



It’s Friday night, and the clinic is closing in less than an hour when you receive an emergency call. The patient complains of a red eye. How many optometrists can relate to this scenario?
Red eye is one of the most common ocular concerns that arise on a weekly basis in the offices of optometrists and physicians. Most patients continue to visit their physicians for these concerns. An Australian study found that 64% of treated cases by primary care physicians were misdiagnosed and 10% led to serious complications.6 Misdiagnosis and not knowing when to refer the patients can result in devastating consequences. Before going over a few common conditions, let’s go back to the basics.
Back to the basics
One of the basic aspects as physicians is communication. Taking an in-depth case history and determining the patient’s chief complaint is beneficial to streamline the eye examination. The chief complaint of red eyes may yield an extensive list of differentials and a detailed case history can formulate differential diagnoses. Listed below are a few important questions.
Case history for red eye
| Frequency | Previous episode or history? |
| Onset | Acute vs Chronic? |
| Location | Unilateral or Bilateral? Diffuse or Localized? |
| Duration | How long have symptoms been present? |
| Alleviating factors | Use of artificial tears or other eye drops? Cold compresses? |
| Related symptoms | Discharge? Burning? Tearing? Itching? Pain? Photophobia? Foreign body sensation? Blurry vision? |
| Quality | Pain threshold? (on scale of 1 to 10) |
| Ocular history | History of trauma or chemical injury? Exposure to an infected person? Contact lens wearer? Use of topical or over the counter drops? |
| Medical/Social history | Recent illness or infections? Computer use? Occupation? Smoking history? |
Communication, observations and listening to key phrases can narrow down a list of differential diagnoses. For example: a patient says ‘My eyes are always itchy’ which may indicate allergies or if your patient walks into the exam room wearing sunglasses, the patient may be photophobic. Good communication skills and bedside manner are critical skills for all physicians and can help lead to a more accurate diagnosis for the patient.
This article is a review of a few conditions commonly associated with red eyes, listed in order of urgency of the conditions (least to most urgent).
- Subconjunctival hemorrhage
- Dry eye syndrome
- Conjunctivitis
- Contact lens related problems
- Episcleritis/Scleritis
- Iritis
- Foreign body & Corneal abrasion
Subconjunctival hemorrhage
Subconjunctival hemorrhage is defined as diffuse or focal area of blood under the conjunctiva due to ruptured conjunctival blood vessel. Patients are usually asymptomatic.

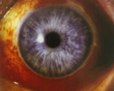
Figure 1: Subconjunctival hemorrhage2
| Key phrase | “I did not notice anything until someone said something.” |
| Etiology | Idiopathic Valsalva (coughing, sneezing, constipation) Trauma (isolated or associated with retrobulbar hemorrhage or ruptured globe) Systemic conditions (hypertension, diabetes) Bleeding disorders Use of antiplatelet or anticoagulant medications (aspirin, clopidogrel, warfarin) |
| Signs | Focal or diffused hemorrhage Rule out conjunctival lesions and ruptured globe (check extraocular motility, intraocular pressure) If recurrent or suspect bleeding disorder, refer for blood work (bleeding time, prothrombin time, partial thromboplastin time, complete blood count, liver function test, protein C and protein S) |
| Treatment | Condition is self-limiting with spontaneous resolution within 2-3 weeks Artificial tears may be given if ocular irritation is present |
| Follow up | No follow up necessary unless condition reoccurs Refer to family doctor for high blood pressure and bleeding disorder if recurrent |
Dry eye syndrome
Keratoconjunctivitis sicca, also known as dry eye syndrome, is caused by decreased tear production or poor tear quality. It may be associated with increased age, female > male, medications and some medical conditions.
| Key phrase | “My eyes are watering and I feel like something is in it.” |
| Symptoms | Burning/Dryness Foreign body sensation Excessive tearing |
| Signs | Scant, irregular tear prism at inferior eyelid margin Decreased tear break-up time Punctate corneal or conjunctival staining Excess mucus or debris in tear film Meibomian gland dysfunction |
| Treatment | Artificial tears Lubricating ointment QHS or lubricating gel QHS Lifestyle modifications (use of humidifiers, smoking cessation) Cyclosporine 0.05% BID for chronic dry eye |
| Follow up | Depends on severity |
Conjunctivitis
Conjunctivitis is the most common cause of red eyes, viral being the most prevalent. The term conjunctivitis refers to the inflammation of the conjunctiva. Below are a few clinical pearls for differentiating viral, bacterial and allergic conjunctivitis.
Viral Conjunctivitis

