The journey towards becoming a retina specialist is challenging and humbling, yet very rewarding. On average, it takes 14 years after graduating from high school to become a vitreoretinal surgeon: 4 years of undergraduate education, 4 years of medical school, 1 year of internship, 3 years of
ophthalmology residency, and 2 years of fellowship (1 year if in medical retina). Moreover, the learning never stops. We must remain dedicated to the dynamic, ever-evolving, advancing field of vitreoretinal diseases and surgery so as to provide the highest quality of care to our patients.
My goal in this article is to provide insight into the process involved in becoming a successful retina specialist, with a special focus on making the most of
fellowship education.
Retina fellowship facts and FAQs
Is retina fellowship competitive?
Vitreoretinal fellowships are pretty competitive. In 2019, according to the SF Match statistics, there were 160 positions offered in retina and 123 positions filled. These statistics include both medical retina fellowships and surgical retina fellowships.
How long is retina fellowship?
Medical retina fellowships are one year long, and surgical retina fellowships are two years long.
How do I apply to retina fellowship?
Applying for retina fellowship is done through the SF Match Central Application Service (CAS) and by contacting programs directly to learn about additional materials and requirements.
How to prepare for retina fellowship during ophthalmology residency
The decision to pursue a profession in retina is multifactorial and needs to be well-informed. One must consider short and long-term professional and personal goals. One must account for family, significant other, location, compensation, lifestyle, and professional satisfaction.
Medical education should not be discounted, as the eye—especially the retina—mirrors overall health. By focusing on this delicate, thin, neurosensory tissue of the eye, we cannot forget all the medical knowledge we have accrued.
The retina is the only part of the body where one can directly visualize nervous and vascular tissue in its native state without any invasive maneuvers. No blood draw is needed. No radiographic imaging is necessary. As a retinologist, one can use light and a lens to directly evaluate part of the central nervous system and help optimize a patient’s overall health.
The retina mirrors overall health. Photo credit: Vanderbilt University Medical Center Photography Department
The patient’s history is important and will always be important, but we are privileged in the world of ophthalmology and retina to be able to rely heavily on the physical examination. If a patient can’t reliably communicate or is malingering, a thorough ophthalmic examination can frequently trump a poor history.
I could know nothing about a patient. I could not know their name, age, or sex . . . yet I could still make impactful, even life-changing, diagnoses through a physical examination. Without any knowledge about a patient’s health, I could evaluate the posterior segment and make diagnoses such as HIV, diabetes mellitus, hypertension, choroidal melanoma, choroidal metastases, lymphoma, autoimmune disease, and atherosclerosis, to name a few. As retina specialists, we have the incredible ability to inform patients of their overall health, coordinate care with primary care physicians and other specialists, and help to optimize health and quality of life for our patients.
Take advantage of retina opportunities during residency
It is important to develop a solid foundation in ophthalmology residency. The goal should not be to do as many vitrectomies as possible, but rather to learn the fundamentals of clinical and surgical ophthalmology well. No subspecialty of ophthalmology should be neglected.
Understanding that a macular pucker can cause monocular diplopia, encircling scleral buckles induce myopia, pars plana vitrectomy frequently leads to progression of cataract, and that repeated intravitreal injections may lead to spikes in intraocular pressure and progression of glaucoma—to name a few examples—will make one a more well-rounded retina specialist. A deep understanding of the fundamentals is critical to be the best physician, ophthalmologist, and retina specialist.
During residency, your experience will be dictated to some extent by the number of retina specialists, their expertise, their teaching styles, and their expectations for the ophthalmology resident. Ultimately, the goal is to learn comprehensive ophthalmology well and create a solid foundation to become a consummate, well-rounded physician and ophthalmologist.
That said, making the additional efforts to gain exposure in the subspecialty of your choice makes good sense, as it allows you to better appreciate each part of the eye and how the system works seamlessly in unison when optimized. That is, you're able to view medical and surgical management of patients in the ophthalmology clinic through the lens and perspective of a future retina specialist.
