




Case presentation of 61-year-old female with extreme case of retinal disease
In this presentation, we’re going to discuss diabetic retinopathy and the role of OCT angiography in routine to extreme cases. We have a 61-year-old female presenting for a doctor-directed follow up. She's managed in our clinic for both glaucoma suspicion and diabetic retinopathy, but here, we’ll be focusing only on her diabetic history and imaging. She has type 2 diabetes, a fasting blood sugar of 110, and an A1c of 8.5. She reports moderate control and that she's taking two medications. Her BCVA is 20/20 in both eyes.
61-year-old female presents for doctor directed follow-up
- Type II DM
- FBS 110
- A1c 8.5
- Medications
- Metformin 500 mg BID
- Glyburide QD
- BCVA
- OD: 20/20
- OS: 20/20
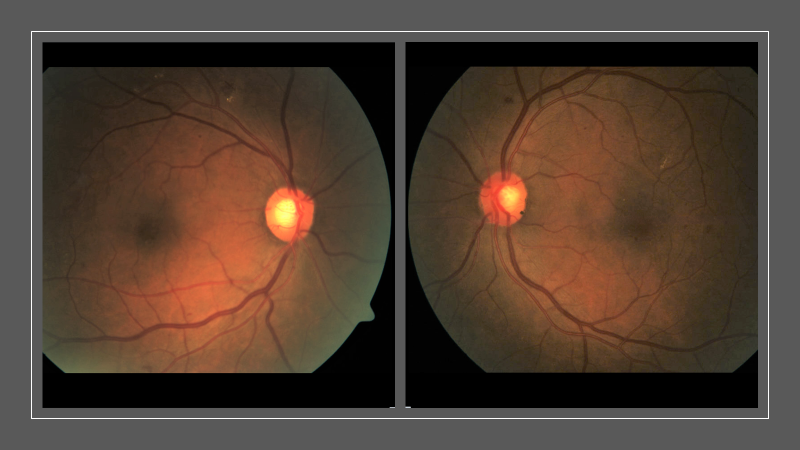
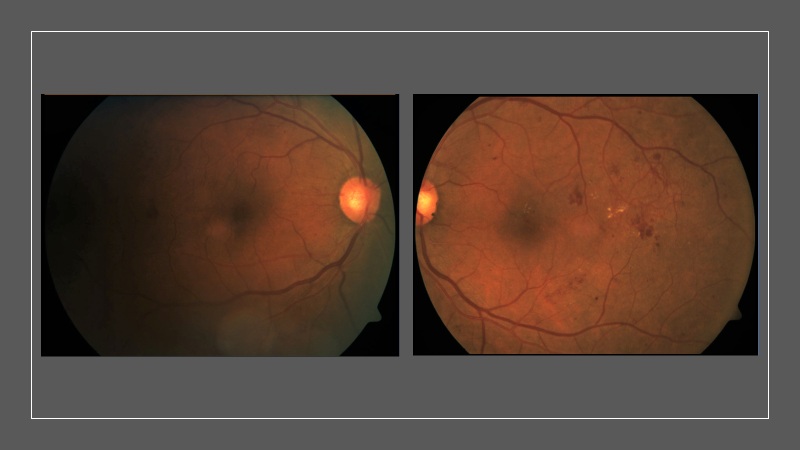
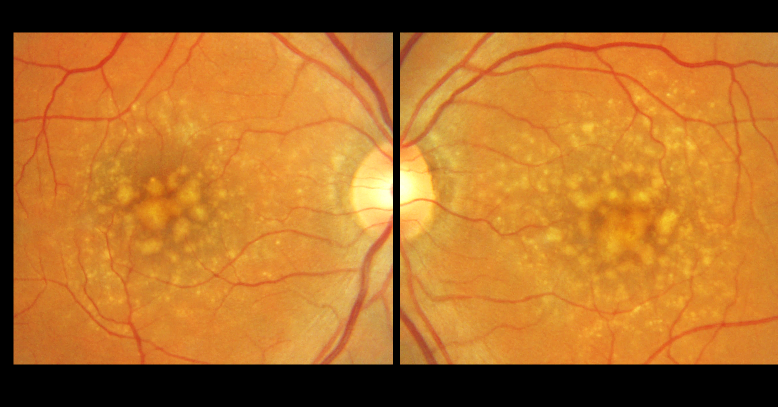
Her anterior segment exam was unremarkable, so we'll move to her posterior segment imaging. In these color fundus photos, some retinopathy is present, which is worse than in the past. She has some microaneurysms, most significantly temporal to the macula in both eyes. She also has retinal hemorrhages evident superiorly and some areas of exudation, as well.

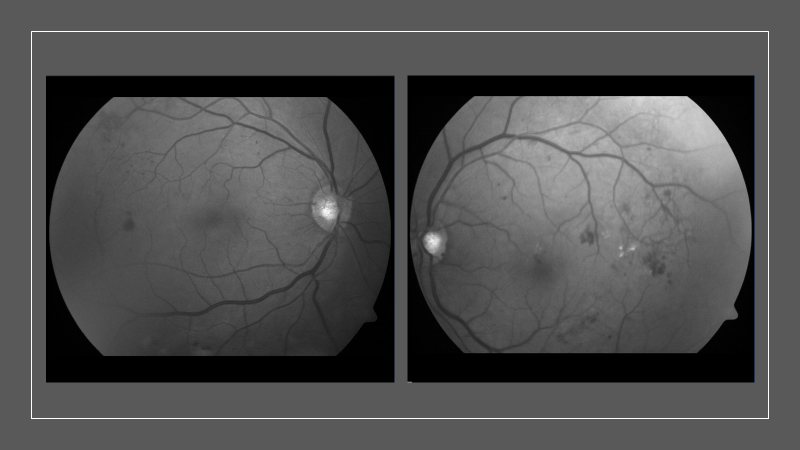
I sometimes do red-free photographs in these cases—especially if the retinopathy is more subtle or if the exposure wasn't right on the color photos. This technique really highlights the areas of hemorrhages, as well as areas of exudation.
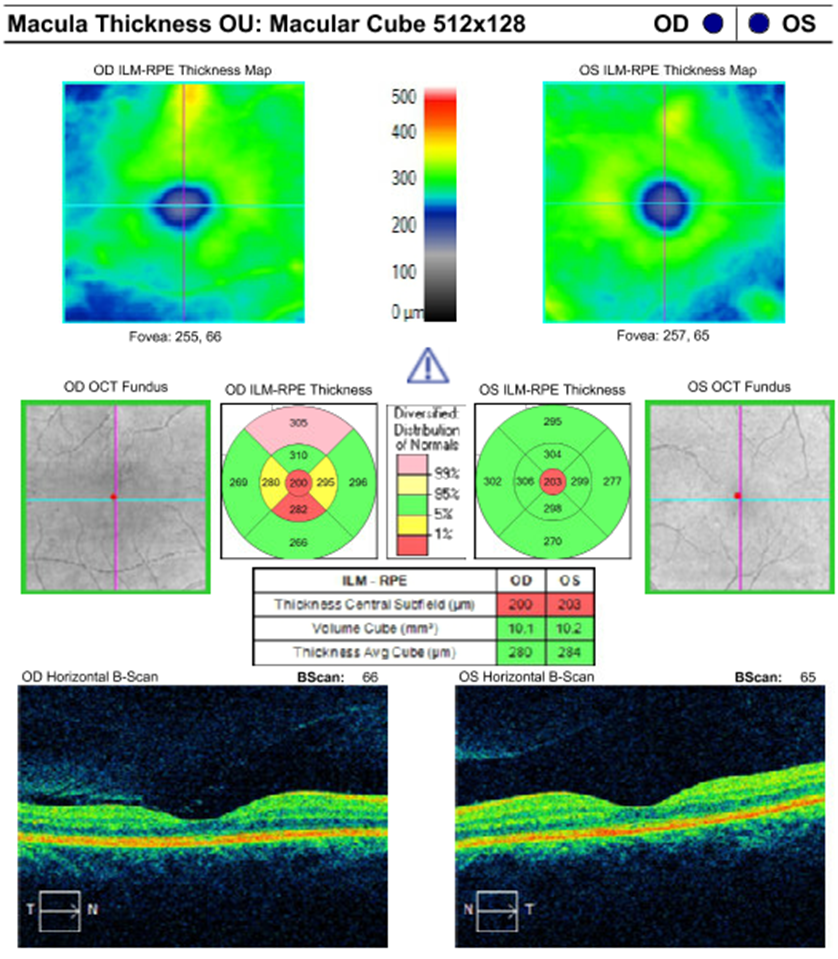
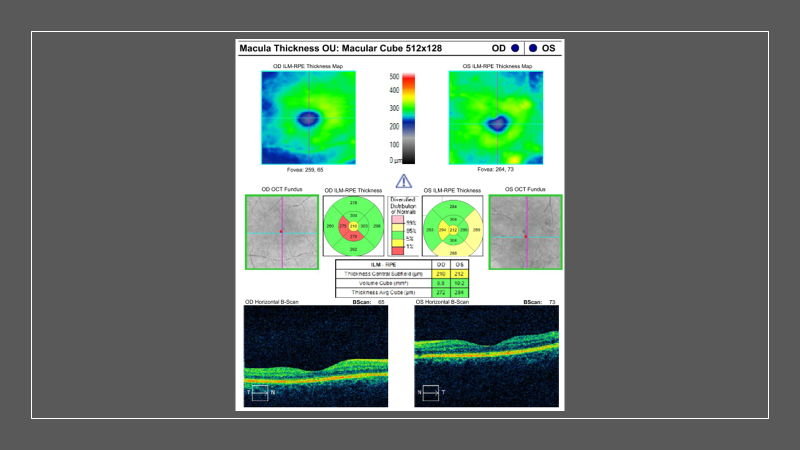
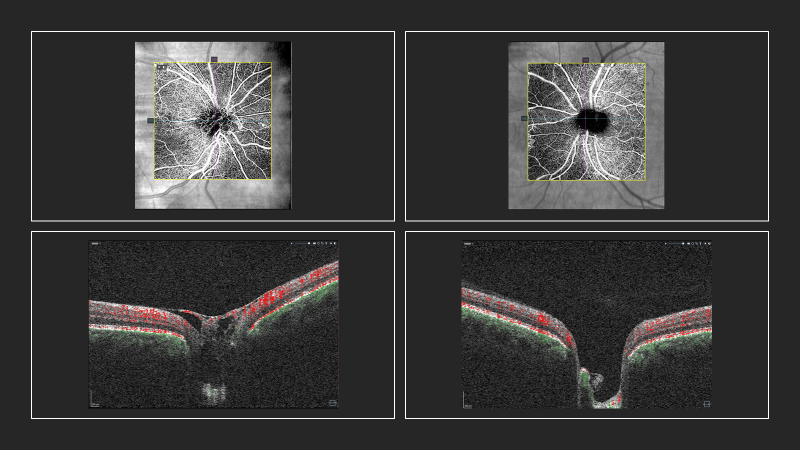
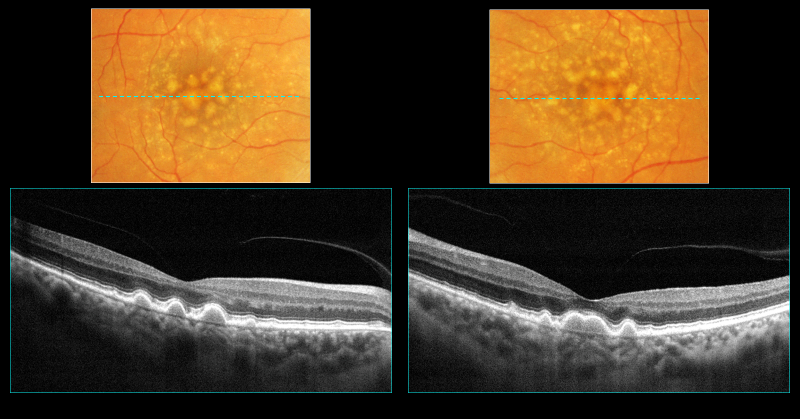
We didn't perform OCT at this particular exam. We brought her back three months later to do so, and we have her Mac Cube posted here, which reveals the development of some macular edema. She has an area of retinal thickening superior to her macula in the right eye and a trail of exudates moving inferiorly, affecting the central macula, as well.

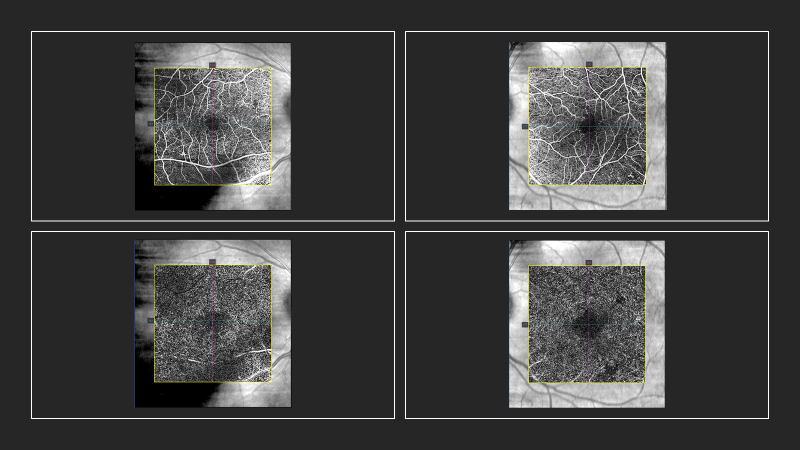
We also performed OCT angiography at this visit. What I've pulled here is her superficial capillary plexus at the top and the deep capillary plexus at the bottom. Of note, we actually can see that large retinal hemorrhage with the shadow and that area of exudation, inferiorly. But what I'd like to focus on is the foveal avascular zone. As we can see in the left eye, it looks a little bit smaller than it does in the right eye. In both, it's actually a bit enlarged. And this, we know, is a hallmark of diabetic retinopathy—we get an enlargement of the foveal avascular zone.
