


Amniotic membranes, due to their regenerative capabilities, have been used for over a century to treat pathological conditions. In the 1900s, physicians used fetal membranes for skin grafts and treatment of serious chemical burns. It was in the 1940s that De Rotth used both the amnion and chorion for conjunctival reconstruction and Brown used rabbit peritoneum as a temporary patchy for ocular surface burns (1)(11). In 1946 and 1947, Sorsby modified the technique with human amniotic membrane. However, it was not until Kim and Tseng reintroduced the idea of using amniotic membranes to treat ocular surface disease that the idea became popular among the ophthalmology community (6)
Wound healing in adults occurs in three phases: inflammation, proliferation, and maturation. Inflammation involves infiltration of neutrophils and macrophages, followed by lymphocytes. Ideally, neutrophils rapidly undergo apoptosis and are phagocytized by macrophages. In pathological states however neutrophils adopt an extended lifespan, prolonging inflammation and preventing M1 macrophages from clearing out apoptotic neutrophils leading to scarring or inflammation-mediated tissue injury (4).
Wound healing in a fetus is considered “scarless” because fetuses can regenerate tissue rather than form scars (9). When a fetus is injured, there is decreased inflammatory response with fewer inflammatory cells that enter the wound and diminished production of pro-inflammatory cytokines. Amniotic tissue is beneficial for treating patients with chronic inflammation, corneal defects, dry eye, or other ocular surface diseases.
Origin of cryopreserved amniotic membrane
Cryopreserved amniotic membrane created by Biotissue® incorporates human amniotic membrane and umbilical cord processed using proprietary CrytoTek® technology to create an anti-inflammatory tissue that promotes the growth of corneal and conjunctival tissues. Amniotic membrane is comprised of an epithelial monolayer, basement membrane, and avascular stroma that contains nerve, keratinocyte, and hepatocyte growth factor. Each plays a key role in corneal wound healing (2).
Amniotic membrane comes in two types; cryopreserved and dehydrated. Cryopreserved membrane is kept frozen until shortly before it needs to be used while the dehydrated membrane is kept dry and rehydrated shortly before use. Both products can be inserted into the eye similar to contact lenses or sutured in place.
The significance of cryopreserved (Cryo-AM) versus air-dried human amniotic membrane is that cryo-AM is a better substrate for cultivating human limbal epithelial cells. As such, relative to dry amniotic membrane, cryo-AM increases the rate at which limbal epithelium grows out of the palisades of Vogt and release of wound-healing mediators is heightened (12l).
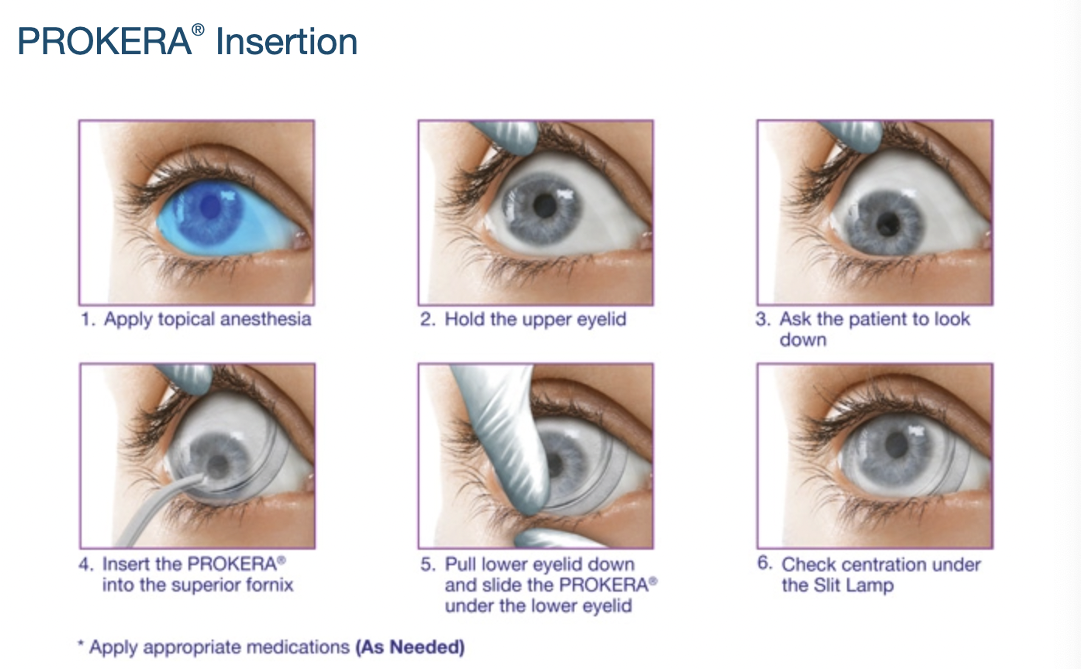
PROKERA®: Corneal Bandage
PROKERA® is a corneal bandage made of amniotic membrane and is used to treat ocular conditions such as recurrent corneal erosions, persistent epithelial defects, herpetic ulcers, filamentary keratitis. There are various types of PROKERA products ranging from PROKERA Slim, PROKERA, PROKERA Clear, and PROKERA Plus.


