
You walk in to the office on your very first day as an employed OD.
As you grab your cup of coffee and greet the office staff, you sit down at your computer to look over the day’s schedule. To your surprise, you see no middle-aged myopes, zero red eye exams, and not a single glaucoma work-up scheduled.
Instead you find 14 patients between the ages of 10 years and 6 months old!
This is a joke, right?
As much as I wish I could’ve laughed it off as the ol’ “let’s prank the new doc” trick, this was exactly how my first day as an OD began.
While I’ve always had a knack for vision therapy and have enjoyed working with kids, nothing could have prepared me for that first day’s gauntlet. Fast-forward one month and now with a full day’s schedule I average 12 patients a day under the age of 12.
Needless to say, I’ve had to quickly adapt my exam technique and get in and out with as much information as possible.
If you have the right tools, and go in with a game plan, examining children really isn’t all that intimidating. If done right, you can even turn it into a tremendous practice builder and leverage for potential practice ownership.
Step 1: Make your technicians your sidekick.
It’s absolutely true what they say about first impressions.
Especially when it comes to children. The first person that walks through that door to greet them and escort them to the exam room HAS to have their trust.
Particularly difficult when one of the first things the child is forced to do is shove their head in a chin rest and stare into an autorefractor. Add in having to cover up an eye to read blurry letters, having bright lights shined at them, and getting poked in the eyes with a tonometer and you have the recipe for ZERO trust.
I learned very early on that my technicians were my absolute greatest allies when it came to gaining a child’s trust. Similar to a championship bull rider, you must rely on a few of your closest rodeo clowns to make sure you get out alive.
In order to keep things on track, train your technicians to get as much pertinent information as they can as quickly as possible. With the attention span of a goldfish, kids only grant you so much of their time before they attempt to swing from the phoropter or use your fundus lenses as marbles.
Simplest form of visual acuity –
A lot of docs will say, “There’s no way for me to do pediatrics! It’s not practical for me to spend thousands of dollars on Teller cards, OKN drums, and Broken Wheel charts.”
The reality… Snellen or Allen pics work just fine for the majority of children. Now of course an infant isn’t going to be able to identify letters or pictures, but using “fixate and follow” or an OKN ribbon is just as easy with no additional investment. If possible, I encourage my technicians to use single form vertical lines to speed up the process.
A one-letter column going from 20/50 to 20/25 is used to start. If the child is able to read all the way down, a single isolated 20/20 line is then tested. If they’re struggling, isolate a single letter with or without crowding bars and slowly decrease the size to determine their threshold.
Tell your technicians to make it a game for the child in order to keep him or her interested.
Push them to their limits.
Attempt to get monocular acuities as best they can.
Have the child use an occluder or “occlusion glasses” in order to keep them from trying to peek through their hands. Kids will do anything they can to read every letter. You and your technicians have to learn how to out smart even the smartest kids.
Binocular status –
I recognize that technicians are not as well tuned to subtleties of cover test, so to make it easier on them I use a “phoria measure” or Maddox rod with attached prism (pictured).


To do this, they instruct the child to hold the paddle over their right eye with the Maddox rod bars oriented horizontally.
Then, standing across the room with a penlight or transilluminator, they ask the patient what they see.
If binocular, they should see a spot of light and a red vertical line. The child is then instructed to rotate the prism dial until the light and the line are lined up. The amount of prism and direction are then recorded.
The process is then repeated for the vertical phoria using a horizontal line. Typically this is only used on children 5 or older or those that are able to understand the instructions.
If a phoria measure is not available, the same process can be completed using a Maddox rod over one eye and prism bar over the other. This subjective dissociated phoria gives me much more usable data than even the most skilled cover testing technician. No offense to my technicians reading this!

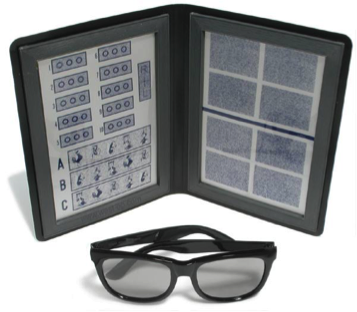
As an additional binocular function screener, I also encourage a Randot stereo test on all children older than 4 if possible. Kids love putting on the “magic sunglasses” and reading the “3D book.”