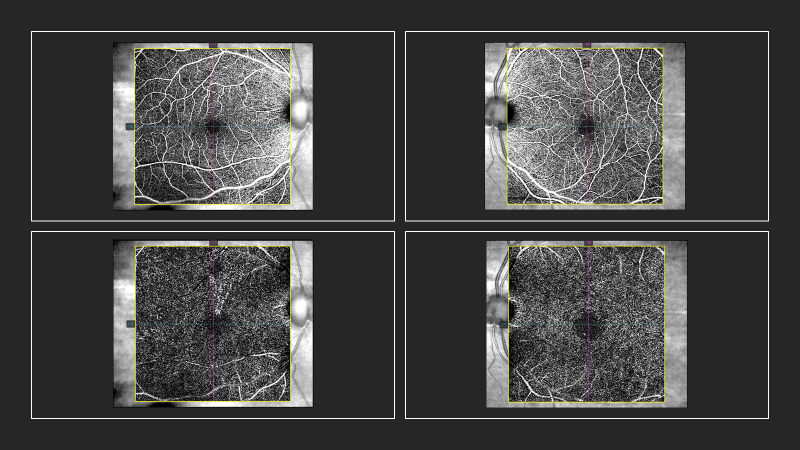
- When dealing with inner retinal disease, like diabetic retinopathy vein occlusions, it’s important to focus on those superficial and deep capillary plexus preset en face displays, exactly as presented here. - Dr. Majcher comment.
- Are you routinely getting an OCT or OCTA on your mild NPDR patients and moderate ones, or are you waiting until the retinopathy is more severe? - Dr. Parikh inquiry.
Years ago I didn't think it was necessary if there was not much retinopathy, especially in the area of the macula. Now that we have the ability to do OCTA, even if there aren't hemorrhages or exudate present centrally, I like to get a regular OCT and then specifically an OCTA to look for this area of ischemia.
- Agrees with getting OCT and OCTA studies, even if patient has early NPDR. - Dr. Parikh
- Notes that the OCTA provided of patient’s left eye highlights the importance of doing so. - Dr. Parikh
We diagnosed this patient at this time with moderate nonproliferative diabetic retinopathy in both eyes and macular edema present in the right eye. We now know that she had this significant area of macular ischemia, more evident in the left eye compared to the right eye. Our plan at this time was to educate our patient on the importance of improved control and also refer to a retinal specialist to evaluate that macular edema for possible treatment, since, although she was 20/20, it was central. It would be wise to also consider fluorescein angiography due to the documented ischemia in her retina.
Assessment/Diagnosis
- Moderate nonproliferative diabetic retinopathy OU with macular edema OD
- Diabetic macular ischemia OS>OD
Plan
- Educate the patient on the importance of tight glycemic control and follow-up care with PCP
- Refer to retinal specialist for evaluation of macular edema and possible fluorescein angiography
Unfortunately, this patient was lost to follow-up. We finally saw her three years later, at which time she was 64 years old. She presented still with her diabetic history, which had worsened. Her A1c was 12. Her fasting blood sugar was consistently elevated. She was on a third medication and she knew she was not well-controlled at the time. This was at the height of the pandemic in New York City. She was working from home, not exercising, not eating healthily, and aware that she let things slip. So, she came in for an eye exam.
