When it comes to ensuring good surgical outcomes, one of the first things an eyecare provider looks for is
Meibomian Gland Dysfunction (MGD). Equipping your practice with tools and treatment options to address MGD before surgery is a way to not only set your practice apart, but ensure your patients are happy and healthy for years to come.
At Empire Eye—an ophthalmic practice in Spokane, WA—we use the
Johnson & Johnson TearScience® suite of products to evaluate gland function and treat MGD. With these products and the workflow we’ve installed in the practice, we’ve seen an increase in happy patients, better collaborative care, and good surgical outcomes.
6,10Dr. Claypool and Dr. Kontos are paid consultants for Johnson & Johnson Vision.
Hear from Dr. Claypool and Dr. Kontos on how they practice collaborative care at Empire Eye!
MGD and your patient population
Meibomian gland dysfunction can present in various levels and eye care professionals (ECPs) will likely only continue to see more of it as our environments both at home and work become increasingly dependent upon immersion in technology and screen-use.1 Single studies have shown the prevalence of meibomian gland dysfunction in:
- Up to 86% of patients with dry eye2
- Up to 39% of asymptomatic patients3
- 80% of glaucoma patients taking long-term anti-glaucoma medications4
- 63% of pre-cataract surgical patients5
Although MGD may be increasingly prevalent in our patient populations, it can be challenging to identify. Too often, ECPs may wait for patients to complain of symptoms rather than proactively testing and searching for it.
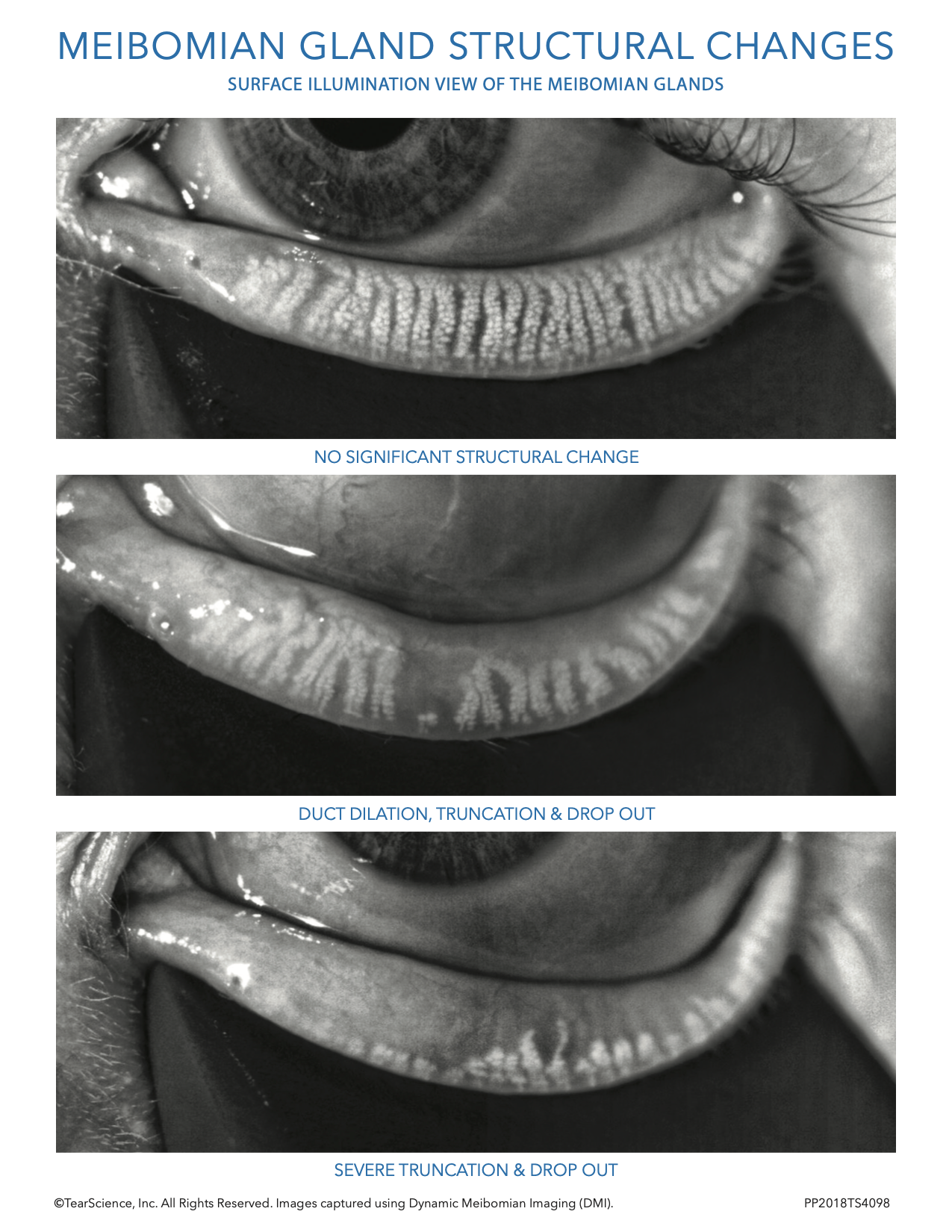
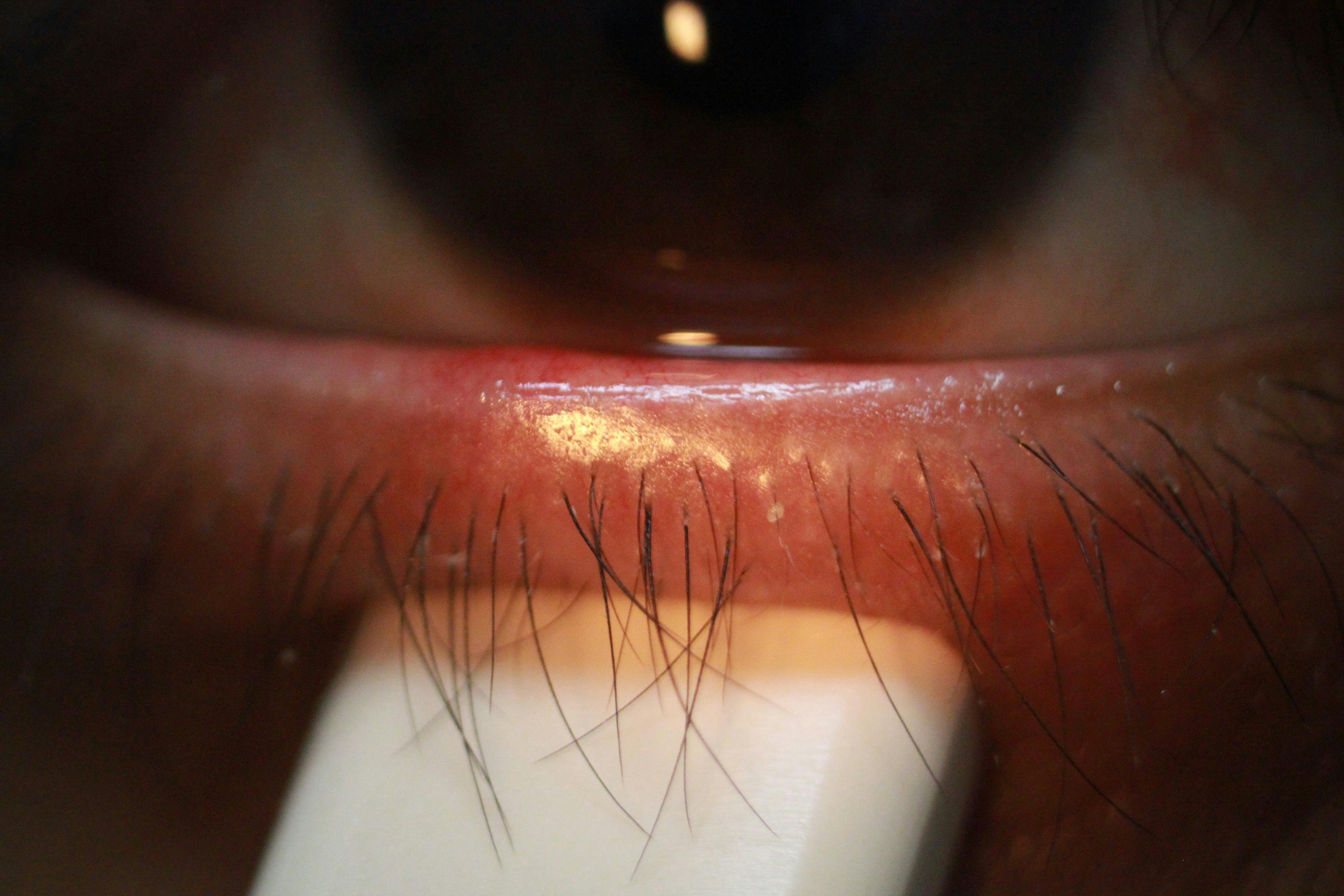
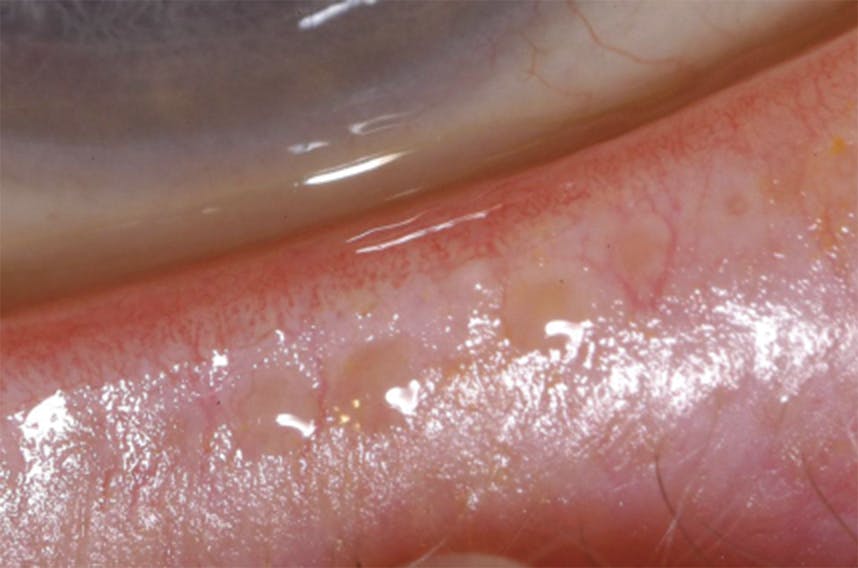
MGD can be difficult to identify due to its co-mingled nature with other forms of Ocular Surface and Dry Eye Disease.2 Separating MGD from these diseases is paramount for treating it properly. The two critical characteristics that ECPs should look for when determining if MGD is present are gland structure and function—not symptoms.
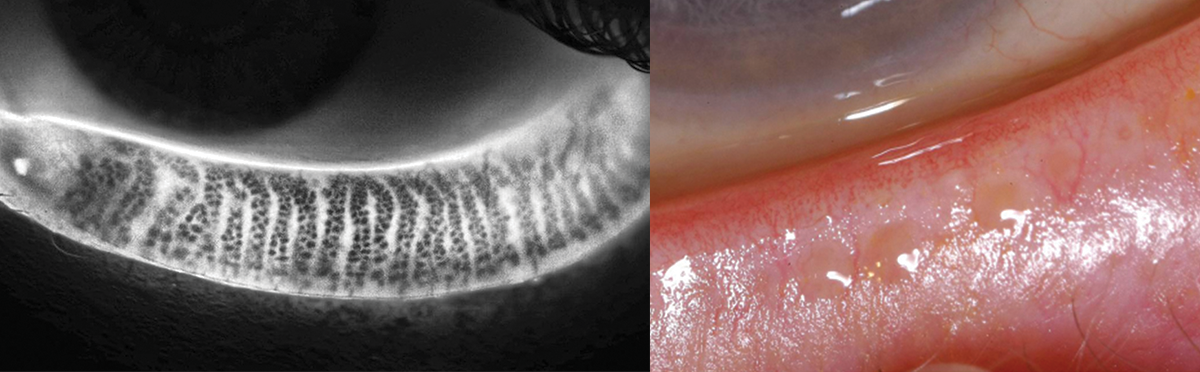
Left: Transillumination show no signification structural change; Right: Testing gland function to see clear oil. Images for illustrative purposes only.
