



Omega-3 fatty acids have been considered a staple in the treatment and management of dry eye disease (DED) along with other methods for many years.
Prescribing omegas became somewhat controversial when the 2018 Dry Eye Assessment and Management (DREAM) study results seemed to question the validity of fish oils, as the study found omega-3 fatty acids offered no benefit over the olive oil placebo.1
What is the DREAM Study?
As a quick refresher, the DREAM Study was a one-year, double-masked, randomized multicenter study by the National Eye Institute. 535 participants with a mean age of 58 who had signs and symptoms of moderate-to-severe dry eye were included. Patients also had to be willing to continue their current dry eye treatment regimens. The inclusion criteria were broad to mimic “real-world” clinical applications because it included patients with dry eye disease who still pursued relief of symptoms even though they were using other interventions.1
A 3000 mg daily dosage of omega-3 fatty acids—2000 mg eicosapentaenoic acid (EPA) and 1000 mg docosahexaenoic acid (DHA)—was used and the daily placebo was approximately 1 tsp or 5000mg of olive oil.
Olive oil primarily delivers omega-9 oleic acid, a substance considered to be neutral with respect to changes in signs and symptoms of dry eye. Patients were followed up with four times within the year and after 12 months, and the authors of the study did not find significant differences in the mean Ocular Surface Disease Index (OSDI), conjunctival staining, corneal staining, Tear Break-Up Time (TBUT), and Schirmer’s test between both groups.1
Interestingly, the DREAM study showed the omega-3 treatment had a phenomenal statistical improvement from baseline, but the placebo treatment worked just as well. It can be fair to state that omega-3 fatty acids do work, and they are effective for managing DED, but the real question is why did the placebo—1 tbsp of olive oil—have a strong level of efficacy that met the omega-3’s?
Interpreting the DREAM study
Including moderate-to-severe dry eye patients of different demographics and health profiles, where subjects were already using different treatments and then allowed to change treatments over time can make it increasingly difficult to come to a definitive conclusion and say that oral omegas are essentially ineffective.
The inclusion criteria of the study were broad and included an enormous slice of the dry eye population with relatively few exclusions. This can easily skew results because given the diversity of the study population that have a complex and multifactorial disease, measuring the effects of a single, non-specific intervention is extremely challenging.2
The placebo used in the study was refined olive oil, an omega-9 oleic acid, meaning it is supposed to have no significant levels of antioxidant and anti-inflammatory compounds. Although, research has shown that oleic acid can alter the microbiome and reduce dysbiosis, allowing for anti-inflammatory effects in the body, including the eyes.3
It is important to acknowledge that the findings of the DREAM study did not thoroughly examine all omegas and therefore its conclusions should not apply to all omegas. The omega-3s used in the treatment arm was 3000 mg of fish-derived EPA and DHA but did not include the omega-6, gamma-linolenic acid (GLA). Particular omega-3 and -6 fatty acids play an integral role in the body’s ability to regulate and balance inflammation.3
Let’s get down to the nitty-gritty: How omega-3 and omega-6 are connected to managing DED
Omega-3 and omega-6 fatty acids are essential nutrients, and they cannot be efficiently synthesized in the body but rather must be obtained from the diet. Both omega-3 and -6 have to go through a series of transformations in order to become active substances in the body, and depending on which substances these omega fatty acids transform into they can have an anti-inflammatory or inflammatory effect.
Depending on dietary intake, omega-3s compete with omega-6s for incorporation into all cell membranes in all tissues of the body. Composition of a cell membrane has an impact on the cell’s function, especially for inflammatory pathways, because these fatty acids will perform important signaling or communication roles within and between cells.4
Omega-3 fatty acids include alpha-linolenic acid (ALA), DHA, and EPA. Since ALA does not efficiently convert to EPA and DHA in the body, EPA and DHA are most commonly found in fish and fish oils where research shows that supplementing with these omega-3s dramatically reduce prostaglandin formation, downregulate proinflammatory gene expression, and inhibit and reduce neutrophil entry to sites of inflammation.5
Omega-6 fatty acids include linoleic acid (LA), dihomo-gamma-linolenic acid (DGLA), GLA, and arachidonic acid (ARA). ARA is the most common omega-6 found abundantly in the American diet, such as many meats, eggs, and dairy, and essentially the precursor to pro-inflammatory markers. But not all omega-6s are pro-inflammatory. GLA is known as the most powerful health-promoting omega-6 and is found in a very limited number of foods, like evening primrose oil, hemp oil, and black currant seed oil and not readily available in the typical American diet.