64-year-old female presents for doctor directed follow-up
- Type II DM
- FBS 134
- A1c 12.0
- Medications
- Metformin 500mg BID
- Glyburide QD
- Actos 30mg QD
- BCVA
- OD: 20/20
- OS: 20/20
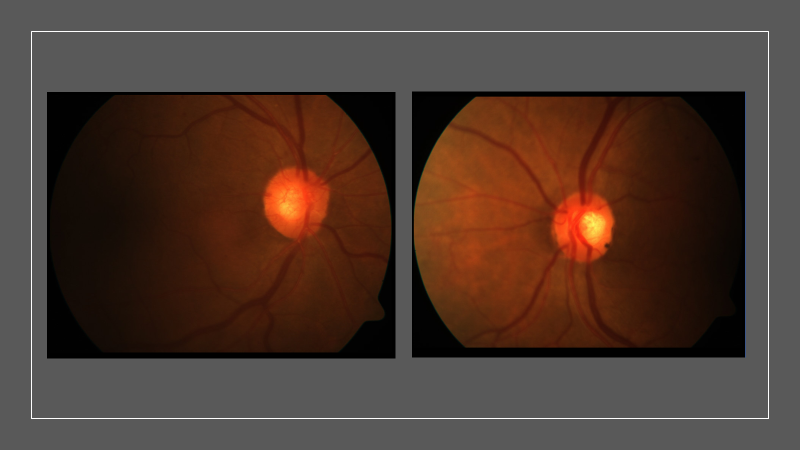
Her color photos revealed an escalation from a routine case to an extreme presentation, she now has proliferative disease. In the right eye, she has an area of pretty significant neovascularization of the right nerve. In the left eye, she has a very large area of neovascularization of her retina. We see more hemorrhages and exudation, as well.
Her red-free photos tell the same story, but provide a bit of a different perspective and highlight those areas a little better.
In the closeup picture of the nerve, it’s apparent how many neovascular blood vessels are present over that right disc.
We repeated her OCT, and luckily, it seemed that that edema that was present three years prior had since resolved. The patient did not have any history of reduced vision in either eye over the previous few years.
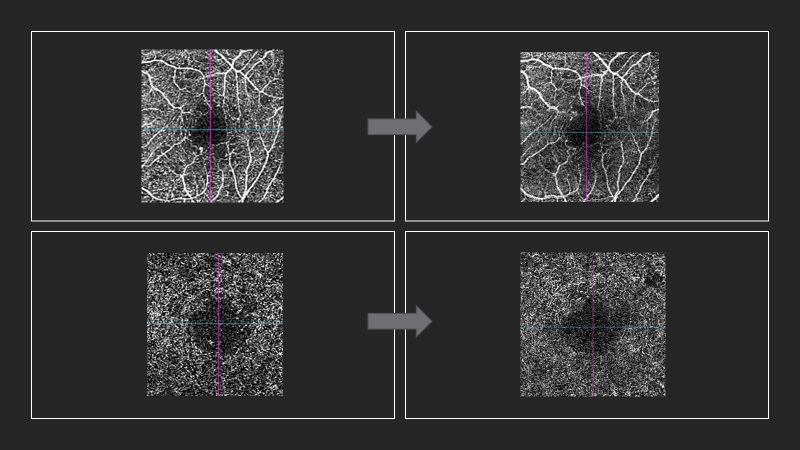
However, her OCT angiography reveals an enlargement of the foveal avascular zone compared to her original exam. We have those superficial layers on the top and the deep layers on the bottom. Overall, it looks darker and less saturated with capillaries, and there are more areas of capillary dropout, both within the fovea and paramacularly, as well.
Panel discussion:
- All three clinicians agree that the secondary impact of the pandemic on patients with eye disease has been unfortunate. - Dr. Gleason, Majcher, and Parikh.
- Many patients have been hesitant to maintain the follow-up care needed to prevent disease progression, especially at the height of the pandemic.
- As a result, it’s common to see patients with disease progression that may have been preventable with timely intervention.
- Patients with NPDR who still have 20/20 vision may not be aware of the underlying changes that are occurring.
Case presentation continued
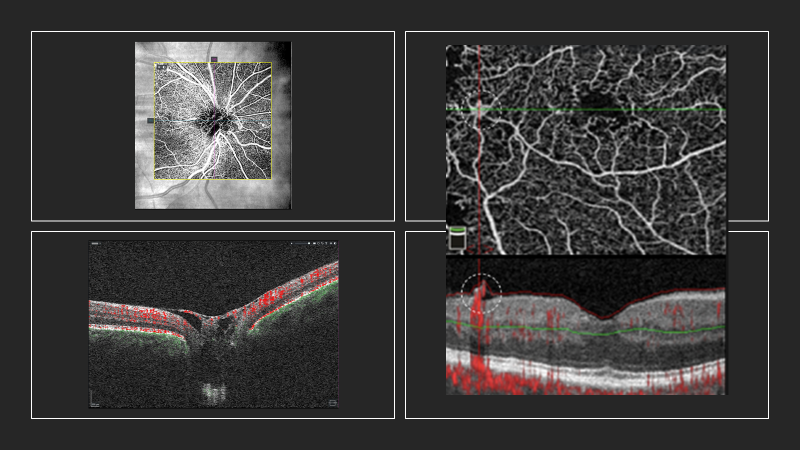
Anytime I'm suspicious for neovascularization of the disc, or I see it in my clinical exam, I always obtain an angiography over the nerve. Note on left nerve: this is a little bit of a segmentation error, which is why it doesn't look completely round. But in this particular slice of the OCTA, you want the nerve to look black, you don’t want to see any blood vessels on top of the nerve here. In the right nerve, it’s apparent how many blood vessels are there and how significant that neovascularization is. If you look at the bottom, we have our tomograms, which indicate areas of red, which indicate areas of blood flow. So remember, the OCTA is taking multiple B-scans repeatedly, looking for movement in the retina, and that movement is going to be blood flow. So you can even see within this neovascular net, over top of the optic nerve, she has blood flow.
I think even without OCT angiography—such as in offices that don’t have it—if you’re doing just structural raster scans through the optic nerve, you have that classic presentation of neovascularization on the disc, which I refer to as similar to a hammock hanging across the cup of that preretinal tissue. Sometimes, in patients who have bad cataracts or poor-fixation nystagmus, I'll use a raster scan to look around the posterior pole or scan across the nerve, looking for areas of tissue sticking up out of the retina that may signify preretinal neovascularization or, as in your case here, neovascularization of the disc. - Dr. Majcher
This is a great point because not everybody has OCTA capabilities now, but if you have OCT capabilities, you can still use those tools to pick up that neovascularization.
Unfortunately, in this patient the OCTA did not capture that area of retinal neovascularization, but I did pull an image to demonstrate what that would look like. This is showing that area of retinal neovascularization, and as was just mentioned, we know that this blood vessel should not be growing on top of the retina. So you don't even need it to say that there's blood flow in the area. If you see a vessel that looks anomalous and you do an OCT through the area, you can really document that neovascularization quite well.
Dr. Parikh, I'm curious to have your input on that. Is it unusual to see patients who have neovascularization within that macular scan? It seems that in many of the patients I'm seeing who are type 2 diabetics, a lot of the neovascularization occurs in the arcades and out toward the mid-periphery. What's your experience? - Dr. Majcher inquiry to Dr. Parikh
Absolutely. You’re going to get a lot of variation in patients’ presentations, but I definitely agree. A lot of the neovascularization you're going to see is going to be in areas somewhere between ischemic retina and vascularized retina, so it'll be in the arcades and the periphery. Oftentimes you'll see NVD first, or at the same time. There can be various presentations, and I bet this patient has neovascularization elsewhere. The other thing I want to mention is that this patient’s eyes are at such high risk, and given the level of pathology these eyes can go south really quickly. Although she’s 20/20 right now, it’s good she finally got in to see you, Dr. Gleason, because if she had waited another six months, things may have been much worse. - Dr. Parikh
In terms of our plan for this patient, she was diagnosed with proliferative diabetic retinopathy in both eyes, we have that area of macular ischemia more significant in the left eye. We referred to our retinal specialist for treatment, and he opted to perform PRP in both eyes for this patient.
Assessment/Diagnosis
- Proliferative diabetic retinopathy OU
- Diabetic macular ischemia OS>OD
Plan
- Refer to retinal specialist for injection vs. laser
- PRP performed OU
Diabetic retinopathy: overview
Just an overview of diabetic retinopathy. We see it all the time in clinic, but it's nice to take a step back and remember what's going on in the retina in our patients. Nonproliferative disease, characterized by increased vascular permeability. In more mild stages, we see microaneurysms. As the disease progresses, we see more hemorrhages and exudates. As severity increases further, we'll see cotton wool spots, IRMA, and venous beating.