Everyone who presents in our practice is imaged with meibography, especially those cataract surgical patients who are presenting for premium IOLs. This gives us an inside look into structure and whether there is any visible structural absence. If you can identify this ahead of time, you can plan properly for treatment, particularly in patients presenting for surgical care.4 When it comes to assessing gland function, the device we rely on is the TearScience® Meibomian Gland Evaluator (TearScience® MGE). By using this device and applying a consistent pressure to the glands, it can assist in identifying if the patient’s glands are functioning properly. Using meibography to assess structure and the TearScience® MGE to assess function, you can quickly identify gland issues.
TearScience® Meibomian Gland Evaluator (MGE)
In more advanced cases of MGD, we also investigate the presence of inflammation in the tears. In these instances, we like to leverage InflammaDry (Quidel). Based upon our findings, it will clue us in as to whether or not we need to consider additional topical therapies.
Collaborative care for cataract patients between an MD and OD
When it comes to offering collaborative care for cataract patients between an MD and an OD, there are a few things that ODs can do in order to ensure a smooth process.
In our practice, the language we use most often is “preparing the eyes for surgery.” In many cases, a little bit of therapy goes a long way, and we educate patients on proper eye hygiene, hot compresses, and other therapies they can perform at home. For patients presenting with MGD, we recommend
TearScience® LipiFlow® before surgery.
As an independent optometrist, preparing patients for surgery and spending the time on patient education is of tremendous value to the surgeon, but also to the patient. If a patient presents for a surgical evaluation only to hear for the first time they have another condition that needs treatment, it can create an uncomfortable situation for all parties involved.
If the independent optometrist doesn’t have the technology or resources to fully evaluate and manage a patient’s MGD, it can still be immensely helpful to educate their patients on the common treatments that could occur prior to surgery or afterwards. It makes patients happier and more willing to continue treatment when they know that the problem was already there.
When the patient has had their conditions explained to them before treatment, patient compliance and satisfaction are improved. Educating the patient on the condition and informing them that they might need treatment for it ahead of time can go a long way in building that trust and relationship between the referrer, the patient and the surgeon.
Hear from Dr. Claypool and Dr. Kontos about how they manage dry eye patients through collaborative care
Addressing dry eye and treating MGD before cataract surgery
In 2019, the ASCRS Cornea Clinical Committee introduced consensus-based clinical practice guidelines, which acknowledged the importance of screening for and addressing visually significant ocular surface disease due to its potential direct adverse effect on visual quality and acuity both pre- and post-operatively.6 We see this in the literature and in our practice every day. Today, leading eye care providers are increasingly recognizing the importance of healthy meibomian glands in managing the integrity of the ocular surface.
This is especially important for those patients preparing for eye surgery. Without treatment or intervention, tear film and gland dysfunction can advance and increase causing poor visual outcomes and consequently reduced patient satisfaction. Often, a patient’s MGD will have gone undiagnosed, and will only be discovered when they come in with a complaint of degrading vision that they assume is due to a cataract. Often, they will not be aware that their MGD is impacting their vision—or that, untreated, it will have deleterious effects on their surgical outcomes. Untreated MGD can lead to recurrent corneal erosion, corneal scarring, and other ongoing problems.6,13
Treating MGD before cataract surgery is a great way to support better surgical outcomes. We know that when the tear film is disrupted, which we can understand through corneal staining and other means, IOL calculations can be inaccurate. An unstable tear film impacts surgical planning—whether that means the choice of IOL, the IOL power, or any aspect of the surgery itself. This is why it’s so crucial to address MGD before surgery. Similarly, in those patients who present for laser refractive surgery, healthy glands and a stable tear film are vital for optimal outcomes.
In addition, failing to treat MGD before surgery can result in new and more difficult problems—not least an erosion of patient trust. Patients often don’t have context for accepting ongoing care as their new normal, and if MGD is left untreated, you might be denying the patient the full benefit they could be receiving from the surgery. Better outcomes mean more satisfied patients, which can also have a positive impact on your practice. Recognizing issues with glands and tear film can also help you manage patient expectations ahead of time, so you and they are not caught by surprise.
Finally, identifying MGD as early as possible in the disease state will enable early intervention. Early intervention for any disease typically offers a less complex treatment approach.
Identifying MGD before surgery or afterwards: Patient case studies
*The information contained in a case report is anecdotal and may not be assumed to be generalizable to the larger clinical population. Anecdotal findings may or may not have been verified in randomized controlled clinical trials. The findings should be considered particular to the individual case reported here.*
Patient #1: Pre-surgery
In March 2020, a patient was referred to us for cataract surgery. During the slit lamp examination, we also tested for gland function and determined she had an advanced stage of MGD. Her chief complaint was problems with blurry and unclear vision; the patient reported avoiding driving at night in unfamiliar territory and noted that the bad vision had been going on for at least a year. She was a -7.00 myope currently wearing Acuvue® Oasys contact lenses, who showed interest in receiving an advanced technology lens.
Though she made no complaints of dry eye symptoms to either her referring optometrist, or in our ophthalmic exam, her completed SPEED questionnaire score was 18/28, even while wearing a contact lens designed for moisture. Because of her interest in an advanced technology lens, meibography was performed as part of the pre-cataract surgery workflow so we could have a better understanding of her overall ocular surface health. Her images showed severe gland drop out OU. During the slit lamp exam, we also tested for gland function and determined she had an advanced stage of MGD.
