



We present a case of bilateral central retinal artery occlusion (CRAO). Case reports have been published linking bilateral central retinal artery occlusion to antiphospholipid syndrome1,2, Hughes Syndrome3, acute respiratory distress syndrome4, metastatic Burkitt-type lymphoma5, positive human immunodeficiency virus (HIV) status6,7, sickle cell hemoglobinopathies8-10, giant cell arteritis11, and cocaine abuse12.
Case report
A 45-year-old male with essential hypertension, hyperlipidemia, a history of a cerebral vascular accident approximately one year prior without residual deficits, gastroesophageal reflux disease, and diabetes mellitus type 2 with a history of severe non-proliferative diabetic retinopathy with macular edema in both eyes (status-post two injections of ranibizumab in both eyes four months prior to presentation) presented as an urgent add-on to a retina specialty clinic with acute “foggy” vision in the left eye for two days. Best corrected visual acuity was 20/20 in the right eye and 20/25 in the left eye with the remainder of his examination grossly unchanged from previous including an optical coherence tomography (OCT) of his macula without notable macular edema in either eye (Figure 1).

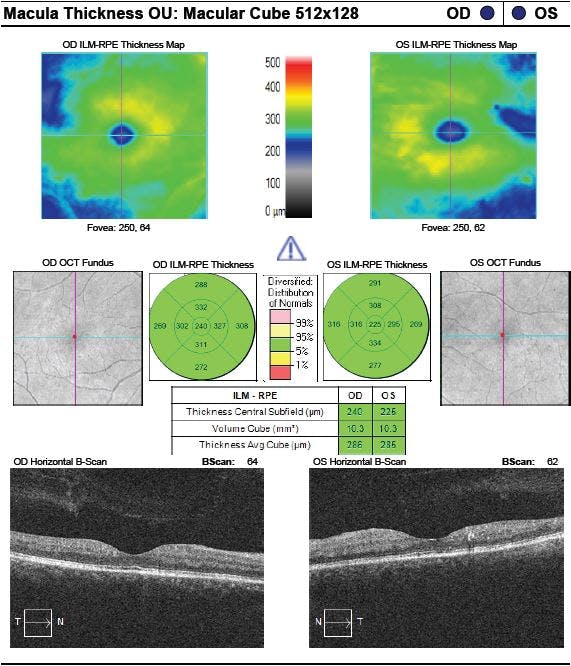
Figure 1. Optical coherence tomography (OCT) of the macula of both eyes obtained two days prior to patient’s loss of vision. Right eye demonstrates grossly normal findings and left eye reveals hard exudates in the parafoveal macula.