Each product is designed for a specific purpose—PROKERA Slim contours to the ocular surface and is used for patients who are uncomfortable with a thicker ring. PROKERA Clear is used for monocular cases in patients who must retain visual acuity in the affected eye. PROKERA Plus is a double layer of cryopreserved amniotic tissue used for patients requiring intense, sustained tissue coverage (2).
PROKERA is the only FDA-approved device for use on the ocular surface (3). It can be used to help resolve defects in the cornea, delayed healing, dystrophy, degeneration, and damage. For patients with ocular surface disease, corneal healing is imperative because impaired healing can result in repeated corneal erosions, chronic inflammation, scarring, vision loss, and pain (10). One study found that self-retained cyropreserved amniotic membranes can also be used in the treatment of neuropathic corneal pain due to the production of neurotropic factors that are essential for corneal nerve regeneration and maintenance (7).

For non-healing corneal abrasions, PROKERA creates a scaffold that allows cells to follow it over the area of epithelial defect to allow it to close. The amniotic membrane contains high molecular weight heavy-chain high molecular weight complex (HC-HA), which initiates a number of mechanisms to modulate wound healing and reduce scar formation. HC-HA binds neutrophils, induces apoptosis, promotes macrophage formation (these remove apoptotic neutrophils), and reduces activation of Th-1 and Th-17 lymphocytes which reduce inflammation and decrease scar formation (8).
AmnioGraft®: Ocular Transplantation Graft
AmnioGraft® is an ocular transplant graft used to treat ocular surface conditions like pterygium, excision of tumors, conjunctivochalasis, and chemical burns. AmnioGraft is obtained from placentas donated after birth. It is commonly used for tissue tuck procedures for pterygium. AmnioGraft speeds recovery, promotes healing, decreases surgical time, obtains more cosmetic results, and minimizes post-surgical inflammation (2).
AmnioGuard®: Umbilical Cord Graft
AmnioGuard® is an umbilical cord graft with high tensile strength and thickness; making it ideal for conjunctival, socket, corneal, and eyelid reconstruction. Similar to PROKERA and AmnioGraft, AmnioGuard decreases scarring inflammation and promotes healing. One study found that AmnioGuard supported 100% epithelialization with no complications like wound dehiscence, donor-site morbidities, symblepharon formation, or tears (5).
AmnioGuard can also be used in glaucoma surgery complications such as to create an alternative graft to cover the drainage devices and prevent erosion of the tube. One study used either cyropreserved umbilical cord or pericardium patch grafts to cover glaucoma drainage devices in patients with uncontrolled glaucoma. The stability of the patch graft was monitored by following patients post-op and obtaining their anterior segment OCT. The study found that patients with the amniotic membrane umbilical cord graft had decreased graft thinning and cosmetic appearance compared to the pericardium graft.
References
- Brown, AL. Lime burns of the eye: Use of rabbit peritoneum to prevent severe delayed effects. Arch Ophthalmol. 1941;26:754-769.
- Data on file, Bio-Tissue, Inc., 2012.
- Desai NR. A comparison of cryopreserved amniotic membrane and bandage contact lens in their ability to provide high-quality healing after superficial keractectomy. Rev
- Ellis S, Lin EJ, Tartar D. Immunology of Wound Healing. Curr Dermatol Rep. 2018;7(4):350-358. doi:10.1007/s13671-018-0234-9
- Finger, Paul T., Puneet Jain, and Sri Krishna Mukkamala. "Super-thick amniotic membrane graft for ocular surface reconstruction." American journal of ophthalmology 198 (2019): 45-53.
- Kim JC, Tseng SCG. Transplantation of preserved human amniotic membrane for surface reconstruction in severely damaged rabbit corneas. Cornea. 1995;14:473-484.
- Morkin, Melina I., and Pedram Hamrah. "Efficacy of self-retained cryopreserved amniotic membrane for treatment of neuropathic corneal pain." The ocular surface 16.1 (2018): 132-138.
- Ophthalmol. September 2014:1-6. 2. John T, Tighe S, Sheha H, et al. Corneal nerve regen- eration after self-retained cryopreserved amniotic membrane in dry eye disease. J Ophthal-mol. 2017:6404918 (Epub).
- Rolfe KJ, Richardson J, Vigor C, et al. A role for TGF-β1-induced cellular responses during wound healing of the non-scarring early human fetus? J Investig Dermatol. 2007;127:2656–2667
- Rumpakis J. Amniotic membranes—the perfect cover. Rev Ophthalmol. April 2016:49- 54.
- Sorsby A, Symons HM. Amniotic membrane grafts in caustic burns of the eye. Br J Ophthalmol. 1946;30:337-345.
- Thomasen, H., Pauklin, M., Steuhl, KP. et al. Comparison of cryopreserved and air-dried human amniotic membrane for ophthalmologic applications. Graefes Arch Clin Exp Ophthalmol 247, 1691–1700 (2009). https://doi.org/10.1007/s00417-009-1162-y