Severe gland dropout OU shown in meibography
Aggressive therapy, including TearScience® LipiFlow®, was recommended so we could quickly address her MGD prior to surgery. We provided education about her disease and the need for long-term care even after surgery. The patient was relieved to hear she had treatment options like TearScience® LipiFlow®, and had assumed her dry eye symptoms were normal. On the same day as the consult, she received the TearScience® LipiFlow® treatment, and her surgery with a premium lens was scheduled.
After her 1-day post-cataract surgery follow-up appointment, she had a new SPEED score of 8 (improvement from the original 18). Her original TearScience® MGE measurements for gland function revealed 2 functioning glands OU with inspissated meibum. After her TearScience® LipiFlow treatment®, gland functioning had improved to 4 functional glands OU. Her visual acuity was 20/20 OD/OS, with great near and distance vision. She was pleased with both her visual outcome and overall eye comfort.
Though we were able to address her MGD before surgery, the patient presented with advanced disease state that will require long-term management to maintain ocular surface health & comfort.
Patient #2: Post-surgery
Contrast this patient's experience with another case: in October 2019, a 93 year old female patient presented to our clinic with chief complaints of glare and difficulty reading, and mild complaints of watering and irritation of the eyes. She had best corrected vision of 20/50 due to grade 3 nuclear sclerosis.
Meibography performed October 2019 during initial cataract consult.
Cataract surgery was performed in November 2019. The surgery was uncomplicated, and the patient was initially happy with her comfort and vision following surgery. However, over the next two weeks, the patient reported constant severe foreign body sensation OU with limited relief from artificial tears. The patient had grade 2 corneal staining OU. She regretted the surgery, and reported feeling like it had made her life miserable as her discomfort was now severe, and her depression increased as her dry eyes were now keeping her from functioning. Ointments, warm compresses, topical steroids, oral doxycycline, prescription dry eye drops and more aggressive lubrication were prescribed with limited relief over 6 months with several visits mixed in.
The patient had grade 3 to 4 MGD with two functioning glands on each lower eyelid (two cloudy OD and one inspissated, one cloudy OS). Meibography demonstrated 75% visible gland atrophy OU. I showed the patient the difference in gland atrophy, offered TearScience® LipiFlow®, and the patient considered it for several months before agreeing to the treatment in June 2020.
Six weeks following treatment, the patient noted better comfort after TearScience® LipiFlow®. She was still struggling to read for long periods of time, but was happy to finally notice some improvement after six months.8 Corneal staining had dramatically improved from grade 2 SPK to trace OD and trace to +1 OS. Glands doubled in expression (now had four open OU - 4 cloudy OD and 3 cloudy and 1 inspissated OS) and SPEED score improved from 27 to 22.
This was the happiest I had seen the patient in 6 months and was excited for the improvement as well. With continued therapy and ongoing management, I expect her to continue to improve.
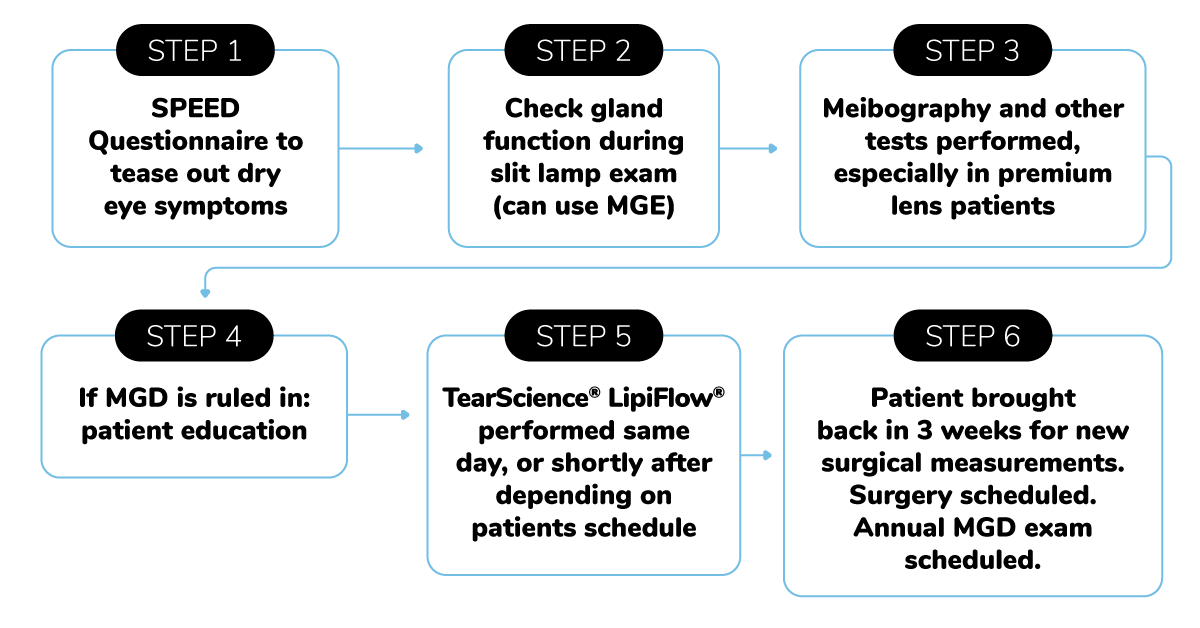
Key Takeaways:
- SPEED questionnaires can help pull out symptoms of dryness that patients may assume is normal
- Check patients gland function during your slit lamp exams for a quick insight into their ocular surface health
- Meibography can be a great tool to better understand health and educate the patient
The impact that treating MGD can have on your surgical patients
One of the most common complaints I’ve seen from cataract patients whose MGD was left untreated before their surgery is that they are still experiencing vision loss post-surgery. They find they are unable to read for long periods of time. While we know that it’s because their tear system is degraded, for them, it’s the same issue but a different cause.