Screening eye exams in the Bronx: Giving back to the community and gaining experience!
When you demonstrate genuine interest and passion, you have the greatest likelihood of being rewarded. It is the ophthalmology resident who is well-read, eager, and facilitates efficient, high-quality patient care, that is more likely to have the opportunity to gain exposure to interesting cases and have the opportunity to do more surgically. You should not be expecting to peel proliferative vitreoretinopathy membranes as an ophthalmology resident, but it is not out of the realm of possibility to be able to perform or at least assist in multiple straightforward vitrectomies and scleral buckles.
Connect with your retina mentors, and stay in touch!
Mentorship in life and in the practice of medicine colors one’s experience and can be transformative. People who inspire and challenge us while doing things the right way have the greatest impact. My parents and my brother have been incredible mentors as model human beings and as physicians. I can recall high school teachers, internal and family medicine attendings during medical school, a group of the finest retina specialists who served as our department of ophthalmology during medical school, a cornea specialist at an away rotation, a refractive surgeon in my home state, several attendings during residency, a handful of retina specialists during fellowship, and many more, all of whom played an important part in my development and equipped me for success. Mentorship facilitates, but it is self-directed learning, the drive to achieve, execution of a plan, and commitment on this arduous journey, that are key.
Learning with Dr. Paul Sternberg! (Photo used with permission)
Remaining in contact with a few close mentors goes a long way. We are constantly dependent on experts vouching for our capacity and competence to move forward. One's own merit and accomplishments only go so far, especially later on in the journey. A strong letter of recommendation or a brief phone call can dramatically alter the course of one's path to becoming a retina specialist. Frequently, these outweigh one’s curriculum vitae no matter how stellar the CV. Along the same lines, an unsatisfactory reference can be the kiss of death to attaining your goal in this small world of ophthalmology—and even smaller circle of retina specialists.
Research, research, research
Research helps us to advance the field and improve patient outcomes. Retina is such a dynamic field that has made leaps and bounds in the past 15 years. The majority of these advances are grounded in the development of new molecules and delivery systems with confirmation of safety and efficacy from well-designed randomized controlled trials. The most prominent breakthrough in the recent past was the advent of anti-vascular endothelial growth factor (anti-VEGF) therapy, which has revolutionized the field. Patients with
wet age-related macular degeneration, for example, no longer have to have their neovascular membranes lasered leaving large, atrophic central macular scars and marked central vision loss or go blind without prompt, effective treatment.
Surgical techniques and systems have also been refined tremendously to allow for efficient, consistent microsurgery. The interplay between research and the practice of retina seems inextricable. In order to remain abreast with the field and afford patients the best opportunities for first-rate care, one must be aware of—if not directly involved in—clinical research.
Surgical training: learn the fundamentals . . . and everything else
In residency, the goal is to learn the fundamentals well so that one can be an efficient, adept vitreoretinal surgeon in the future. You want to maximize your exposure to the retina world but you will have your whole life to continue to build on it.
That said, it’s almost more important to learn everything else really well, because your future exposure to the other subspecialties of ophthalmology may be quite limited. Vitreoretinal surgery overlaps with many other surgical subspecialties of ophthalmology.
Strabismus
Learning to isolate the recti muscles properly and avoid the obliques is important in scleral buckling for retinal detachment repair. Learning how to isolate the muscles atraumatically will lower the risk of extraocular muscle dysfunction, strabismus, and diplopia.
If you end up placing radioactive plaques and removing them in the management of uveal melanoma, you may have to disinsert and reinsert recti muscles depending on the size and location of the tumor. You do not want to inadvertently recess or resect a rectus muscle in the context of brachytherapy, as it can result in strabismus and diplopia.
Cataracts
The most commonly performed surgery by the ophthalmologist is cataract surgery, which also happens to be one of the most commonly performed surgeries in the United States overall. As ophthalmologists, we have the incredible ability to have a significant impact on the lives of many. With cataract surgery, most people note a marked improvement in vision, color vision, depth perception, activities of daily living, and quality of life. Patients are elated to see the vibrance of colors post-cataract surgery.