- Nonproliferative
- Increased vascular permeability
- Microaneurysms, hemorrhages, exudates, cotton wool spots, IRMA, venous beading
In proliferative disease, there is persistent retinal ischemia, which can lead to release of VEGF, which can lead to angiogenesis. Down the road, this may also lead to development of NVD and NVE, as we saw in the case above. Complications of this can include vitreous hemorrhage and tractional retinal detachments—all the things we want to prevent in our patients.
- Proliferative
- Ischemia --> angiogenesis
- NVD, NVE, vitreous hemorrhages, retinal detachments
Diabetic macular edema, which is the most common cause of reduced acuity in our patients. In this case there is a breakdown of the blood retinal barrier, leading to intraretinal accumulation of fluid. In our patient, this didn't end up being something as significant, but we see this very frequently.
Diabetes and the macula
- Diabetic macular edema
- Breakdown of blood retinal barrier
- Intraretinal accumulation of fluid
Diabetic macular ischemia: Although not frequently mentioned, it's something that's occurring in our patients. The retina is ischemic and that's why we worry about proliferation. This is characterized by capillary occlusion and atrophy. However, you will not document this in your patients if you're not performing angiography. Previously, we weren't going to refer our mild patients to get a fluorescein angiography since it's a quite invasive procedure, if it wasn't really indicated. However, with the advent of OCTA, we can actually document this on our patients very early on in the disease process.
What to look for
- Diabetic macular ischemia
- Capillary occlusion & atrophy
- Visible on FA or OCTA
I pulled up images of the patient's left eye—the areas of macular ischemia—and compared the visit three years prior with the visit three years later. It’s evident that she has an overall reduction in capillaries. It looks just a little dimmer, a little less saturated on the right side of the slide. You can appreciate how the foveal avascular zone is widened, and she has these areas paramacularly of that capillary dropout documented.
In terms of diabetic macular ischemia, we know this occurs when capillary occlusion and atrophy are present, and as with our patient, visual function generally is not affected unless the ischemia is very severe. There is a correlation of severity of ischemia with the severity of the retinopathy, and therefore it can be an indicator of a risk of progression to proliferative disease.
- Capillary occlusion and atrophy
- Enlargement of foveal avascular zone (FAZ) and paramacular areas of capillary nonperfusion
- Visual function only affected in moderate to severe macular ischemia
- Correlation of severity of ischemia with severity of retinopathy
- Indicator of increased risk of progression to neovascular complications
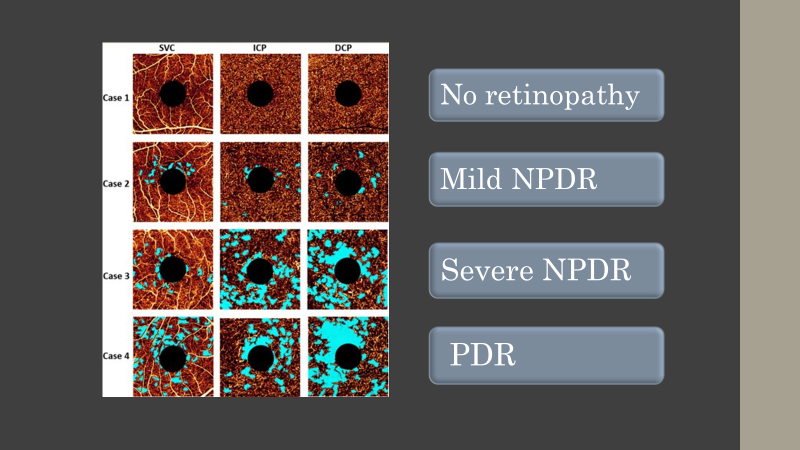
There are many studies on this topic. Expublished by Sheng You, et al. in 2020,1 which confirms those factors. If there's macular ischemia present, the patient may be more likely to progress to proliferative disease and that we should consider earlier referral and a more frequent follow up schedule.
This is a figure from that study. The areas of blue are showing areas of capillary dropout, and you can see that capillary dropout significantly increases with the severity of the disease.
Just some clinical pearls to wrap up this case. For every patient, the goal of doing these clinical exams is to preserve vision. Every time we're examining our diabetic patients, we're trying to determine the risk of vision loss in this patient's lifetime. When do we need to see the patient back to ensure that we catch it, if there is going to be vision loss, and when is treatment indicated? Diabetic macular ischemia is something that we should be looking for. If you have the ability to run OCTA on your diabetic patients, I recommend running it on all of them—regardless of level of retinopathy—because we know that it could be useful in determining how frequently you want to see that patient back. It will help us better care for our patients and hopefully better preserve their vision.
Clinical pearls
- Primary goal in taking care of our diabetic patients – preservation of vision
- Determine risk of vision loss
- Determine if treatment is indicated
- Diabetic macular ischemia may be a useful indicator in predicting progression to proliferative disease
- Consider using OCTA as an additional tool to determine follow up schedule and referrals for intervention
Discussion
Dr. Parikh:
- Great case, agrees with all points.
- Also important to remember that patient doesn’t really appreciate decrease in vision until severe ischemia present.
- Therefore, purpose of OCTA testing is twofold: Prognostication to inform the follow-up schedule and patient education.
- Showing patients their OCTA images can help them better understand presence or risk of disease progression and better engage them in follow-up and treatment.
Dr. Gleason:
- Agrees. Having OCTA images to show this patient helped her to understand the need for treatment by a retina specialist and improved her compliance moving forward.
Case study of 60-year-old female: routine to extreme case in retinal disease
Case study presentation by Dr. Majcher
Patient is a 60-year-old American Indian female who came in for an AMD follow up. She had no vision complaints and hadn't noticed any changes on Amsler in her vision. She had been diagnosed with macular degeneration (dry form) two years ago, was taking AREDs only, and hadn't had any other type of ocular treatment like anti-VEGF. In terms of medical history, she had some prediabetes and high cholesterol. She was a former smoker, which we know is a risk factor for macular degeneration. Her best corrected visual acuities at this baseline visit were 20/25 minus one in the right eye and slightly reduced 20/30 minus one in the left.
60yo American Indian female
- No vision complaints, no changes via home Amsler screening
- Dry AMD x 2 yrs, taking AREDS 2
- Med Hx: preDM, dyslipidemia, former smoker
- LEE approx. 15 months ago
- BCVA OD: 20/25-1, OS: 20/30+1
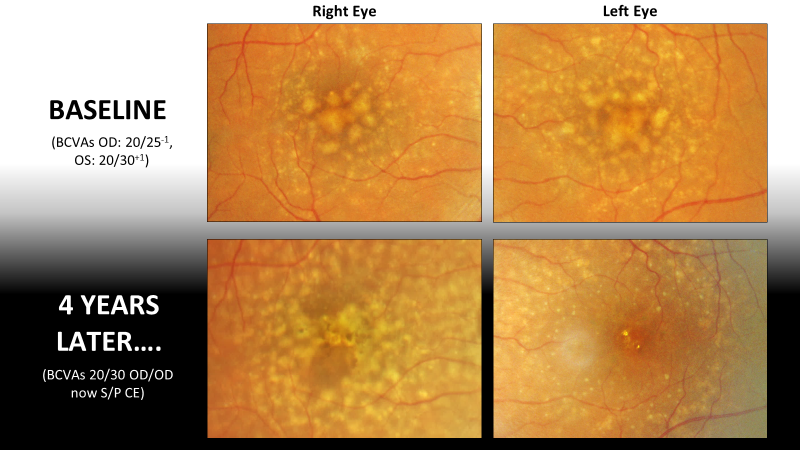
Here, we're looking at her color fundus photographs magnified on the macular region. Both eyes have large-sized soft drusen of greater than 125 microns and you only need one large-size drusen to put you into the intermediate stage of a nonexudative macular degeneration. So that's clearly what she has in both eyes, assuming no neovascularization is present. The drusen centrally are usually where we think are probably soft drusen because they have these indistinct borders, but there's another subtype of drusen that we can see in this patient's color fundus photographs, which are these small discrete focal deposits in the perimacular region.
Dr. Parikh, Would you mind commenting on what you think this other variant of drusen might be and what is the clinical significance of that for you?— Dr. Majcher inquiry
Dr. Parikh:
- Can use additional imaging modalities (OCT, perhaps autofluorescence) to help differentiate drusen, especially depending upon what layer they're in.
- These may be subretinal drusenoid deposits, aka, reticular drusen or pseudodrusen, which tend to have a poorer prognosis, as do soft drusen.
- AMD doesn’t become intermediate all of the sudden—patients have typically had it for years.