Two days later, the patient noticed cloudy vision in the right eye followed by a sudden onset of complete vision loss for 20 minutes in both eyes recovering only to “dark and cloudy” vision. Patient did not present to an emergency room, but called his retina specialist two days after symptom onset to be seen. He was evaluated that same day.
His visual acuity was counting fingers at 1 foot in both eyes. The dilated fundoscopic exam as well as fundus photography (Figure 2) showed flat and pale macula bilaterally with ghost vessels.

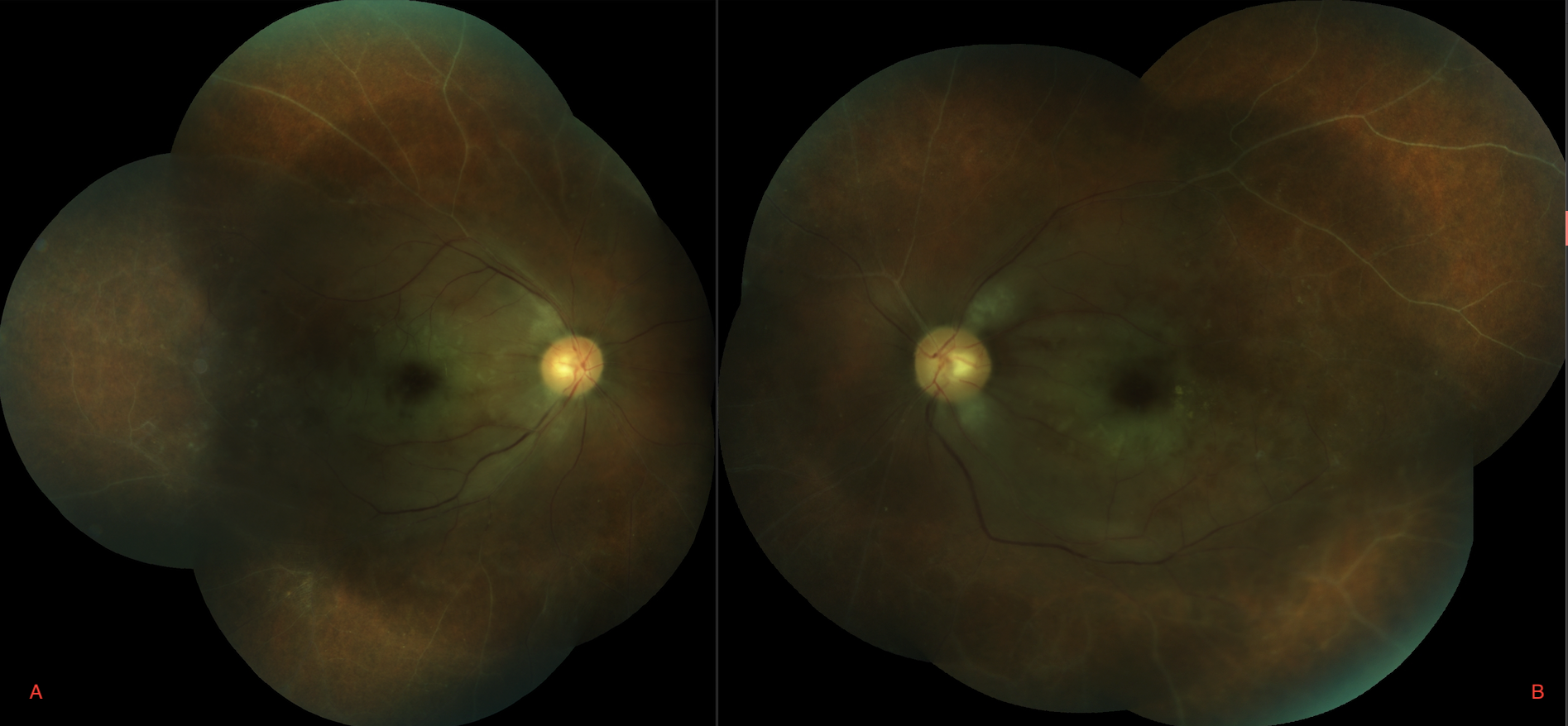
Figure 2. Fundus photography of right (A) and left (B) eyes two days after patient’s loss of vision demonstrate pale macula as well as sclerotic/ghost vessels in both eyes.
OCT of the macula (Figure 3) revealed bilateral significant photoreceptor loss, significant decrease in reflectivity of the outer retinal layer, and an increased reflectivity and thickness of the inner retina.
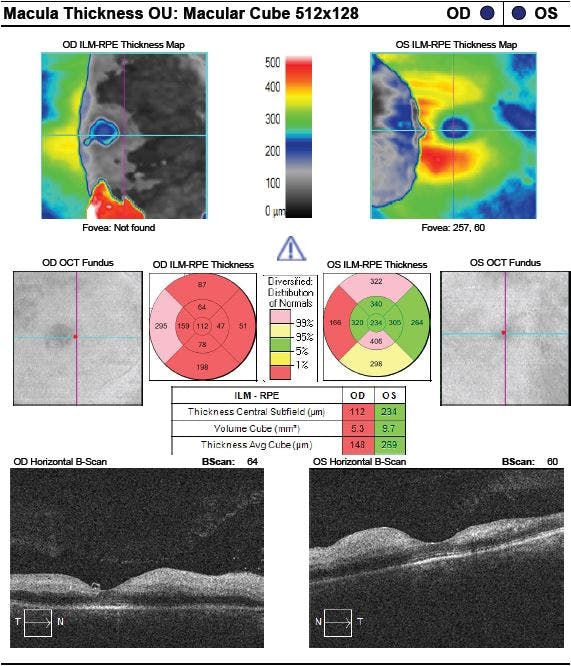
Figure 3. Optical coherence tomography (OCT) of the macula of both eyes two days after patient’s loss of vision demonstrates significant photoreceptor loss, significant decrease in reflectivity of the outer retinal layer, and an increased reflectivity and thickness of the inner retina in both eyes.
Fluorescein angiography (Figure 4) revealed delayed and poor arterial flow with capillary dropout only sparing approximately 3 disc diameters in the peripapillary region and extending up to 5 disc diameters temporally over the macula. The patient was sent to the emergency department for laboratory and imaging work up.