Learning the techniques and nuances of bimanual cataract surgery help to solidify the foundation for becoming a retina surgeon. Learning to operate the microscope, delicate handling of tissue, using both hands and both feet, toggling between different settings, controlled cutting and aspiration using the foot pedal, and maintaining intraocular pressure and anterior chamber stability, are all important elements to much of ophthalmic and retina surgery.
The cataract surgeon frequently involves the vitreoretinal surgeon when lens fragments get displaced into the posterior segment or when there is zonular dehiscence or instability leading to an unstable natural lens. These are some very rewarding cases, as patients have improvement in floaters, blurred vision, inflammation, and intraocular pressure once the displaced lens material is cleared from the eye.
Intraocular lenses
Primary intraocular lens implantation in the capsular bag at the time of cataract surgery is ideal when feasible and appropriate. It is worthwhile to learn as many techniques of intraocular lens implantation as possible during residency (and fellowship). Perfecting standard phacoemulsification cataract surgery with posterior chamber intraocular lens implantation is the first priority. It is expected that most residents will also learn to place sulcus and anterior chamber intraocular lens implants, but if you have the opportunity to get exposed to and learn techniques of scleral-sutured and scleral-fixated intraocular lens implantation, take full advantage—the earlier the better.
Suturing
One of the earliest ways to develop hand-eye coordination and manual dexterity is from practicing suturing. Many programs now have access to a wet lab where one can practice on cow or pig eyes. There are many other ways to practice; some have used a banana peel, orange peel, or a stiff fabric to practice. Learning to suture well with and without the microscope will pay dividends later on and should not be taken for granted. Whether it’s closing a sclerotomy promptly in a hypotonous eye, getting a good gas fill, or closing the wounds quickly in a case of the dreaded, expulsive suprachoroidal hemorrhage, suturing skills are critical to develop well. In the age of sutureless cataract surgery and sutureless vitrectomy, residents must make a special effort to develop suturing skills well.
Retina Fellowship
When you first see your future on the match website, receive your match letter, or get the phone call from your future program director, it is a whirlwind of emotions. It is exciting and nerve-wracking at the same time. You will leave many of your family, friends, and colleagues to likely relocate to a new city in a new environment with new people and start from the bottom again for a one to two-year stint. On the flip side, the future is bright and you have the opportunity to pursue your passion, gain invaluable experience, impact the lives of many, and become part of an elite group of highly specialized physicians and surgeons.
What is AUPO Certification?
Retina is not governed or regulated by the Accreditation Council for Graduate Medical Education (ACGME). The Association of University Professors of Ophthalmology (AUPO) is committed to the establishment and maintenance of standards of subspecialty fellowship training in ophthalmology. The
Association of University Professors of Ophthalmology Fellowship Compliance Committee (AUPO FCC) certifies retina fellowships based on meeting or exceeding certain standards and program requirements. The American Society of Retina Specialists (ASRS), Macula Society, and Retina Society, support and endorse the fellowship training compliance program of the AUPO.
Representatives of each of the vitreoretinal subspecialty societies established the initial guidelines for vitreoretinal surgical fellowship programs. The ultimate goal of the AUPO FCC is to ensure that fellows complete the program successfully so as to provide competent, safe care for patients. The AUPO aims to protect the integrity of the fellowship process and protect the fellow.
It is important to be mindful of options when applying for retina fellowship. There are many academic and private practice retina fellowships. Some are in compliance with AUPO requirements and others are not. An AUPO-certified fellowship does not guarantee a well-rounded experience in a nurturing learning environment, but it is more likely to adhere to the pre-defined guidelines and provide a comprehensive experience. One must apply and set goals having understood what each retina fellowship provides.
Medical retina and surgical education
The majority of our patient care is in the clinic diagnosing and treating medical retinal conditions such as age-related macular degeneration, diabetic retinopathy, retinal vein occlusion, myopic degeneration, retinal dystrophies, etc. Being a thoughtful clinician and refining examination skills will assure best patient outcomes and help to optimize their overall health.