The patient’s raster OCT scans for each eye through the center of the macula reveal these soft drusen as large round elevations of the RPE. There are other subvariant of drusen seen, which are subretinal drusenoid deposits. It's nasal in the left eye, where we have this nodular hyperreflective deposit that’s anterior to the RPE. So it's sitting on top of the RPE in the subretinal space. And of note, there are no signs of neovascularization or exudation here.
Question for Dr. Gleason:
What would you be looking for on the fundus exam or OCT that would indicate exudation?
Dr. Gleason:
- Look for breaks in Bruch’s membrane.
- Identify areas where neovascularization might be growing and presenting itself through the retina.
- Observe any indication that subretinal fluid is present, which may be difficult to detect if extensive, overlying drusen cover it up—which is why OCT very helpful in these cases.
As discussed, OCT can be used to classify various subtypes of drusen—like hard, soft, or these particular pseudodrusen or subretinal drusenoid deposits. Some research suggests that subretinal drusenoid deposits are high-risk biomarkers for conversion, as Dr. Parikh pointed out. Not only for neovascular conversion, but also for conversion to atrophic advanced AMD, which is like central geographic atrophy. This is just one study that demonstrated that if you have a combination of soft drusen—which we typically think of as high-risk—with the subretinal drusenoid deposits, that puts you at an even higher risk than if you just had soft drusen alone. So this patient is at one of the highest risks for conversion to neovascular AMD that we could possibly have, based on the drusen subtypes present.
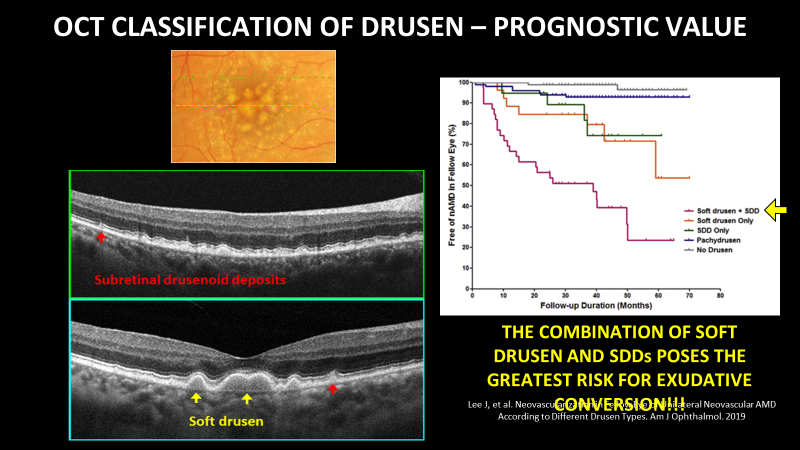
- Recent research presented at the ASRS meeting found substantial link between subretinal drusenoid deposits and cardiovascular disease. - Dr. Parikh comment.
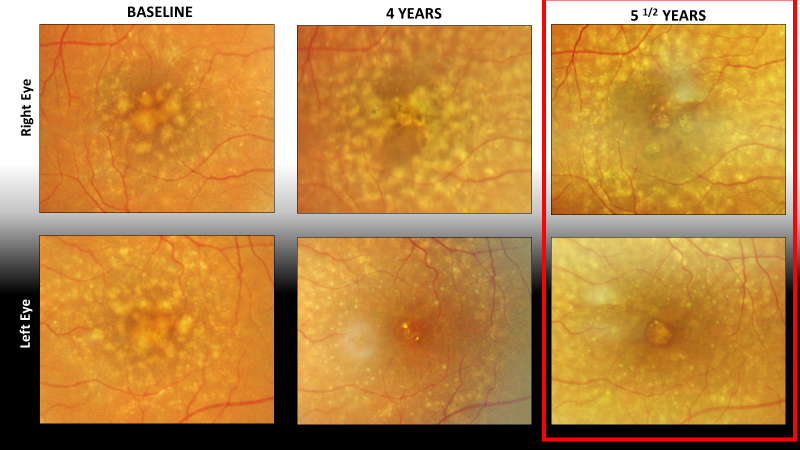
In this patient’s case, if we fast forward four years, we see we've had drusen regression in both eyes. The right eye has slightly more pigmentary changes, which are another high-risk biomarker for progression to advanced AMD. In the left, it looks like most of that drusen has gone away. Although that may seem a good sign, drusen regression is actually a risk factor for progression to advanced AMD—especially the geographic atrophy form.
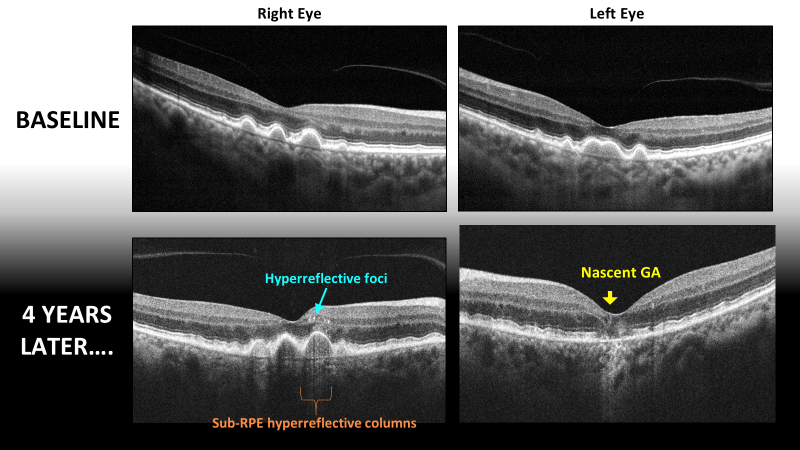
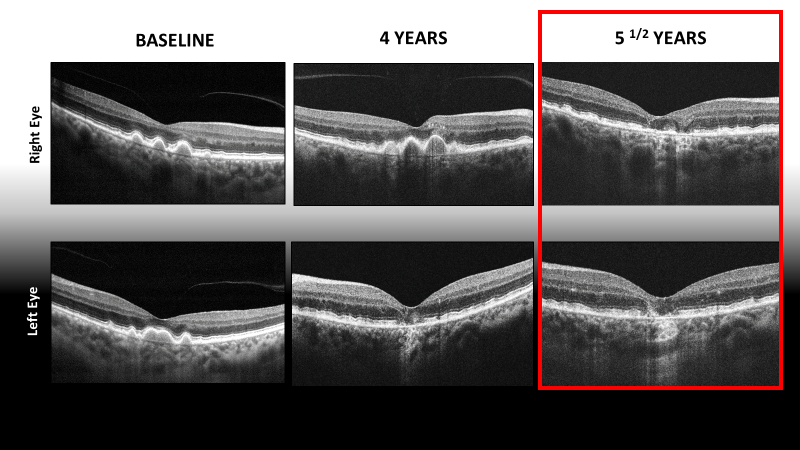
Results of her OCTs help confirm current status. In the left eye, at baseline, we had this large confluence of soft drusen. At the four-year follow up, those drusen have collapsed, and we're starting to form nascent geographic atrophy. I like to think of this as impending geographic atrophy, where we have a hypertransmission choroidal signal due to attenuation or loss of the RPE, and the outer plexiform layer seems to be sinking into that pit. We know this lesion is probably going to go on to develop full-blown geographic atrophy with complete atrophy of the photoreceptors and RPE.
Some other high-risk biomarkers on OCT that have formed in the right eye over the past four years are these hyperreflective foci, which are little hyperreflective deposits that are often on top of the apex of drusen. These also represent high risk for conversion to advanced AMD, as well as these hyperreflective columns, which are these vertical bars of hypertransmission telling you that the RPE on the apex of this drusen is compromised.
In this phase of the disease process, when seeing these signs of progression that indicate a poor prognosis, there isn’t a lot we can do for them except to watch them get worse. How do you navigate those conversations? - Dr. Gleason inquiry
Dr. Majcher:
- Since patients aren’t typically symptomatic at this point, I’m usually more concerned about conversion than they are.
- When I want to increase monitoring frequency, they may not understand the need.
- It’s important to provide education about taking AREDs 2. If they’re not already taking it, would recommend they start—though I think there’s little support showing that it decreases conversion to GA vs neovascular AMD.
- Consider a discussion with the patient about lifestyle changes, ie, stop smoking, UV protection, dietary modification.
- Not much more we can do at this time, but hopefully that will change in the future.