Even if they aren’t able to appreciate any of the targets, the “R+L” suppression checks give me useful information about any potential alternating fixation.
Performance-based case history –
Ask both the child and their parents about their scholastic performance including their current grade level, subjects they excel at, subjects they struggle in, and any difficulties they may be having in the classroom. Difficulty in reading and/or math can indicate saccadic dysfunction or perceptual difficulties that can be easily improved with vision therapy.
The remainder of the medical and social history is completed over the phone prior to the exam in order to mitigate time spent in office filling out paperwork.
Step 2: Channel your inner child.
Take a moment to remember what it was like for you as a child to go to the doctor’s office.
I guarantee that you only remember the doctors you had that were fun, loved to joke and play, and were probably a little nutty. Kids are much more likely to play along with you if you think, act, and talk like them.
When talking to the parents in front of the child, instead of using big words like “convergence, acuity, and amblyopia,” use words like “eye teaming, x-ray vision, and sleepy eye” instead. The more time the child spends in your office waiting, the less likely they are to pay attention during your exam.
Parents will understand what you mean and appreciate that you’re not using intimidating language to talk to their child.
In addition, don’t be afraid to be as silly as you possibly can. I’ve never heard of a parent complaining that their child’s doctor was “too much fun” and “not serious enough.”
From the moment you walk in the door to the time you leave, make plenty of jokes, laugh along with the kids, and leave with a high five or knuckles every single time. Oh, and don’t forget to have plenty of stickers around for after they’re all done!
Step 3: Rely on what you see more than what you hear.
Kids are going to be kids. They think your “1 or 2” routine is just a game.
They want to “cheat” on your tests by squinting, closing an eye, or repeating the same letters they’ve already read even if they can’t see them.
No matter their motivation, they will do everything they can to either avoid or ensure the potential for getting glasses.
What’s your best counter move?
Deception (as awful as that sounds).
You have to come up with sly ways to trick them into thinking that refraction is super important, where they look during slit lamp is their life’s duty, and that 0.12 diopter lens you have in your trial kit is the “magic lens” that will help them see.
Throw them into a pediatric trial frame and claim “these will make you see like a super hero!”
As much as you may despise it, your retinoscope is a savior when it comes to getting the information you need. Made famous by one of my mentors, Dr. Glen Steele, “just look” retinoscopy really can tell you a lot about how the child is using their eyes.
Subtleties in brightness, clarity, and motion of the reflexes will reveal much more than what the child is able to verbalize.
It takes time to hone these skills, and I don’t claim to be an expert, but if you slow down your retinoscopy techniques, you’ll begin to gather all the information you need to guide your treatment plan.
For more tips on pediatric optometry
Here are my top 3 tips to getting everything you need with only 3 minutes of retinoscopy:
Step 1: Check quickly for an equality of retinoscopy reflexes by having the child look directly at you while viewing with either a retinoscope or direct ophthalmoscope. (30 seconds) Remember, a dimmer than normal reflex indicates a non-fixating or amblyopic eye.
Step 2: For younger kids who refuse to fixate on a big red-green E…perform distance retinoscopy using cycling 20/125 red-green letters or your favorite Disney movie on repeat. If your electronic chart system allows, a movie enables you to see how the child’s refractive status changes while viewing an interesting distance target. (1.5 minutes) Take your time and pay attention to the way the eye’s reflex changes with changes in the target viewed.
Step 3: Repeat retinoscopy at near to test the child’s accommodative response. (1 minute)
It may come as a surprise, but kids are not interested in your near retinoscopy targets. Reading the same five words or “finding the letter” gets boring real quick. Instead, I use an old iPod Shuffle with Nickelodeon videos on it as a near fixation target. I hold it at the same plane as my retinoscope as I scope with skiascopy bars.
Pediatric optometry can be extremely challenging, yet immensely rewarding. In order to get through the exam without losing your Legos, remember to remain patient, utilize your technicians, and think like a kid.