Vitreoretinal surgery is complex, delicate, fine (mostly) microscopic surgery requiring great manual dexterity, problem solving, and composure. Every case is different and no two patients are the same. Though I wanted to be a part of a field that is mostly black and white (e.g. tear or no tear, detached or not detached, neovascular membrane present or absent), there is still a lot of grey in the world of retina. Every case is a puzzle, especially in patients with history of trauma, uveitis, and/or retinal detachment. Surgical planning, efficient, purposeful movements, anticipating and preparing for complications, and adaptability, are critical to achieve success in vitreoretinal surgery. Things frequently do not go exactly as planned. So, one must remain composed and act quickly when faced with intraoperative hurdles.
It is very important in fellowship to have balance between clinic, surgery, research, and self-directed learning. Some fellowship programs boast 800-1200 primary surgical cases for retina fellows. In my opinion, it is more important to have done a large number of primary cases as long as there is adequate variety of cases and the operating room time is not so excessive that it detracts from one’s medical retina education. Mindful learning is more important than having done a thousand primary cases.
A good goal is 350-500 primary cases including retinal detachment repair by vitrectomy, scleral buckle, or both, vitrectomy for hemorrhage, vitreous opacities, macular pucker, macular hole, tractional retinal detachment, proliferative vitreoretinopathy, and so on.
Uveitis
Uveitis is fascinating and has been associated with numerous factors such as trauma, surgery, infection, genetics, autoimmune disease, inflammatory bowel disease, tattoos, pets, medications, cancer, etc.
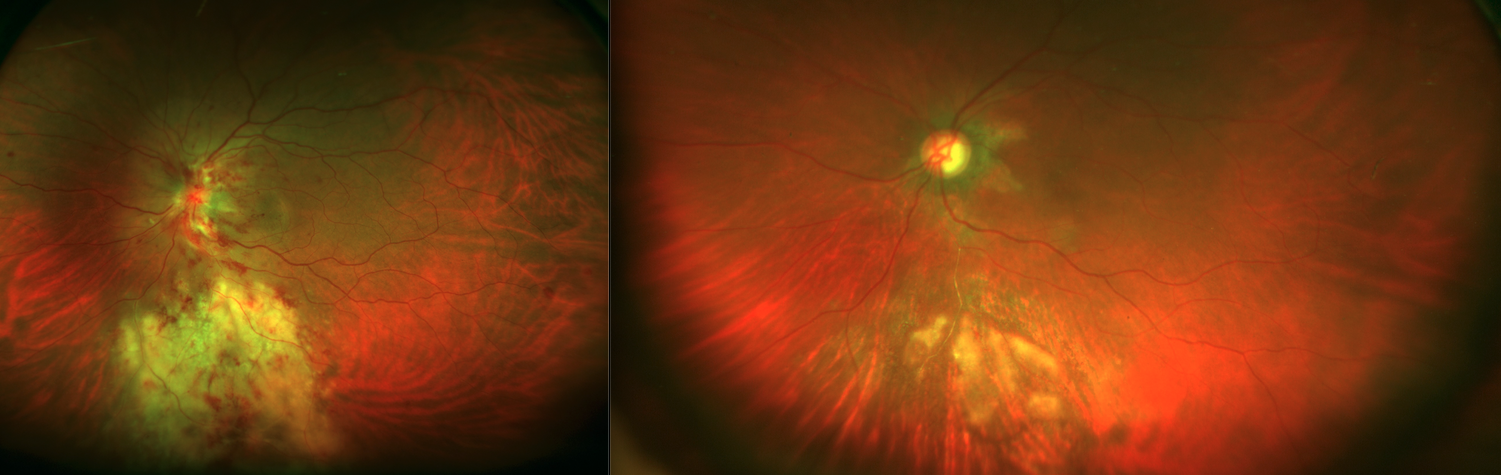
Left: Cytomegalovirus Retinitis in patient with lymphoma. Right: Marked improvement of retinitis and hemorrhages post-treatment.