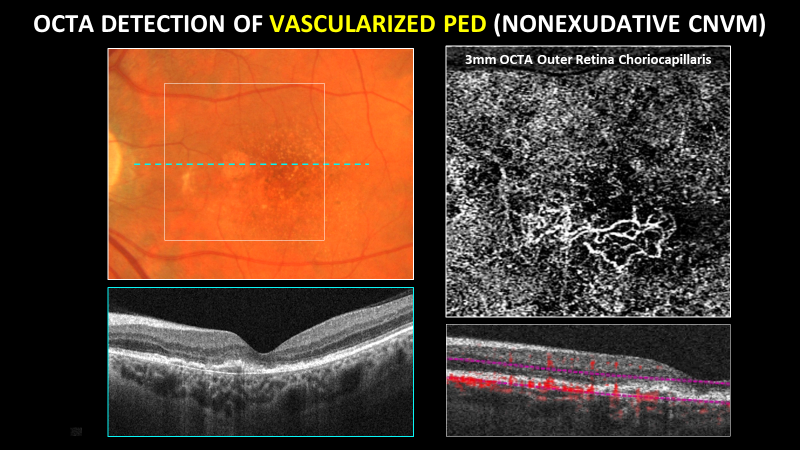
OCT angiography is very valuable in detecting early neovascularization because it allows direct visualization of the membrane itself, not just the secondary exudative effects of fluid or other factors. Anytime I have a patient—like this patient's right eye—where there's a large drusenoid —presumably drusenoid—pigment epithelial detachment (PED), I'm going to position my segmentation lines on OCT angiography so I'm sandwiching that PED. I want to see what's inside that PED sandwich and whether there’s neovascularization in there. If I'm looking at the en face image, neovascularization looks like a well-formed vascular net. This patient has atrophy of the choriocapillaris, which is a characteristic feature of atrophic macular degeneration.
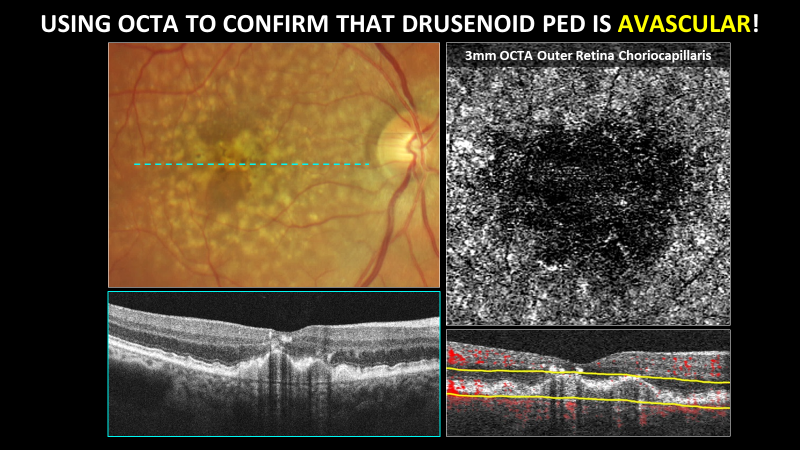
This image puts that into context and demonstrates the contrast with a pigment epithelial detachment that is vascularized. There's a shallow irregular pigment epithelial detachment, and on OCT angiography, we see this well-formed neovascular net—definitely something I'm going to refer to retina for a second opinion. This patient may benefit from anti-VEGF therapy.
Let's now fast forward to five and a half years of follow up. In the right eye, there’s even more drusen regression and we're starting to see multifocal, geographic atrophy forming in the right eye, even centrally. On the left eye, frank geographic atrophy has formed centrally about one third disc area in size. It seems bigger than previously.
On OCT, again, we have almost complete drusen regression in the central fovea of the right eye, and we now have impending geographic atrophy lesions, where the retina is sinking down towards these areas of RPE atrophy with choroidal transmission defects, as well. In the left eye, the area of geographic atrophy seems to have enlarged compared to just one year ago.
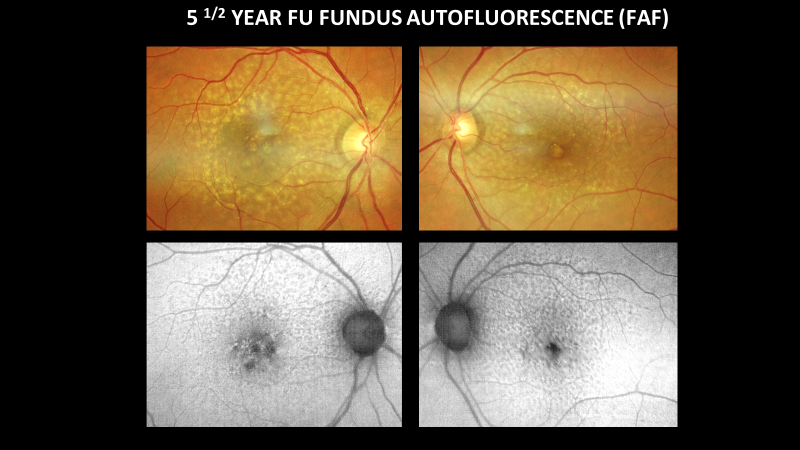
I think fundus autofluorescence has a lot of value in this case, for two reasons. One is looking at reticular pseudodrusen, which can be difficult to see with color fundus photography alone. They look like dark, hypoautofluorescent deposits on fundus autofluorescence. This kind of reticular pattern is really a classic presentation of pseudodrusen. Fundus autofluorescence also helps you delineate areas of geographic atrophy and monitor them over time. When you have atrophy of the RPE, that's going to appear dark or hypoautofluorescent on FAF imaging.
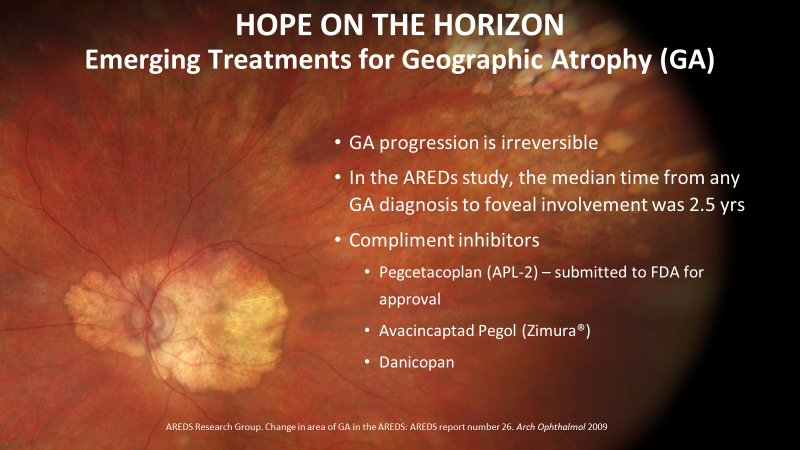
Unfortunately, geographic atrophy is irreversible, and foveal involvement can actually occur faster than most realize. When we think about geographic atrophy, we may assume it’s slowly progressing and there’s really nothing we can do. Actually, it can take as long as two and a half years for extrafoveal GA to progress to the point at which the center of the fovea is involved. Fortunately, there is hope on the horizon for these patients with geographic atrophy and nascent geographic atrophy. There are several pharma companies working on treatment options, mostly complement inhibitors. Most of them are intravitreal injections, though one I’ve listed here is oral and under investigation. So there's really an exciting future to come, I think, for the treatment of geographic atrophy. Since the first drug will probably be available on the U.S. market by the end of this year, we need to identify these patients now that have geographic atrophy, especially extrafoveal GA, who may benefit from slowing the progression in hopes of stabilizing vision.
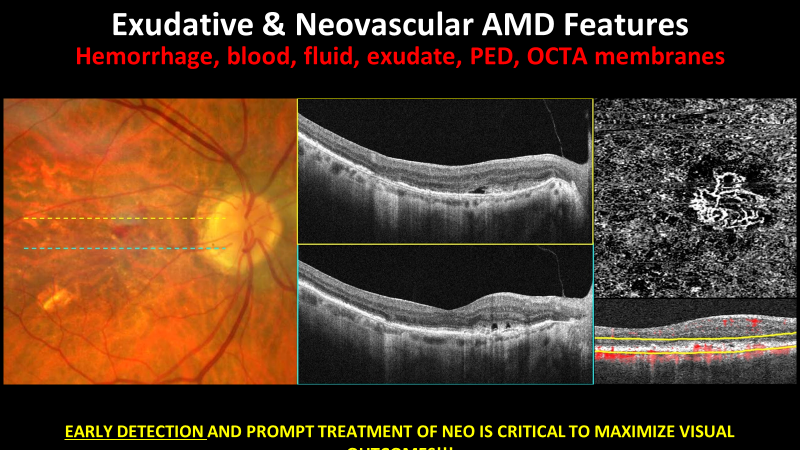
Let's now switch gears and talk about the more extreme and visually devastating form of AMD, which is neovascular AMD. While only about one fifth of AMD cases are exudative, neovascularization accounts for 90 percent—the majority of severe central vision loss from macular degeneration. So early detection by anyone—whether it be eyecare professionals or the patient—is crucial. You need to be looking on fundus examination for hemorrhage, for exudate, for grayish-green subretinal thickening. On OCT, you want to be looking for fluid, pigment epithelial detachment—especially if it's an irregular contour that has a weird internal reflectivity. Or on OCT angiography, if you're seeing a frank choroidal neovascular membrane, that should all be concerning to you and you need to refer that out. The earlier we treat, the better the visual outcomes.
