based on the etiology of the CN VI palsy.
- Papilledema if increased intracranial pressure
- Altered sensation along the distribution of V1 and V2 if cavernous sinus lesion
- Nystagmus if pontine glioma
- Horner syndrome if carotid oculosympathetic plexus involvement in the cavernous sinus
The most common presenting symptom of CN VI palsy is diplopia. However, patients may also experience other neurologic symptoms. Headache, pain around the eyes, tinnitus, nausea, and vomiting are associated with elevated or decreased intracranial pressure. Ipsilateral facial weakness, contralateral hemiparesis, and/or sensory abnormalities can be seen in brainstem lesions. Symptoms of other cranial nerve palsies on the same side as the CN VI palsy are indicative of a lesion of the meninges, superior orbital fissure, orbital apex, or cavernous sinus. (2,3)
Laboratory studies and imaging
Laboratory testing and imaging are useful tools in confirming the etiology of a CN VI palsy. The testing ordered should be tailored to the suspected etiology.
Common laboratory studies include:
- Complete blood cell (CBC) count
- Diabetes mellitus testing
- Glucose levels
- Glycosolated hemoglobin (HbA1C)
- Glucose tolerance test
- Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)
Additional laboratory studies to consider:
- Fluorescent treponemal antibody-absorption test, VDLR, or PRP
- Lyme titer
- Antinuclear antibody test
- Rheumatoid factor test
- Thyroid function tests
- Acetylcholine receptor antibodies
MRI imaging would be indicated for the following:
- Younger patients with no vasculopathic history
- Associated pain or other neurologic symptoms
- Trauma
- History of cancer
- Bilateral CN VI palsy
- Papilledema
- If other cranial nerves are or become involved
A lumbar puncture can be considered if MRI results are negative.
There is no universal protocol on the use of neuroimaging for the diagnosis of CN VI palsies. Some practitioners routinely order MRI for all ocular motor palsies. Others will hold off for patients over age 50 with clear vasculopathic risk factors. However, 16.5% of patients with vasculopathic risk factors may develop ocular motor palsies due to other etiologies. (2,3,5)
Differential diagnoses
CN VI palsy causes lateral rectus weakness with resulting ocular motor deficiencies and diplopia. Differential diagnoses include:
- Duane’s retraction syndrome (Types 1 and 3)
- Congenital esotropia
- Thyroid eye disease
- Spasm of the near reflex
- Esotropia with medial rectus contracture
- Myasthenia gravis
- Blowout fracture with medial rectus entrapment
Treatment and management
The treatment of CN VI palsy depends on the etiology. Patients may require coordinated care by a team of specialists including optometrists, ophthalmologists, neurologists, and primary care providers. While the underlying cause of the CN VI palsy will be treated by other members of the patient’s care team, we are uniquely qualified to manage the symptom of diplopia.
Diplopia can be managed in a variety of ways. Prism is a viable option for children and adults. Because of the incomitance of the deviation, the effectiveness of the prism is limited to primary gaze. Educating patients about this will lead to better understanding, less disappointment, and overall improved patient satisfaction. Occlusion using a Bangerter filter or patch will also eliminate diplopia. This decreases the possibility of ipsilateral medial rectus contracture. For children who are patching, it is important to alternate the eye that is patched to reduce the risk of amblyopia.
Surgery is also an option for patients who exhibit a stable ocular deviation over a period of time, usually six months. The most likely complication following surgery is residual diplopia. This can be managed with prism. Botulism toxin can also be used as a temporary alternative to surgery. (2,3,5)
The prognosis of CN VI palsy also depends on the underlying etiology. A recovery rate of 49.6% has been reported in patients with nonspecific etiologies, and 71% in patients with a vasculopathic etiology. Most patients with CN VI palsy due to vasculopathic factors will recover within 6 months. (2,3)
Clinical pearls
“Side by side double vision that goes away when I close an eye” is likely a chief complaint that you will hear at some point in your career. Listening to the patient and taking a detailed history is always the first step. A careful and thorough examination will help to confirm a diagnosis of CN VI palsy. Treating this condition hinges on determining the etiology. That will likely require an interdisciplinary approach and being a member of a team of healthcare professionals. As eye care providers we are probably the first person a patient calls when their vision changes. We have the opportunity to provide our patients with education, support, and appropriate referrals. We might even be able to get out the prism kit!
References
- Jung, E. H., Kim, S., Lee, J. Y., & Cho, B. (2019). The incidence and etiology of sixth cranial nerve palsy in Koreans: A 10-year nationwide cohort study. Scientific Reports, 9(1). doi:10.1038/s41598-019-54975-5
- Triantafilou, D., CO, & Shuh, D. W., MD. (2020, May 11). Abducens nerve palsy. Retrieved May 21, 2020, from https://eyewiki.org/Abducens_nerve_palsy
- Ehrenhaus, M. P., MD. (2019, November 10). Abducens Nerve Palsy (Sixth Cranial Nerve Palsy). Retrieved May 21, 2020, from https://emedicine.medscape.com/article/1198383-overview
- Nguyen, V., Reddy, V., & Varacallo, M. (2020, April 13). Neuroanatomy, Cranial Nerve 6 (Abducens). Retrieved May 21, 2020, from https://www.statpearls.com/kb/viewarticle/17030
- Graham, C., & Mohseni, M. (2020, January 20). Abducens Nerve (CN VI) Palsy. Retrieved May 21, 2020, from https://www.ncbi.nlm.nih.gov/books/NBK482177/