There is a lot of overlap between uveitis and retina. As a retina specialist, especially in the absence of a fellowship-trained uveitis specialist in the area, we are frequently called upon to diagnose and manage a variety of ocular inflammatory diseases. It is important to obtain a thorough patient history and perform a complete ophthalmic examination so as to guide the appropriate testing for the individual patient. We never want to miss life-threatening or vision-threatening conditions. It is also of critical importance to consider infectious etiologies and avoid blanket treatment with corticosteroids without due diligence.
Injections
Since the advent of anti-vascular endothelial growth factor (VEGF) therapy, there has been a dramatic increase in the number of intravitreal injections performed. Intravitreal therapy is utilized for treatment of neovascular age-related macular degeneration (AMD), diabetic macular edema, proliferative diabetic retinopathy, retinal vein occlusion, uveitis, neovascular glaucoma, etc. Given that this is one of the most common in-office procedures performed by retina specialists, it is more important that we make it a comfortable experience for patients and minimize the risk of post-injection complications, especially infectious endophthalmitis.
Laser
As retinologists, we use laser therapy to barricade retinal breaks as well as occasionally to barricade a localized retinal detachment or retinoschisis. Laser is occasionally used to prevent worsening of non-central diabetic macular edema. It can be used to treat a focal leak in
central serous chorioretinopathy. It is frequently utilized to decrease the vascular drive in ischemic retinal vascular diseases.
Photodynamic therapy (PDT) is a special type of laser therapy performed with a photosensitizing dye to selectively target abnormal blood vessels. PDT has been used to effectively treat central serous chorioretinopathy, neovascular age-related macular degeneration, polypoidal choroidal vasculopathy, choroidal hemangioma, etc.
Cryotherapy
Cryotherapy is a freezing treatment that, like laser, works to create adhesions and seal retinal breaks. It is also used for peripheral retinal ablation in ischemic retinal vascular diseases and to treat certain tumors.
With both laser and cryotherapy, experience will allow one to learn the nuances. It is important to avoid white-hot burns with laser, as iatrogenic breaks and rarely bleeding can result. The biggest challenges with cryotherapy are positioning and avoidance of overtreatment, as it can be quite pro-inflammatory and can increase risk of proliferative vitreoretinopathy. The cryotherapy probe tends to roll along the globe and thus, stability, control, and confirmation before treatment are important. “Shafting,” where the shaft and not the tip of the probe is creating the indentation, can lead to imprecise treatment and risks accidental treatment to the macula.
Pars plana vitrectomy (PPV)
Pars plana vitrectomy (PPV) is the mainstay of vitreoretinal surgery. Surgery, ideally, is like a perfectly choreographed dance. Every step matters. The proper sequence of events allows for smooth transitions and efficiency. From draping to placing the eye pads and shield at the end of the operation, each step affects the following steps. As a fellow, be proactive and learn how to properly position the patient, drape the patient, prepare the eye, place the lid speculum, appropriately place sclerotomies, and perform an efficient vitrectomy achieving the goal of surgery successfully while avoiding iatrogenic complications. Some of the steps such as draping may seem less important but trust that they are all important. For example, improper draping can lead to significant fogging of the lens and make the procedure more challenging. Proper visualization throughout PPV is critical for successful completion of individual steps of the operation. There are many tips and tricks that you will pick up from attendings and colleagues or figure out on your own. Whether it is transiently raising the intraocular pressure to place cannulas when facing resistance, using a dispersive viscoelastic to clear the view when significant corneal edema is present, gentle back and forth movement of the soft tip within a cannula to gain access to the vitreous cavity, using a bent microvitreoretinal (MVR) blade as a pick to elevate a diffuse, taut macular pucker, there are numerous tricks to help when the standard procedure is not adequate.