Case study of 73-year-old female: routine to extreme case in retinal isease
Case Study Presentation by Dr. Majcher
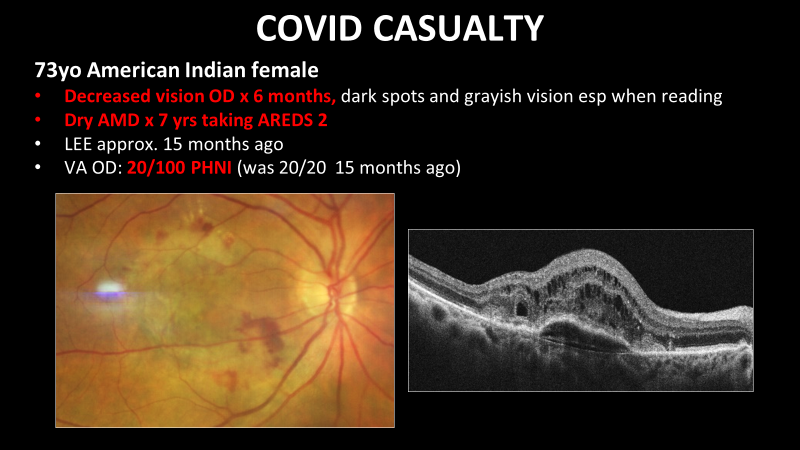
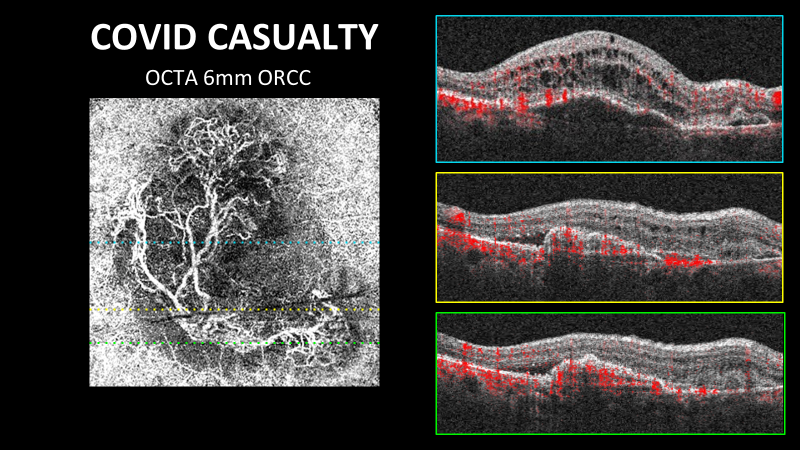
Similar to the case Dr. Gleason presented, this next case is about a patient who fell by the wayside because of COVID. This was a 73-year-old American Indian female who complained of decreased vision in the right eye for the past six months. She had a history of dry macular degeneration for which we were following her for several years. She missed two appointments, fell by the wayside for about 15 months and showed up as a walk-in to our emergency clinic. Her vision at this point was 20/100. We had previously had her documented as 20/20. If we look at her color fundus photograph, we have this classic grayish green, subretinal thickening with an adjacent subretinal hemorrhage and retinal exudate, all features of exudative AMD.
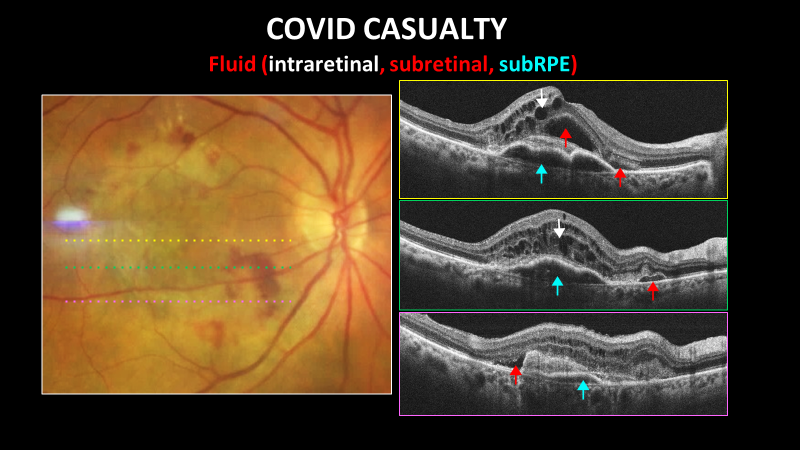
Next are several different structural OCT raster scans through her macula. In the center area of the macula, we have fluid at pretty much all levels possible. We have intraretinal fluid. We have subretinal fluid. And we have this irregular contour, multi-lobed pigment epithelial detachment that probably contains mostly fluid. There is also a subretinal hyperreflective mass, which is the membrane itself—as well as a subretinal hyperreflective mass in the inferior macula. Again, this is the membrane itself, exuding intraretinal, subretinal, and subRPE fluid.
On OCT angiography, this is the en face image, 6mm scan, so you can imagine how huge this choroidal neovascular membrane is. It's very mature with large feeder vessels associated with it. On the B-scan overlay, as Dr. Gleason mentioned earlier, the red aspect on top represents blood flow on top of your traditional structural OCT scans. Remember that hyperreflective mask we had? With the structural imaging, it highlights in red. That's the area of neovascularization that's sandwiched between the RPE and the retina. We can also see the lumens of the large feeder vessels sitting in the subretinal space.
Comments from Dr. Parikh:
- Such amazing images clench the diagnosis.
- He’s had some success in treating patients with this level of severity by reducing fluid through a series of anti-VEGF injections.
- With current treatment options, vision loss at this level of severity will never return to 20/20, but may gain some improvement.
Take Home Message:
- Recognize OCT biomarkers for conversion from intermediate nonexudative AMD to advanced AMD.
- Begin looking for patients with GA and nascent GA that may benefit from future therapies.
- Know the features suggestive of exudative AMD (blood, fluid, PED, etc) like the back of your hand.
- OCT/OCTA allows for earlier detection of neovascularization and exudation in AMD = Earlier treatment = Vision preservation.
- OCT & OCTA can be valuable in monitoring for CNV regression and need for anti-VEGF retreatment.
Q&A
How frequently are you seeing your patients with mild to moderate NPDR and how frequently are you imaging them, with either OCT or OCTA?
Dr. Gleason:
- Mild NPDR patients generally seen anywhere from every 6 months to every year.
- Normally follows them yearly, but in some instances, feels more frequent evaluations are needed.
- For barely moderate patients, every 6 months typically works.
- If developing more areas of ischemia, will see them every 3 to 4 months.
- Eval frequency is not necessarily based on patient’s stage, but on what imaging reveals.
- Advanced imaging techniques like OCTA enable more insights about ischemic areas and the potential to develop proliferative disease.
Dr. Majcher:
- Mild NPDR patients usually monitored every nine to 12 months.
- Moderate NPDR patients usually monitored every six to nine months, depending on how many risk factors present.
- Mac OCT done about yearly for moderate NDPR patients.
- Thinks imaging plays a greater role in more severe stages of disease, like severe NPDR versus early PDR.
Dr. Parikh:
- Also considers patient’s A1c when determining monitoring schedule.
- Would take a different approach to patient with moderate NPDR and an A1c of 12 compared to patient with moderate NPDR, recently diagnosed with diabetes, and A1c of 6.8.
Dr. Gleason had a good photo of NVE that was caught with OCTA. Dr. Majcher, you have some great cases in that context. Can you share some of those photos in which early NVE or even late NVE is captured on OCTA imaging?