So even if—for whatever reason—we can’t treat MGD prior to surgery, it’s absolutely crucial to discuss the potential impact of not treating it with patients before surgery. That way, if they don’t receive the outcomes and success they expect, the next level of treatment does not come as a surprise.
One could argue that MGD is a very overlooked problem. It is easy to see dryness and note it, but not really do anything about it. Sometimes, patients don’t suffer immediately from it, and therefore, you can fall into the trap of convincing yourself that it doesn’t need to be addressed. This is why assessing even our asymptomatic patients’ glands structure and function is so critically important. Addressing MGD, and doing so in a serious way, makes the patient feel that they're being listened to, that they're being paid attention to as far as what the issues that are bothering them are. This results in a more satisfied patient when they come through the other side.
These are the patients who become very loyal to our practice, the ones we continue to see, and the ones who refer a lot of people in. Having advanced tools and therapeutic instruments really helps differentiate our practice as well.
Since we started treating MGD at our practice, our surgical patients have experienced far fewer residual refractive errors. Overall, the number of refractive touch ups or surgical retreatments have dropped by 50% since we have begun treating MGD before surgery.
Furthermore, it makes surgery and surgical planning much smoother. With all of the ocular imaging equipment we use to assist us, our planning can still be stymied by the way tear film degradation and severe MGD disrupts accurate measurements. It doesn’t matter whether your equipment is top-of-the-line or the least expensive on the market: the accuracy you’re getting when a patient’s MGD is generating bad information is going to be poor.
Patient expectations for cataract surgery are extremely high—as ophthalmologists, we’ve created high expectations for ourselves, and usually we meet them! However, in order to live up to them, we need to think about all of the factors that affect surgery outside of the operating room.
Why invest in technology like TearScience® LipiFlow®, TearScience® LipiView® II, and TearScience® LipiScan®
There are many ways to treat MGD and a variety of reasons as to why investing in technology is important and worthwhile. Conservative therapies are often the first line of treatment. Hot compresses, lid hygiene, and various topical treatments are all highly regarded as the first line of therapy. The issue is, as we all know, that patient compliance with home therapy can be suspect.
That’s where robust technologies like TearScience® LipiFlow® come in. When it comes to surgical intervention, we typically want an efficient approach to treating MGD for optimized surgical outcomes. In these cases, TearScience® LipiFlow® is invaluable.
TearScience® LipiFlow®
TearScience® LipiFlow® takes twelve minutes for a bilateral treatment, and prep time—plus tech time—is minimal.
Patient undergoing TearScience® LipiFlow®
Unlike home therapies and hot compresses, which thin the oil obstruction but don’t fully remove it, TearScience® LipiFlow® is indicated to actually remove obstructions, and unclog glands, increasing OSDI symptom scores three-fold.8 Additionally, it is an automated technology that is extremely efficient, consistent and reliable, using simultaneous vector thermal pulsation (VTP).
At our clinic, TearScience® LipiView® II fits in the first stage of patient education. TearScience® LipiView® II analyzes the patient's tear film, lipid layer thickness, partial blink patterns, and allows your technicians to capture gland images. We use this imaging when explaining our treatment plans to patients. The visual aid is an immense help in educating patients on their eye health and how we plan to address it.
In addition, the learning curve for our technicians was much easier than many other imaging technologies out there.12 We’ve found that the TearScience® LipiView® II and TearScience® LipiScan® technologies offer a simple user experience without compromising image quality, which has really enhanced our practice efficiency.
MGD patient selection and efficient patient education
Utilizing this technology first begins with identifying the right candidate. We have our patients fill out questionnaires and perform a full lid evaluation with imaging. A good candidate for TearScience® LipiFlow® is an adult patient who has MGD or dry eye disease.
In terms of presenting TearScience® LipiFlow® to patients, we begin the conversation by discussing their intake questionnaire and reviewing their meibography images with them. If they’ve reported symptoms, it is easier to make this connection and help them understand why they are experiencing discomfort and how their lids are playing a role.
What many people don’t realize is that our tears can be even more complex than our blood. In order to protect the eye and nourish the cornea, the tear film has evolved to be extraordinarily complex, and can’t be easily duped by artificial tears. I tell patients my goal is to get their own natural tears to do their job. I explain to them that there is only so much artificial tears can do and it doesn't treat the root cause of the problem, which in the majority of cases, is poor gland expression or lack of structure.
Our next step is to put together a narrative for them to help them understand why MGD is so important to treat prior to surgery. When this comes up, we explain to our patients that when the tear system is not as strong as it ought to be, that will have a huge, negative impact on how well they see after surgery. The goal of cataract surgery, of course, is to improve vision, and if this other issue isn’t addressed, the surgery will not meet their expectations.
For many patients, this might be the first time they’ve been told about their MGD as a problem, and not just a fact of life. Often, they’re referred to us for cataract surgery, and they understand this issue—but now there’s something else for them to deal with.
While hot compresses and other at-home methods are often the first line of treatment, ultimately these are ineffective options when addressing gland structure and function, particularly when obstruction is present. TearScience® LipiFlow® removes the obstruction, treating the cause of the problem, while artificial tears and heated therapies only treat the symptoms. In our clinic, we’ve seen that at six months, TearScience® LipiFlow® has a substantially better rate of longevity when compared to heated therapies.7
The other thing to understand is that while this therapy is effective, it addresses one problem patients might have among many. You need to be having conversations with your patients throughout this treatment, informing them that they may need additional therapy afterwards, particularly for those who present with MGD and components of aqueous deficient dry eye or signs of severe inflammation. These patients may not only need TearScience® LipiFlow® treatment, but could potentially need anti-inflammatory treatments as well to help tackle their other issues.
Of course, addressing the root cause of the issue takes time, no matter how efficient your workflow is. TearScience® LipiFlow® may take less than twenty minutes of chair time, but that’s twenty minutes longer than it takes to hand a patient a bottle of artificial tears and call it a day. Choosing to take that time to get to the root cause of the problem is a paradigm shift. This is why one of the biggest challenges of treating MGD lies in patient education.