Scleral buckle
There are some who believe that retinal detachment repair with scleral buckle is not necessary, is less elegant, induces myopic shift, and causes ocular surface symptoms. It is one of the earliest techniques of retinal detachment repair and for many of us, still plays a very important role. With advances in small-gauge vitrectomy, scleral buckle surgery appears to be decreasing and the AUPO requirement for number of scleral buckles has decreased over the last several years. Scleral buckle remains of great value and is useful for primary retinal detachment repair, especially in phakic patients without posterior vitreous detachment, high myopia, extensive lattice degeneration, very anterior retinal break(s), or with retinal dialysis. Scleral buckle is useful for retinal detachment repair in combination with vitrectomy, especially in cases of retinoschisis, proliferative vitreoretinopathy, trauma, recurrent and complex retinal detachment.
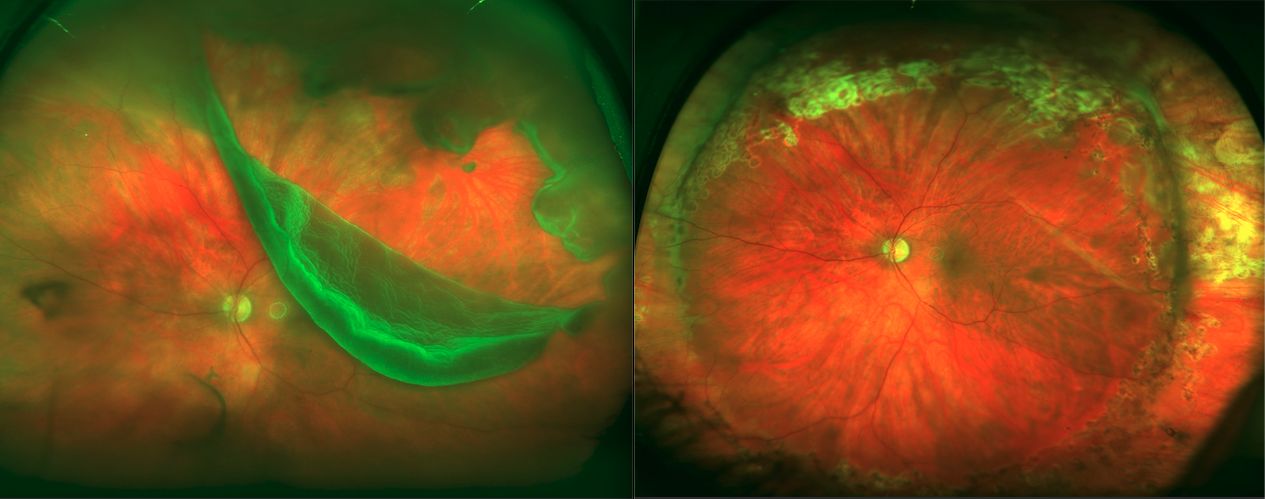
Left: Giant retinal tear. Right: Status post-repair with combined scleral buckle-vitrectomy.
As a fellow, it is worthwhile to learn the fundamentals of scleral buckling well. I would recommend doing as many as primary scleral buckles as possible, as it is a fading art form and it allows one to learn scleral indentation and the principles of retinal detachment repair well. If you do not have the opportunity to do many or any primary scleral buckles, at a minimum, learn the techniques of buckling as part of a combined scleral buckle-vitrectomy procedure. The scleral buckle supports retinal breaks, supports the vitreous base, relieves traction, decreases risk of progression of cataract and preserves accommodation in young patients, and avoids the risk of complications from intraocular surgery. It is an important part of the retina surgeon’s armamentarium.
Intraocular lenses—part two
The vitreoretinal surgeon is frequently called to action when an intraocular lens implant is subluxed, displaced, or fully dislocated into the posterior segment. This can happen in a variety of connective tissue diseases such as Marfan syndrome but more commonly occurs from pseudoexfoliation syndrome or traumatic ectopia lentis.
Doing a thorough pars plana vitrectomy with laser barricade of any retinal breaks in these cases is critical to lower risk of postoperative retinal detachment, especially in trauma cases.