GLA is produced in the body as an intermediate in the metabolism of LA; however, this reaction is very slow and is further restricted by alcohol use, stress, smoking, trans-fatty acid intake, and deficiencies of magnesium, vitamin B6, and zinc. Administering oral GLA is a means to bypass this inefficient and rate-limiting step in the metabolism of LA to GLA. GLA is then elongated to form the biologically activated DGLA, which goes on to either form the anti-inflammatory prostaglandin E1 (PGE1) or pro-inflammatory ARA (Figure 1).
There are critical metabolic and genetic factors that affect the conversion of DGLA into anti-inflammatory or pro-inflammatory markers, yet these specific biochemical pathways are not well understood. Interestingly, studies have shown that when subjects are supplemented with GLA, it heavily favors the anti-inflammatory pathway when converted to DGLA and produces significantly fewer pro-inflammatory markers.6

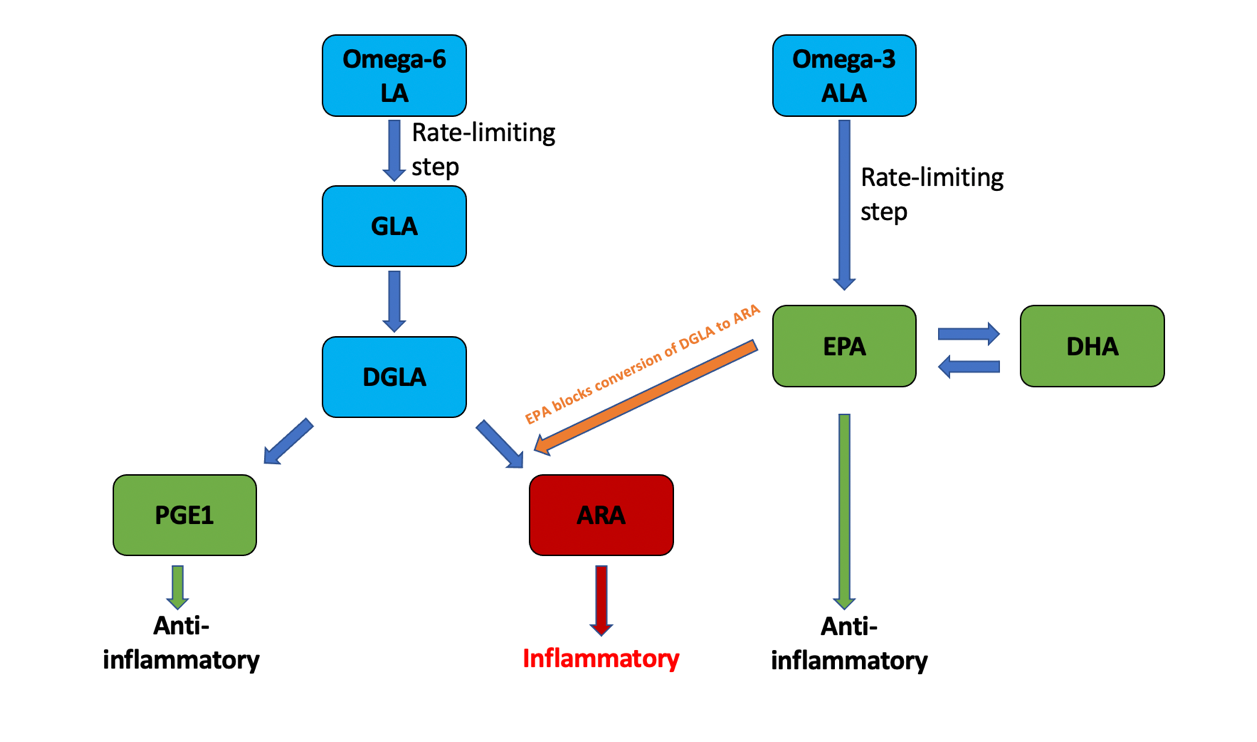
Figure 1: A simplified breakdown of omega-3 and -6 metabolism
One of the main mechanisms of the anti-inflammatory effects of omega-3s is that dietary omega-3s compete with ARAs for a place within cell membranes and inhibit the enzymes that catalyze the biosynthesis of pro-inflammatory markers, such as thromboxane, prostaglandins, and leukotrienes. In more detail, EPA inhibits the only enzymatic step that is necessary to convert DGLA to proinflammatory ARA (orange arrow in Figure 1).