The entire patient education process begins from the moment they walk in the door and go over their patient history with a technician. Our technicians show patients the results of their imaging, and we walk them through the options that they have based on our clinical findings. Every member of the team has a crucial role in educating patients and helping them understand their diagnosis and the options available to them.
Team efforts: how staff roles and responsibilities can simplify patient education
We strongly recommend this treatment to surgical patients with MGD, and have integrated it into our overall workflow. Our initial intake questionnaire identifies candidates for this treatment, and our technicians go from there.
We used to use the Ocular Surface Disease Index (OSDI) questionnaire, which is the gold standard, but it’s very long and cumbersome from both a clinical and patient perspective. We use the Standardized Patient Evaluation of Eye Dryness (SPEED) Questionnaire now, because it’s a very simple eight question questionnaire that has been shown to be extremely accurate—and less frustrating for patients.
Additionally, using the SPEED Questionnaire during follow-up appointments allows you to show your patient the progress they’ve made with regards to their dry eye with MGD. Many times patients don’t necessarily feel the difference, even though their questionnaires and gland function will show a marked change.
In our practice, each patient receives an initial intake questionnaire, and if they mark anything that indicates signs of dry eye disease—watery eyes, red eyes, burning eyes—they will have meibography done at the same time as the autorefractor. And right next to the tools, we have a screen where patients can see their meibography report and how it compares to examples of glands showing normal to severe gland drop out on the wall. The tech is then able to show them the comparison immediately, and patients get a brief bit of education with their imaging.
Showing patients their meibography report is integral to patient education. Images for illustrative purposes only.
This starts the conversation, and takes a bit more time on the technician’s side in the front end, but it saves an enormous amount of time in the back end. The technician is able to discuss the patient’s symptoms briefly and bring up the source of them, whether that is from gland blockage or loss, and will explain a bit about the function of the meibomian glands using the visual aid. Depending on the technician and their knowledge and comfort level, they’re often able to do more patient education and answer questions, as well as introduce the TearScience® LipiFlow® technology as one potential treatment option the doctor might discuss.
Our techs all know that even just taking five minutes to bring up how the tear system impacts vision with the patient is immensely helpful. We’ve worked this into the process techs go through when taking patient history, and they’re trained to listen for the kinds of patient responses that will throw up these flags, and begin the initial discussion with the patient while marking it on the notes for the doctor.
This isn’t where our team stops, though. Once the doctor has discussed the upcoming surgery with the patient, our surgical coordinator will go through everything one last time with them. We used to have a dry eye or a lens counselor come in afterwards to answer questions, and that’s a great option for really busy surgical practices. And the surgical coordinator and the counselors are trained to be especially cautious, because they’re the last chance to catch these issues before surgery.
Presenting the costs associated with treatment
Cost of treatment can be a delicate conversation to have with patients who you believe are good candidates for TearScience® LipiFlow® treatment. The key to helping them understand is by discussing how the treatment works, and why you believe it will likely be beneficial.
We talk about out of pocket costs and tell patients that this procedure is not covered by insurance. We reference other treatment options and therapies and create a comparative matrix that shows expenses over time to help patients better understand the true costs of the treatment.
Finally, for those surgical patients with MGD, we combine the TearScience® LipiFlow® treatment with their individual surgical plan. In the end, it is all about presenting the true value of the treatment and spending time on patient education, and if patients can manage the cost, usually the decision is an easy one for them to make.
Integrating TearScience® LipiFlow® into the exam workflow
Our workflow for using these products depends on the purpose of the patient visit. MGD and treatment is presented for every dry eye consult, of course, but it can be brought up other times as well depending on patient need.
Identifying MGD in pre-surgical patient workflow
I check basic gland function on every patient, including those coming in for their annual appointments, even if they’re asymptomatic. For many, it might just be a quick push with my thumb, but the only time I don’t evaluate the lids is for a quick LASIK or cataract post-operative checkup. For LASIK or dry eye evaluations, and comprehensive eye exams where the patient has any kind of symptoms, I’ll make sure to check gland function with the TearScience® MGE across the entire lower lid.
Checking gland function: no oil
Checking gland function: clear oil
I’ll always explain to them what I’m doing and why. The oil glands that run across the lids lubricate the eye and allow us to have clear vision. And while I’m explaining this, I will press on the glands, and describe my findings to the patient—it should be clear oil, I’ll say, but it might look more like Crisco or liquid cheese. And that comparison is very understandable!
At that point, I’ll tease out any symptoms that the patient has had, because usually they will be experiencing some symptoms, but not always. It’s very important to tie symptoms to the cause, particularly when it comes to this kind of out-of-pocket treatment. I will explain how and why MGD causes these kinds of symptoms, and what the treatment options are.
I always start my explanation with TearScience® LipiFlow®, because I truly believe this way of treating the problem at its source is the most effective. It really is an optimal way to treat this condition—other treatments used to control symptoms, such as prescription drops, I’ll explain, will often address symptoms without directly fixing the cause, which is gland blockage.11 I will go over all of these options very thoroughly, however, because this is the point where cost comes up.
Because TearScience® LipiFlow® is usually not covered by insurance, it may not be affordable for all patients, and they cannot feel like they are receiving subpar care because of that. We’ll discuss all of the options available to them so they can make an educated choice. I’ll also explain that with the continuously advancing technology, this treatment is much cheaper than it used to be—and when it comes to surgery, we’ll often integrate it with patients selecting premium lenses. We like to do that in our clinic because these are non-covered procedures, and we really want them to get the highest surgical benefit possible.
I’ll let the patient know that while we can perform this treatment immediately in clinic, they’re not required to make the decision today. If they’re on the fence, I’ll make sure to set them up with a home treatment regimen, and they can decide if they want to pursue this treatment at a later time. You can’t overpromise, and you can’t force your patients into a decision.
For many of our patients, it’s not an issue because they’ve been recommended by friends or family, who’ve already told them about the treatment and the cost. We do have a higher patient treatment rate than ever, both because of the growing public awareness around dry eye, and also because patients who go through this treatment are extremely likely to recommend it to their friends and family.