Patient rapport and outcomes
Complications and occasional poor outcomes are inevitable. Some of this is due to advanced disease and delayed presentation for care but some of it happens despite doing everything the right way. Establishing a good rapport with patients and making yourself available to answer questions and allay concerns are important to create a good physician-patient relationship. Some complications are iatrogenic and/or preventable.
Effective communication is key! Photo credit: Vanderbilt University Medical Center Photography Department
Monitoring your patients’ progress over time, especially those with complications or a difficult clinical course, is important to learn from and to hone your skill set.
Setting goals in your retina fellowship
This is one of the most challenging periods and it is easy to get lost in the daily grind and lose sight of the ultimate purpose. Taking the time to clearly define individual goals and tracking one’ s progress over time will pay dividends in the future.
Defining expectations
It is worthwhile to set your own personal expectations as well as clearly identify expectations set by your program. At the beginning of fellowship, meeting with your fellowship program director to discuss expectations will help to ensure that there are fewer surprises throughout your training.
Managing personalities
Whether your program is small or large, you will most likely face a variety of different teaching and management styles as well as varying personalities. During my fellowship, I worked with about eight different retina specialists and numerous other ophthalmologists in a large department, as well as many other physicians in a large academic institution. It is challenging and at times frustrating to deal with varied personalities and management styles. However, there is a lot to gain from the collective experience of many experts who trained at different institutions during different time periods.
Clinical education and self-directed learning
Having reached this point in your life and career, you know what works best for you to learn and retain information. Retina is very visual and a lot of our learning and diagnosis of disease is based on pattern recognition. It is worthwhile to have a reference text and an atlas to solidify your knowledge from seeing patients in the clinic, hospital, or emergency department. Many of us use Ryan’s Retina and Yannuzzi’s The Retinal Atlas or the Gass’ Atlas of Macular Diseases. Personally, I learn best by looking up information promptly as it relates to a specific patient when my curiosity is piqued. I am able to retain that information well with situational associations stored in my memory.
Tools for success
One of the most important goals of fellowship is to have gained the fund of knowledge and experience so that when fellowship is complete, you have a clear plan of action for each patient presentation. That is, you should have an algorithm for work-up and management of all common retinal diseases. These algorithms can evolve and be refined based on the individual scenario but having a general plan for each condition is worthwhile for efficiency and to avoid missing important diagnoses. A standardized work-up and plan of action is especially important in the management of uveitis.
Logs
It is important to maintain a thorough, de-identified log of surgical cases and procedures for your own record, review, and to follow your progress over time. The American Society of Retina Specialists (ASRS) requires a detailed record of your surgical cases. So, try to pace yourself and stay on top of maintaining a good record, as it is challenging to do it all at the end of the year or worse the end of fellowship. I recommend making brief hand-written notes on each case – for example: extent of retinal detachment, location of retinal breaks, macula involvement, type and concentration of gas, complications, iatrogenic injury, sutures used, unusual findings, unusual length of case. It is good to have a physical copy in case of technology glitch or if dictation does not go through for some reason.
It is also a good idea to keep record of all conferences (medical or surgical case conference, fluorescein angiography or imaging conference, journal club, etc.) and what cases or articles were discussed.
Video recordings
One of the greatest ways to learn and hone your surgical skill set is by recording your surgical cases and watching them afterwards to identify areas for improvement. Even better is to discuss surgical cases (with video recordings) with a group of retina surgeons to gain from the experience and guidance of many experts.
Practice on the simulator!
Though the greatest teacher is experience, it is always helpful to practice and to mentally prepare for surgery. Retina surgery is challenging and can be quite exacting and stressful. If you have access to a simulator, you can practice examination of the retina, applying laser, performing vitrectomy, and probably the most useful – membrane peeling. One of the most challenging parts of retina surgery is peeling epiretinal and internal limiting membranes. Early on in fellowship, it is frightening because of the risks of iatrogenic injury to the macula, possible development of scotomata, and other complications such as neovascularization and proliferative vitreoretinopathy. It takes time to develop the skill and you have to be calm, composed, and mindful to effectively and consistently peel membranes. If you allow yourself to become overwhelmed by anxiety or your attending’s stern words, you are more likely to falter, be unsuccessful, and cause iatrogenic injury.