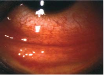
Figure 2: Viral conjunctivitis2
| Key phrase | “I think I have pink eye.” |
| Prevalence | Most prevalent (80%) |
| Contagious | Highly for 10-12 days |
| Medical history | Recent upper respiratory tract infection(cough/flu) |
| Location | Unilateral or bilateral |
| Symptoms | Itching/Burning Foreign body sensation Tearing |
| Discharge | Watery |
| Preauricular nodes | Tender nodes |
| Other signs | Follicles inferiorly Edematous eyelids Intraepithelial microcyst Subepithelial infiltrates |
| Treatment | Self-limiting; however, palliative therapies include: Artificial tears Mild steroid (if necessary) |
| Counseling | Copious handwashing Avoid touching eyes |
| Follow up | 2 weeks or sooner if condition worsens |
Bacterial Conjunctivitis

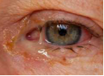
Figure 3: Bacterial conjunctivitis3
| Key phrase | “My lids are shut closed when I wake up.” “My eyes are goopy.” |
| Prevalence | Second most prevalent Children > Adults |
| Contagious | Yes |
| Medical history | None |
| Location | Unilateral or bilateral |
| Symptoms | Foreign body sensation Matted eyelashes |
| Discharge | White/yellow purulent |
| Preauricular nodes | No |
| Other signs | Conjunctival papillae Moderate hyperemia Conjunctival chemosis |
| Treatment | Broad spectrum antibiotic (5-7 day course) |
| Counseling | Avoid touching eyes |
| Follow up | 2-3 days then every 5-7 days until resolved |
Allergic conjunctivitis

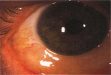
Figure 4: Allergic conjunctivitis2
| Key phrase | “My eyes are itchy." |
| Prevalence | During allergy season |
| Contagious | No |
| Medical history | Seasonal allergies Airborne allergens |
| Location | Usually bilateral |
| Symptoms | Itching & burning |
| Discharge | Watery |
| Preauricular nodes | No |
| Other signs | Conjunctival papillae Mild hyperemia Conjunctival chemosis Red edematous eyelids |
| Treatment | Cold compresses Artificial tears Anti-histamine or Mast cell inhibitors Mild steroid (if necessary) Oral anti-histamine (if necessary) |
| Counseling | Eliminate allergen Avoid rubbing eyes |
| Follow up | 1-2 weeks |
Contact lens related problems
Contact lenses are used for correcting refractive errors, for cosmetic use and for therapeutic use such as bandage lens. However, contact lens overwear may cause several complications including giant papillary conjunctivitis, superior limbic keratoconjunctivitis & corneal ulcer.
Giant Papillary Conjunctivitis


Figure 5: Giant papillary conjunctivitis3
| Key phrase | “My eyelids feel heavy and I need to rub them.” |
| Etiology | Contact lens overwear Loose fit (excessive lens movement) |
| Symptoms | Itching & burning Foreign body sensation |
| Signs | Upper tarsal micropapillae Superior limbal injection Ropy mucous discharge |
| Treatment | Educate patient on proper contact lens care For mild GPC: Decrease wear time of contact lenses Topical mast cell inhibitor or antihistamine For severe GPC: Suspend use of contact lenses Topical steroid |
| Follow up | 2-4 weeks |
Superior Limbic Keratoconjunctivitis


Figure 6: Superior limbic keratoconjunctivitis2
| Key phrase | “I cannot wear my contacts for long anymore.” “I have to take out my contact lenses more often.” |
| Etiology | Hypersensitivity/toxicity reaction to preservatives in contact lens solution |
| Symptoms | Itching & burning Foreign body sensation Contact lens intolerance |
| Signs | Upper tarsal micropapillae Superior limbal injection Pannus at 12 o’clock |
| Treatment | Suspend use of contact lenses Switch to preservative free contact lens solution Use preservative free artificial tears Topical steroid (if necessary) |
| Follow up | 2-4 weeks |
Corneal Infiltrate & Corneal Ulcer


Figure 7: Corneal ulcer3
| Key phrase | "My eyes are red and hurt.” |
| Etiology | Bacterial Fungal Acanthamoeba |
| Symptoms | Pain Photophobia Contact lens intolerance |
| Signs | White stromal opacity Corneal thinning/ulcer Anterior chamber reaction |
| Treatment | Cycloplegic drops for comfort For mild condition: Fluoroquinolone q1-2 hrs For severe condition: Fluoroquinolone q1-2 hrs |
| Follow up | 1 day Maintain treatment until condition resolves |
Episcleritis & Scleritis
Episcleritis is a localized area of inflammation of connective tissue between sclera and conjunctiva involving whereas scleritis is defined as an inflammation of the scleral tissue.
Episcleritis

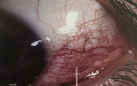
Figure 8: Episcleritis3
| Key phrase | “My eye is red in the corner.” |
| Epidemiology | 80% simple, 20% nodular Bilateral in 33% of cases |
| Etiology | Idiopathic Infectious (herpes zoster) Other (rosacea, atopy, collagen vascular disease, gout, thyroid disease) |
| Symptoms | Mild pain Hyperemia |
| Signs | Sectoral injection Chemosis Episcleral nodules Cells and flare |
| Treatment | Artificial tears Topical steroid (Fluorometholone QID) Oral NSAID for severe cases |
| Follow up | 1 week |
| Prognosis | Self-limiting condition & good prognosis Recurrent in 67% of cases |
Scleritis