Ultimately, with appropriate education about their condition and treatment options, I would say 60-70% of our candidate patients will choose the TearScience® LipiFlow® treatment. This includes patients who agree to the treatment in the first place, but also includes those who will return after their initial appointment for the treatment.
After treatment, we see our patients for a follow up appointment two months after TearScience® LipiFlow® in order to track gland and symptomatic improvement. After that first follow up, we see them roughly every six months after that. Some patients we’ll only see once a year—others we’ll see more often depending on symptoms and disease severity.
Why to consider adding this technology into your practice
Incorporating advanced technology in the practice is a great way to not only help patients, but generate new revenue for your practice. Additionally, it gives you the ability to learn and understand more about this disease process.
The pathway has been paved by other doctors: we’ve found systems that work in our practice and enhance surgical success. It takes effort on the part of the practice, but in the end it truly is worth it. If you are dedicated to adopting new technologies in your practice that can provide patients with better treatment options, and rally your staff behind it, you’ll see incredible gain both in terms of patient satisfaction and improved patient care.
INDICATIONS AND IMPORTANT SAFETY INFORMATION for LIPIFLOW® Thermal Pulsation System
Rx Only
INDICATIONS
The LipiFlow® Thermal Pulsation System is intended for the application of localized heat and pressure therapy in adult patients with chronic cystic conditions of the eyelids, including meibomian gland dysfunction (MGD), also known as evaporative dry eye or lipid deficiency dry eye.
CONTRAINDICATIONS
Do not use the LipiFlow® System in patients with the following conditions. Use of the device in patients with these conditions may cause injury. Safety and effectiveness of the device have not been studied in patients with these conditions.
- Ocular surgery within prior 3 months, including intraocular, oculo-plastic, corneal or refractive surgery procedure
- Ocular injury within prior 3 months
- Ocular herpes of eye or eyelid within prior 3 months
- Active ocular infection
- Active ocular inflammation or history of chronic, recurrent ocular inflammation within prior 3 months
- Eyelid abnormalities that affect lid function
- Ocular surface abnormality that may compromise corneal integrity
PRECAUTIONS
The Activator or Activator II (Disposable) may not fit all eyes, such as eyes with small palpebral fornices.
Use of the LipiFlow® System in patients with the following conditions may result in reduced treatment effectiveness because these conditions may cause ocular symptoms unrelated to cystic meibomian glands and require other medical management. Safety and effectiveness of the device have not been studied in patients with these conditions.
- Moderate to severe (Grade 2-4) allergic, vernal or giant papillary conjunctivitis
- Severe (Grade 3 or 4) eyelid inflammation. Patients with severe eyelid inflammation should be treated medically prior to device use.
- Systemic disease conditions that cause dry eye
- Taking medications known to cause dryness
- Esthetic eyelid and eyelash procedures
In addition, the treatment procedure may loosen previously inserted punctal plugs, which may worsen the patient’s dry eye symptoms.
ADVERSE EFFECTS
Potential adverse effects that may occur as a result of the procedure include, but are not limited to, the onset or increase in:
- Eyelid/eye pain requiring discontinuation of the treatment procedure;
- Eyelid irritation or inflammation;
- Ocular surface irritation or inflammation; and
- Ocular symptoms (e.g., burning, stinging, tearing, itching, discharge, redness, foreign body sensation, visual disturbance, sensitivity to light).
Potential serious adverse events (defined as permanent impairment or damage to a body structure or function or necessitates medical or surgical intervention to preclude permanent impairment or damage to a body structure or function) that are not anticipated because of the device mitigations to prevent occurrence include:
- Thermal injury to the eyelid or eye, including conjunctiva, cornea or lens;
- Physical pressure-induced injury to the eyelid; and
- Ocular surface (corneal) infection.
ATTENTION Reference the LipiFlow® Thermal Pulsation System Instructions for Use for a complete listing of indications, warnings, and precautions.
INDICATIONS AND IMPORTANT SAFETY INFORMATION for LIPIVIEW® II Ocular Surface Interferometer
Rx Only
INDICATIONS
The LipiView® II Ocular Surface Interferometer is an ophthalmic imaging device that is intended for use by a physician in adult patients to capture, archive, manipulate and store digital images of:
- Specular (interferometric) observations of the tear film. Using these images, LipiView® II measures the absolute thickness of the tear film lipid layer.
- Meibomian glands under near-infrared (NIR) illumination.
- The ocular surface and eyelids under white illumination.
CONTRAINDICATIONS
Contraindications are conditions in which the device should not be used because the risk of use clearly outweighs any benefit. No contraindications have been identified for LipiView® II.
PRECAUTIONS
The following patient conditions may affect the interferometry assessment of a patient’s tear film using LipiView® II:
- Use of ophthalmic drops such as artificial tear lubricants, ointments, and medications. Advise patients not not instill oil-based ophthalmic drops (e.g., Soothe®, Restasis®, Systane Balance®) for at least 12 hours prior to device use and not to instill ointments for at least 24 hours prior to device use. Wait at least four (4) hours after the instillation of all other ophthalmic drops prior to device use.
- Soft or rigid contact lens wear. Advise patients to remove contact lenses at least four hours prior to device use.
- Use of oil-based facial cosmetics around the eye.
- Eye rubbing.
- Recent swimming in a chlorinated pool. Advise patients to not to swim for at least 12 hours prior to device use.
- Any ocular surface condition that affects the stability of the tear film. These conditions include disease, dystrophy, trauma, scarring, surgery, or abnormality.
ADVERSE EFFECTS
There are no known or anticipated adverse effects associated with use of this device.
ATTENTION
Reference the LipiView® II Ocular Surface Interferometer Instructions for Use for a complete listing of indications, warnings, and precautions.