Perfect your multi-tasking
As a retina fellow, it will feel like there are not enough hours in the day to read, learn, practice, teach, care for patients, operate, take call, prepare presentations, log and review your cases, follow your patients, call your patients to answer questions and concerns, write prescriptions, study for ophthalmology board exams, conduct important research, present research, write manuscripts and successfully publish, etc. much less have a social life, stay in touch with family, and sleep. You will have to learn to multi-task and maximize the time you have. Take it all in a stride and do the best that you can while taking care of your health.
On time management and efficiency
There is a huge learning curve but once you get the hang of things, it will be more and more important to improve efficiency. You will have to develop the art of making the patient feel comfortable, examine the patient, document your findings and plan, explain the diagnosis, plan, and prognosis to the patient, answer the patient’s questions, and sometimes perform a procedure all in 5-10 minutes. Taking the time to sit down, providing good eye contact, and listening to the patient, go a long way to make the patient feel comfortable and feel that you spent more time than you did.
Find that work-life balance
Finding balance in retina fellowship is challenging because there is so much to learn and it is so busy. You have to immerse yourself fully in the field to gain the most. That said, make sure to take time for yourself when possible to decompress and take care of your mental health. Try to exercise and stay physically active when possible to also maintain good health.
Customize your techniques
Your attendings may have many biases, preferences, and ideas of perceived higher value. It should be your goal to develop a solid fund of knowledge and take the best from each attending to create a mosaic of useful techniques so that you can become the best and most efficient surgeon you can be.
Journal clubs and evidence-based learning
The world of retina is constantly evolving. It is important to remain abreast with the latest research and advances so as to provide optimal patient care rooted in evidence-based medicine. An important component of retina fellowship is discussing the strengths and weaknesses of important publications and how, if at all, the evidence can be applied to clinical or surgical practice.
Teach others and share what you learn
We are constantly learning. Pay it forward by making a concerted effort to
teach and mentor when possible. This will vary depending on the type of fellowship and how much interaction you have with residents and medical students. I ran a very busy retina clinic at the Veterans Affairs hospital in Nashville and was heavily involved in teaching ophthalmology residents clinically and surgically. I staffed trauma cases with residents. The experience is challenging and rewarding. Helping to mentor the future generation is priceless. We all have the opportunity to learn and gain from those who came before us.
Never take for granted what it is like to be at each stage of this long journey. Try to put yourself in the shoes of those who depend on you and remember that the process is difficult.
Getting ready for your future in retina
Throughout fellowship, keep in perspective the ultimate goal of becoming a well-rounded retina specialist. Think about and discuss options with your colleagues and mentors. Decide on what you foresee being the best fit for your interests and personality.
Some will find it important to do an additional fellowship such as in ocular oncology or uveitis. Some will find academia the best fit and others will decide on pursuing private practice. The great thing is that you can tailor your practice to your preferences.
We must remain committed to lifelong learning to continue to grow and provide the highest quality of care to patients. You will have the incredible ability to teach and mentor the future generation of retina specialists. You can get involved in research to help advance the field and improve patient outcomes.
Whatever your path, enjoy the journey and never take for granted the privileged position you hold as a physician and retina specialist. Take pride in your profession but do not allow your ego to get out of control. The patient is always the most important person in the room and our goal is to improve and protect the patient’s vision. Make a positive contribution to the community at large and have a lasting impact by pursuing your passion.
I have never regretted my decision to become a retina specialist. I am confident that you will find it personally and professionally fulfilling as well.
The Ultimate Guide to Ophthalmology Fellowships
This article is part of our series on ophthalmology fellowships, designed to support new ophthalmologists as you navigate the early days of your specialty. The below guides walk you through each specialty.