Dr. Majcher:
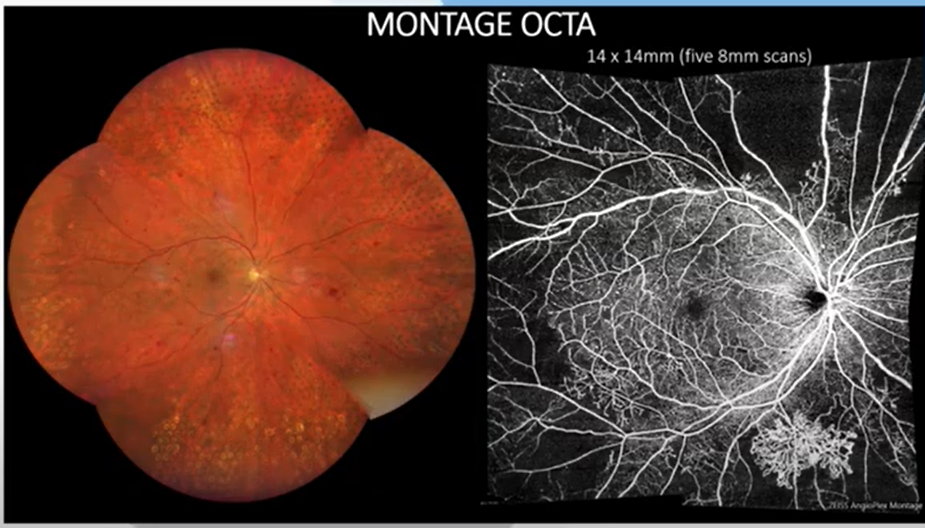
- One of the best ways to identify NVE is by using montage OCT angiography imaging.
- Exciting development that’s become available in past few years on most OCT angiography machines.
- Montage imaging allows for extended field-of-view imaging of the vasculature outside of the arcades in patients with diabetic retinopathy.

Dr. Majcher:
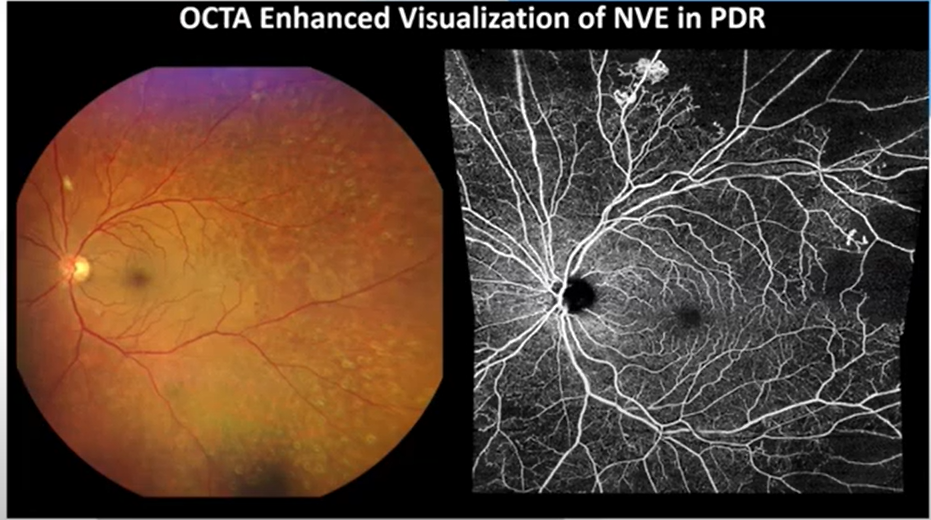
- High resolution microvascular detail enabled by OCT angiography supports visualization of small microvascular pathologies that might not be detectable with fundus examination.
- Supports more accurate disease staging.
Dr. Majcher:
- The volumetric data set of vascular information obtained from OCT angiography that can be segmented out can also be segmented out with OCT angiography montage.
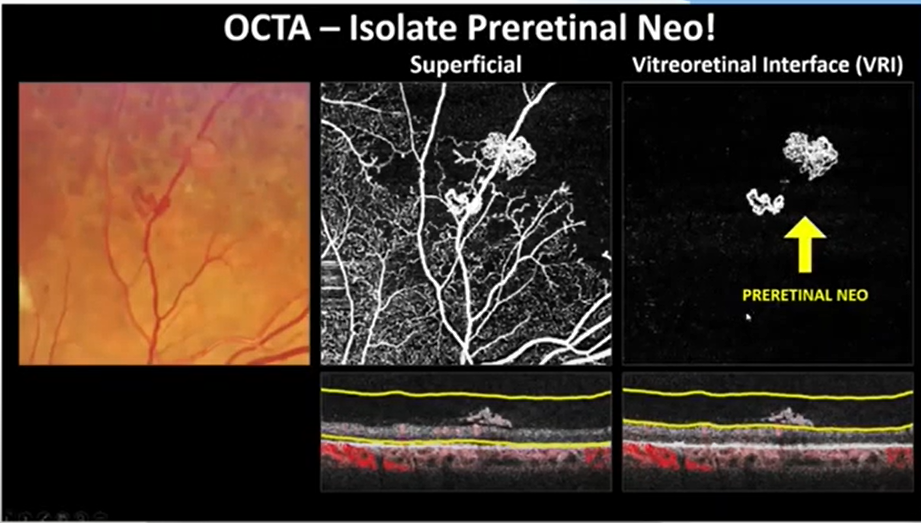
- Vitreoretinal interface is one of the best presets to look for preretinal neovascularization.
- Important to look for preretinal neovascularization on the border of perfused and nonperfused retina.
- OCT angiography montage makes it really easy to identify that border and inspect along it.
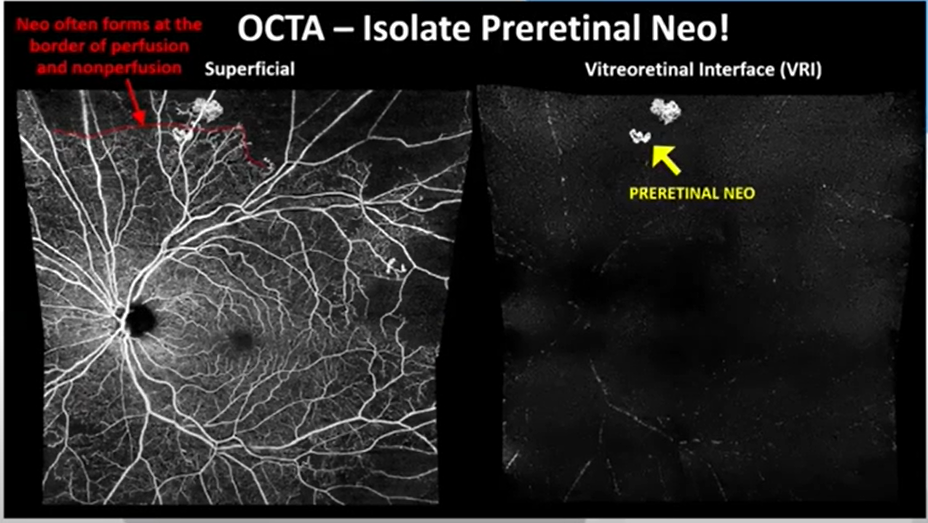
- The vitreoretinal interface preset en face display reveals any vascular data anterior to the internal limiting membrane where preretinal neo usually grows.
- So look at the vitreoretinal interface to identify early cases of proliferative diabetic retinopathy that probably deserve PRP and need to be referred out.
Dr. Parikh:
- Excellent images and insights
- Frequently uses fluorescein angiography and now considering using OCTA montages more.
- However, if assessing for something like vasculitis, will not be able to identify it on OCTA and will still need to use fluorescein angiogram.
Poll question for participants: Upon observation of drusenoid regression, how would you change your management?
Results:
- Monitor more often (38%)
- Order an OCTA scan (35%)
- Continue management as planned (23%)
Dr. Gleason, what do you think of those results? Where would you fall in this poll?
Dr. Gleason:
- I love the split between the first two options, because also may want to do both.
- Would want to increase monitoring frequency, but also obtain OCTA scan if one not already done.
- Priority would be obtaining an OCTA scan.
Poll question for participants: Which of the following patients would most benefit from an OCTA scan?
Results:
- Neovascular AMD (49%)
- Intermediate dry AMD (41%)
- Early dry AMD (10%)
Dr. Majcher, what do you think of those results? Where would you fall in this poll?
Dr. Majcher:
- Both neovascular AMD and intermediate dry AMD are very appropriate responses, but would prefer intermediate dry AMD.
- As a primary eyecare provider, it's my job to detect the earliest neovascular AMD, the early exudation and activity, and refer that out for prompt treatment.
- Monitoring intermediate dry AMD patients with risk factors for progression to neovascular exudative disease is absolutely critical with OCT and OCT angiography to assess for neovascularization.
Question from participants for the panel: With more people turning to various types of self-service eyecare—like purchasing eyeglasses online—are we missing some disease and/or is it presenting later?
Dr. Gleason and Dr. Majcher:
- Absolutely, is a common trend.
- Underscores the critical importance of patient education when the patient is in the office—and using images as part of that process can be very effective.
Final takeaway from Dr. Parikh:
As our field is advancing, we really want to give our patients hope that there are a lot of treatments on the horizon. If we can help our patients maintain hope and continue to progress as a field, I think there will be a great deal of benefit to a lot of patients in the future.