INDICATIONS AND IMPORTANT SAFETY INFORMATION for MEIBOMIAN GLAND EVALUATOR (MGE)
Rx Only
INDICATIONS
The Meibomian Gland Evaluator is a hand-held instrument used by a physician to evaluate Meibomian gland secretions in adult patients during a routine eye examination. The instrument provides a standardized method to apply consistent, gentle pressure to the outer skin of the lower eyelid while visualizing the secretions from the Meibomian gland orifices through a slit lamp biomicroscope.
CONTRAINDICATIONS
No contraindications are known.
PRECAUTIONS
- Do not depress the shaft to the endpoint of the spring. Do not apply any additional force after the shaft has been depressed approximately 6 mm. Applying additional force negates the benefit of using the instrument to apply standard force.
- Familiarity with use of a slit lamp biomicroscope is required to use Meibomian Gland Evaluator for assessment of the meibomian gland secretions.
WARNINGS
To ensure proper use of the Meibomian Gland Evaluator, review the warnings below.
- Do not use Meibomian Gland Evaluator if the package is open or broken. Do not use Meibomian Gland Evaluator if it appears broken or has sharp edges or rough surfaces upon initial inspection.
- Maintain proper infection control procedures including cleaning hands before handling the device and before evaluation of each patient. Disinfect the instrument with alcohol after each use and between patients.
- Avoid contact of the devices with the eye. Instruct the patient to look up and away to avoid injury to the cornea in the event the contact surface inadvertently touches the eye.
ADVERSE EFFECTS
Potential adverse effects that are unlikely but may occur with use of the Meibomian Gland Evaluator include but are not limited to:
- Skin abrasion (e.g., from a rough surface on the device)
- Eye abrasion (e.g., from improper contact of the instrument with the eye)
- Infection of the skin or eye (e.g., from improper or lack of disinfection after use and between patients)
- Allergic or toxic reaction (e.g., from exposure to any residue on device during user handling)
ATTENTION
Reference the Meibomian Gland Evaluator Package Insert for a complete listing of indications, warnings, and precautions.
INDICATIONS AND IMPORTANT SAFETY INFORMATION for LIPISCAN® Dynamic Meibomian Imager
Rx Only
INDICATIONS
LipiScan® Dynamic Meibomian Imager (DMI) is an ophthalmic imaging device intended for use by a physician in adult patients to capture, archive, manipulate and store digital images of the meibomian glands.
CONTRAINDICATIONS
No contraindications have been identified for the LipiScan®.
PRECAUTIONS
Caution: Disinfect the surfaces of the chin rest, forehead rest and Handheld Near Infrared (IR) Lid Everter with isopropyl alcohol immediately prior to use and prior to storage to prevent cross-contamination and patient infection.
WARNINGS
Warnings include any potential hazards for adverse events to the patient or user. Review the warnings in Table 1 of the LipiScan® Dynamic Meibomian Imager Instructions for Use prior to using LipiScan®.
ADVERSE EFFECTS
There are no known or anticipated adverse effects associated with use of this device.
ATTENTION
Reference the LipiScan® Dynamic Meibomian Imager Instructions for Use for a complete listing of indications, warnings, and precautions.
Sources:
- Argilés M, Cardona G, Pérez-Cabré E, Rodríguez M. Blink Rate and Incomplete Blinks in Six Different Controlled Hard-Copy and Electronic Reading Conditions. Investigative Ophthalmology and Visual Science. 2015 Oct; 56(11): 6679-85.
- Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous deficient and evaporative dry eye in a clinic based patient cohort: a retrospective study. Cornea. 2012; 31(5):472-478.
- Korb DR, & Blackie CA. (2015). “Dry Eye” Is the Wrong Diagnosis for Millions. Optometry and Vision Science, 92(9), E350-E354.
- Trattler WS, Majmudar PA, Donnenfeld ED, McDonald MB, Stonecipher KB, Goldberg DF. The prospective health assessment of cataract patient (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017; 11: 1423-1430.
- Uzunosmanoglu E, et al. Meibomian gland dysfunction in patients receiving long-term glaucoma medications. Cornea. 2016; 35(8): 1112-1116.
- Starr C, Gupta P, Farid M, Beckman K, Chan C, FRCSC, Yeu E, Gomes J, Ayers B, Berdahl J, Holland E, Kim T, Francis M, the ASCRS Cornea Clinical Committee. An algorithm for the preoperative diagnosis and treatment of ocular surface disorders. ASCRS and ESCRS. 2019; 45.
- Blackie CA, Coleman CA, Holland EJ. The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clin Ophthalmol. 2016; 10: 1385-1396.
- Blackie CA, Coleman CA, Nichols KK, Jones L, Chen PQ, Melton R, Kading DL, O’Dell LE, Srinivasa S. A single vectored thermal pulsation treatment for meibomian gland dysfunction increases mean comfortable contact lens wearing time by approximately 4 hours per day. Clin Ophthalmol. 2018;12:169-183
- Finis D, Konig C, Hayajneh J, Borrelli M, Schrader S, Geerling G. (2014b) Six-month ocular effects of a thermodynamic treatment for MGD and implications of meibomian gland atrophy. Cornea 33 (12): 1265-1270.
- Cochener B, Cassan A, Omiel L. Prevalence of meibomian gland dysfunction at the time of cataract surgery. J Cataract RefractSurg 2018; 44: 144-48
- Hagen KB, Bedi R, Blackie CA, and Christenson Akagi K. Comparison of a single-dose vectored thermal pulsation procedure with a 3-month course of daily oral doxycycline for moderate-to-severe meibomian gland dysfunction. Clin Ophthalmol. 2018; 12:161-168.
- LipiFlow Dynamic Meibomian Imager Instructions For Use.
- Knop E, Knop N, Millar T, Obata H, Sullivan DA. The international workshop on meibomian gland dysfunction: report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci. 2011 Mar 30;52(4):1938-78. doi: 10.1167/iovs.10-6997c. PMID: 21450915; PMCID: PMC3072159.
PP2020MLT7300
© Johnson & Johnson Surgical Vision, Inc. 2020
All other trademarks are the intellectual property of their respective owners.