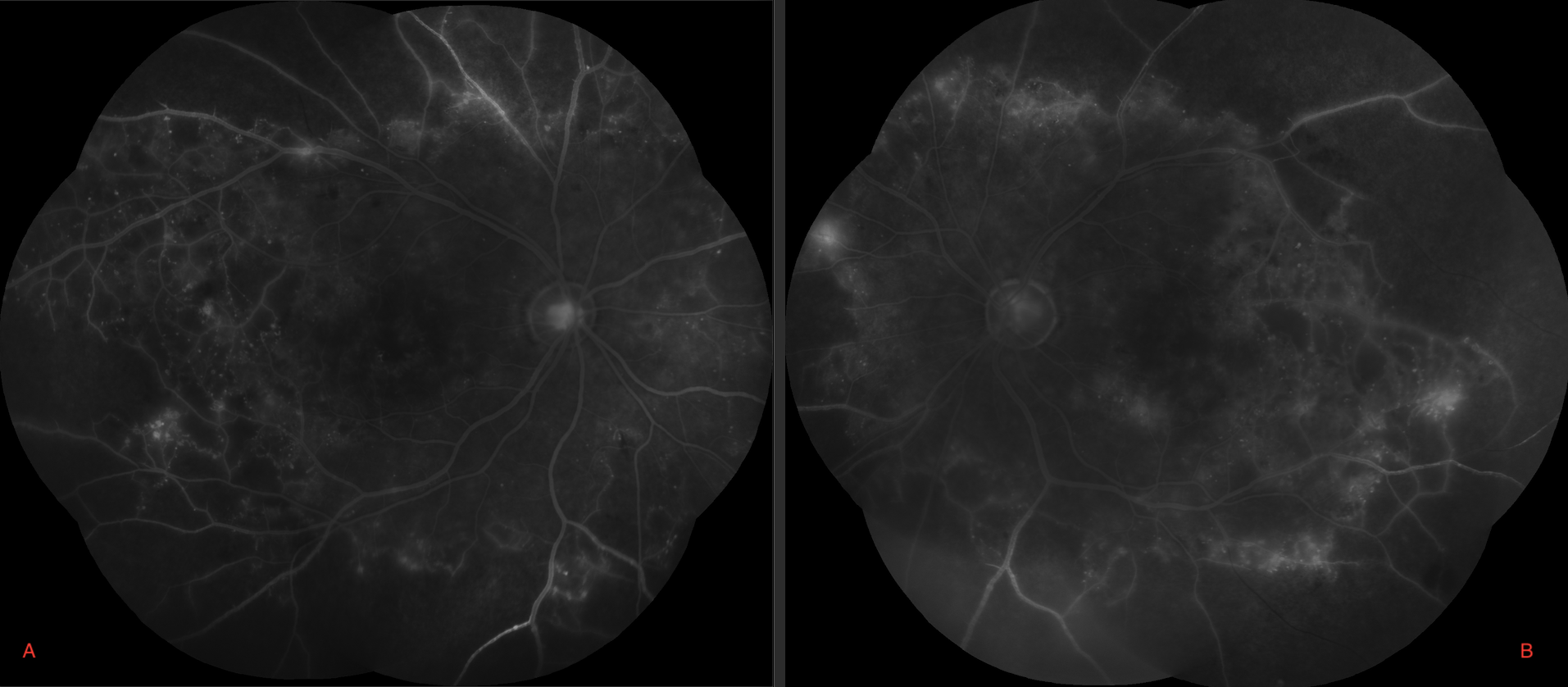
Figure 4. Fluorescein angiography of both eyes (A–right; B–left) demonstrate significant capillary non-perfusion in peripheral retina with sclerotic vessels.
The patient’s laboratory findings were non-reactive, negative, or within normal limits for the following tests: urine drug screen, C-reactive protein, angiotensin-converting enzyme, antinuclear antibody, protein S, anithrombin III, prothrombin G20210A mutation, Beta-2 glycoprotein antibody, lupus anticoagulant, PT/PTT, anti-Smith, anti-centromere, C3/C4, homocysteine, cardiolipin IgA/IgG/IgM, QuantiFERON gold, TSH/T4, rapid plasma regain, fluorescent treponemal antibody absorption, antineutrophil cytoplasmic antibodies, anti-Scl 70, anti-Ro/SSA, and anti-La/SSB. The patient’s ESR was elevated to 66 and had a Protein C level greater than 200. An MRI/MRA of the brain revealed no acute intracranial abnormalities without evidence of vasculitis or acute infarct. A carotid ultrasound revealed no evidence for hemodynamically significant carotid stenosis and a transthoracic ultrasound uncovered no significant intracardial findings. Six days after presentation, a temporal artery biopsy was performed and revealed Mönckeberg medial calcification without evidence of giant cell temporal arteritis. Review of systems was unremarkable and the patient did not have any symptoms suggestive of giant cell arteritis.