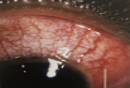
Figure 9: Scleritis3
| Key phrase | “My eye is red and it hurts.” |
| Epidemiology | 40% diffuse, 44% nodular, 14% necrotizing |
| Etiology | Idiopathic Connective tissue disease Herpes zoster ophthalmicus Syphilis |
| Symptoms | Severe pain Hyperemia & chemosis |
| Signs | Decreased vision Diffused injection Chemosis Scleral nodules Globe tenderness Cells and flare |
| Treatment | Oral steroid (Prednisone 60-100 mg po QD) Systemic NSAID |
| Follow up | 1 week or sooner if symptoms worsen |
| Prognosis | Depends on etiology (poor for necrotizing) Recurrence is common |
Iritis
Iritis, also known as anterior uveitis, is an idiopathic inflammation of uvea (iris, choroid and/or ciliary body).

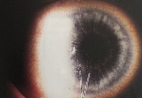
Figure 10: Keratic precipitates3
| Key phrase | “I am light sensitive.” |
| Symptoms | Pain Redness Photophobia Decreased vision |
| Signs | Anterior chamber reaction (cells and flare) Ciliary flush Keratic precipitates Hypopyon Iris synechiae |
| Treatment | Cycloplegic bid Topical steroid (Prednisolone acetate 1% q4-6 hrs depending on severity) May consider steroid ointment overnight |
| Follow up | Every 1-7 days depending on severity, assess patient’s IOP at each visit Taper steroid once anterior chamber reaction has resolved |
Foreign body & corneal abrasion
Defined as defects to the corneal epithelium, corneal abrasion can cause irritation, pain, tearing and photophobia.

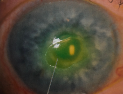
Figure 11: Corneal abrasion3
| Key phrase | “Something got into my eye and it hurts.” |
| Risk factors | Foreign body Trauma Contact lens use |
| Symptoms | Sharp pain Photophobia Foreign body sensation Tearing |
| Signs | Epithelial defect (stains with fluorescein) Conjunctival injection Mild anterior chamber reaction Protective ptosis |
| Treatment | For non-contact lens wearer: antibiotic ointment q2-4 hrs or antibiotic drops QID For contact lens wearer: anti-pseudomonas coverage, antibiotic ointment or drop QID For abrasion secondary to fingernail or vegetative matter: Fluoroquinolone QID For large abrasion: place bandage contact lens |
| Follow up | For bandage contact lens: follow up within 24 hrs for re-evaluation Central or large abrasion: follow up within 24 hrs for re-evaluation Peripheral or small abrasion: follow up within 2-5 days |
Conclusion
Red eye is the most common complaint found amongst patients and the concept that every case is a ‘pink eye’ is a huge misunderstanding. The average person will call their family physician if they have an eye problem. There is a misconception that optometrists only provide a spectacle prescription. Upon questioning patients, they are often unaware that optometrists may provide more detailed care including urgent eye problems. Reaching out to family physicians and providing reports for mutual patients can build a foundation for better communication between optometrists and family physicians. Educating patients and the public with regards to our role as primary care optometrists may help to prevent misdiagnosis and further patient consequences. Stay tuned for more details regarding atypical conditions in association with red eyes.
Citations
- Cronau H, Kankanala R, Mauger T. Diagnosis and Management of Red Eye in Primary Care. American Family Physician. 2010;81(2):137-144.
- Ehlers JP, Shah CP, Fenton GL. Wills Eye Manual Office and Emergency Room Diagnosis and Treatment of Eye Disease. Philadelphia, PA: Wolters Kluwer Health; 2012.
- Friedman NJ, Kaiser PK. The Massachusetts Eye and Ear Infirmary: Illustrated Manual of Ophthalmology. Philadelphia, PA: Saunders, Elsevier; 2014.
- Frings A, Geerling G, Schargus M. Red Eye: A Guide for Non-specialists. Deutsches Arzteblatt International. 2017;114:302-312. doi:10.3238
- Gilani C, Yang A, Yonkers M, Boysen-Osborn M. Differentiating Urgent and Emergent Causes of Acute Red Eye for the Emergency Physician. Western Journal of Emergency Medicine. 2017;18(3):509-517. doi:10.5811
- Statham MO, Sharma A, Pane AR. Misdiagnosis of acute eye diseases by primary health care providers: incidence and implications. Med J Aust. 2008;189:402–404
- Vo A, Williamson J. Red Eye Roundup. Review of Optometry. https://www.reviewofoptometry.com/article/red-eye-roundup. Published March 15, 2019. C