EPA inhibiting this specific enzymatic step promotes metabolic traffic flow to be diverted towards the desirable anti-inflammatory pathway. Thus, omega-3s limit cells from synthesizing the ARA-derived mediators of inflammation. It has been shown that when GLA is combined with the proper balance of EPA one can inhibit production of ARA while stimulating production of anti-inflammatory precursors from both GLA and EPA.7
The purpose of breaking down these complex omega-3 and -6 metabolic pathways is to demonstrate that particular omega fatty acids have the ability to reduce corneal epithelial damage associated with dry eye, increase tear flow, and promote healthy epithelia due to their constant promotion of ant-inflammatory pathways. The advantages of administering particular omega-3s and -6s in the proper combination has been shown to restore the lipid layer, decrease inflammation and apoptosis, and increase tear secretion.8
How to properly prescribe omegas to your patients:
Many studies suggest that people who follow a typical American diet may consume an omega-6 to omega-3 ratio of 20:1. The ideal omega-6 to omega-3 ratio in the diet should be less than 4:1. The overconsumption of omega-6s limits the effectiveness of omega-3s and can easily promote inflammatory processes, such as ocular surface dryness.
The right ratio can also help with cardiovascular health, brain function, and stroke.9 Receiving omega-3 and -6 through nutrition is not enough: supplementation is required to obtain the correct ratios of EPA/DHA and GLA.
Label and Dose?
The two most important factors on an omega fatty acid supplement label are the actual omega-3 and -6 content, expressed in milligrams of EPA, DHA, and GLA, and the number of pills in a serving size.
A reasonable starting dose is between 2000-3000 mg of a combination of higher EPA to DHA daily. GLA should also be supplemented in addition to EPA and DHA in a balanced ratio. Ingesting similar levels of EPA and GLA increases cellular membrane content of both DGLA and EPA, which are precursors to anti-inflammatory markers. This supplementation strategy successfully maintains the anti-inflammatory capacity of GLA and EPA, without causing accumulation of the inflammatory elements from ARA.7
Form: Triglycerides or Ethyl Esters?
Even though omega-3 and -6 occur naturally in the triglyceride (TG) form, for purification and concentration purposes, many manufacturers create fatty acid ethyl esters (EE) by modifying the TG structure where the glycerol backbone is substituted with ethanol. Many over-the-counter omega supplements are in this EE form.
Research shows gastrointestinal (GI) digestive enzymes break down EE to a much lesser extent than TG causing poorer absorption of EE, and thus causing GI issues. In a process called re-esterified TG, some manufacturers convert the EE back to the natural TG form of having the glycerol backbone. This method creates a better tolerated and more easily absorbed product, even though the cost of the product will likely be higher.10
Precautions?
Excessive bleeding? Administering EPA and DHA at more than 3000 mg per day may increase the risk of bleeding. Take into account if patients are on any blood thinners or taking supplements known to have anticoagulant effects.11
Immunocompromised? Since the combination therapy of omega-3 and -6 suppress inflammatory responses and effectively benefit those with inflammatory or autoimmune conditions, caution should be used for those that have compromised immune systems because of the decreased ability to fight against microbial pathogens.12
Upset stomach? Indigestion, diarrhea, constipation, and those “fishy burps” are more likely to occur with high doses of fish oils and the more difficult to digest EE forms of supplementation.11
Ocular surface dryness is a multifactorial disease that involves various inflammatory components and the importance of the anti-inflammatory effects of omega-3 and -6 cannot be underestimated in its management. Even though numerous eyecare professionals will attest to having proof from their own patient base that prescribing only omega-3s significantly helps manage their DED patients, it is important to remember that many studies have shown nutritional supplementation of EPA and DHA in combination with GLA in a proper balanced ratio can considerably help alleviate several dry eye signs and symptoms as well.