Discussion
This patient carried numerous risk factors for the development of CRAOs including male gender, hypertension, diabetes, hyperlipidemia, and a history of a cerebral vascular accident. Cases of bilateral CRAOs have previously been published in the setting of antiphospholipid syndrome1,2, Hughes Syndrome3, acute respiratory distress syndrome4, metastatic Burkitt-type lymphoma5, positive human immunodeficiency virus (HIV) status6,7, sickle cell hemoglobinopathies8-10, giant cell arteritis11, and cocaine abuse12, but to our knowledge and literature review, this is the first published case of a bilateral central retinal artery occlusion in the absence of those conditions.
One consideration is that the patient could have used amphetamines that cleared from his urine by the time of urine drug screening. A peculiarity in this patient’s presentation was his symptomatic presentation two days prior to his presumed event bilateral CRAOs. Upon that day’s evaluation, neither his fundoscopic exam nor his OCT of the macula revealed an obvious change from his baseline and his visual acuity was only mildly affected in the left eye (20/25). Perhaps this patient had experienced a temporary ischemic event provoking his initial presentation.
Risk factors for CRAOs are well established and this patient carried many of them. In the absence of any other clear risks for development of disease bilaterally, it is difficult to attribute a proximate cause or how to anticipate events like this case. At this time, primary prevention and management of comorbid conditions that are risk factors for CRAOs are likely the best plan of action for patients who carry a similar history to this patient.
References
- Saraf SS, Patel YP, Desai A, Desai UR. Catastrophic antiphospholipid syndrome presenting as bilateral central retinal artery occlusions. Case Rep Ophthalmol Med. 2015;206906.
- Joshi U, Afroz S, Ranka S, Mba B. Bilateral central retinal artery occlusion from catastrophic antiphospholipid syndrome. BMJ Case Rep. 2018.
- Sheth S, Rush RB. Bilateral central retinal artery occlusions and hughes syndrome. Retina Cases Brief Rep. 2012;6(3):304-6.
- Gui W, Friesen ET, Bonelli L, Wang YE, Arnold AC. Severe bilateral optic nerve and retinal hypoperfusion in a patient with acute respiratory distress syndrome and septic shock. Am J Ophthalmol Case Rep. 2017;6:84-87.
- DeSouza PJ, Hooten CG, Lack CM, John VJ, Martin TJ. Bilateral Central Retinal Artery Occlusion Associated with Bilateral Lymphoproliferative Infiltrative Optic Neuropathy. Ocul Oncol Pathol. 2017;3:229-34.
- Babu K, Sudheer B, Murthy KR. Bilateral arterial occlusions masking retinitis in a HIV-positive male. Indian J Ophthalmol. 2018;66(2):332-4.
- Bansal R, Jain S, Gupta V, Sharma A, Bal A, Jain S. Bilateral central retinal artery occlusion as presenting manifestation of human immunodeficiency virus infection. Indian J Ophthalmol. 2019;66(3):466-8.
- Okonkwo ON, Hassan AO, Gyasi ME, Oderinlo O. Bilateral Simultaneous Macular Infarction with Spontaneous Visual Recovery in Genotype SS Hemoglobinopathy Patient. Niger J of Clin Pract. 2017;20:1651-5.
- Clarke WN, Vomiero G, Leonard BC. Bilateral simultaneous retinal arteriolar obstruction in a child with hemoglobin SS sickle cell disease. J AAPOS 2001;5:126‑8
- Cusick M, Toma HS, Hwang TS, Brown JC, Miller NR, Adams NA, et al. Binasal visual field defects from simultaneous bilateral retinal infarctions in sickle cell disease. Am J Ophthalmol 2007;143:893‑6.
- Hankins M, Amin S, Gonzalez A, Samy H. Combined bilateral ophthalmic artery occlusion & central retinal vein occlusion from presumed giant cell arteritis. Am J Ophthalmol Case Rep. 2018;12:28-31.
- Campbell J, Burkholder B, Dunn, J. Catastrophic antiphospholipid antibody syndrome and cocaine abuse associated with bilateral retinal vascular occlusions. Retin Cases Brief Rep. 2011;5(4):318-22.

