


WHAT YOU'LL LEARN
Recognize the unique features of FCNP
Know the common tests for FCNP and their diagnostic reliability
Understand when neuroimaging is indicated for FCNP
Introduction
Introduction
It is well recognized that a fourth cranial nerve palsy is a common cause of vertical strabismus in children and adults. However, just the idea of vertical strabismus or diplopia can elicit a visceral reaction from eyecare providers. The objectives for this course are to specifically recognize the causes, clinical presentation, and management of fourth cranial nerve palsies (FCNP). Because of the implications of FCNP on vision development, social concerns, and possible adverse health outcomes, increasing our understanding in this topic can have a far-reaching impact in our patients’ lives.
Background and Etiology
Background
To understand FCNP, we must first review the normal physiology of the fourth cranial nerve and the superior oblique muscle (SOM). The fourth cranial nerve, the trochlear nerve, is one of the three cranial nerves that innervate the six extraocular muscles of the eye. This nerve takes a long trip from the brainstem to its final destination of the superior oblique muscle. Starting from the midbrain, the nerve exits dorsally, runs in the subarachnoid space, and enters the cavernous sinus. It then travels through the superior orbital fissure to innervate the SOM.
Unique features of CN IV:
- Has the longest intracranial course (susceptible to damage by trauma)
- Exits from the rear of the brainstem (the only cranial nerve that does!)
- Innervates a single muscle contralateral to its nucleus (all other cranial nuclei affect the ipsilateral side)
The SOM intorts, depresses, and abducts the eye. These actions arise from the relationship between the trochlea on the frontal bone and the angled insertion of the muscle on the posterior half of the eye.
Unique features of SOM
- Utilizes a pulley system with the trochlea
- Highlights different actions in different positions of horizontal gaze (better depression in adduction, better intorsion in abduction)

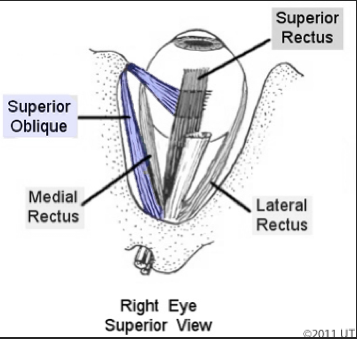
Source: UT Health Department of Neurobiology and Anatomy, color added for emphasis
Etiology
The majority of FCNP are congenital,1,2 but that is not synonymous with presentation in childhood exclusively. FCNP can have a delayed presentation into adulthood due to decompensation of the deviation.1 Recent research using MRI has differentiated congenital FCNP into two sub-types. Nearly three-fourths of patients with congenital FCNP actually lack a fourth cranial nerve and have a subsequent hypoplastic SOM, while the other fourth of patients have normal nerves and muscles.3
Trauma and microvascular disease are considered the most common causes of acquired FCNP. Even a mild blow to the head can cause a traumatic FCNP,4 and tends to be bilateral due to the anatomical course of the nerve. Microvascular disease such as hypertension and diabetes affects more commonly cranial nerves three and six,5 but has been shown to be involved in FCNP in approximately one-fifth to one-fourth of cases.1,2 Intracranial neoplasms are considered a rare cause1 and would often present with other neurological deficits, depending on the location of the lesion.
Diagnosis and Treatment
Clinical Characteristics
The classic picture of FCNP is a hypertropia that is worse on ipsilateral head tilt and ipsilateral face turn. As a result, patients with FCNP usually adopt a head tilt away and chin tuck from the affected eye to decrease the vertical misalignment6. However, there are many variations from this presentation. Within the sub-types of congenital FCNP, head tilt may appear earlier in patients with an absent nerve versus a functioning nerve.3 Patients with congenital FCNP who have a normal nerve may show a nasal upshoot or dissociated vertical deviation.3 A larger hypertropia in up gaze than down gaze can distinguish a congenital FCNP from an acquired FCNP.7 The horizontal deviation can also suggest the type of FCNP, with an exodeviation associated with microvascular acquired FCNP and an esodeviation with congenital FCNP.8 These paradoxical compensations may be due to a combination of underaction and overaction of other muscles.
Tests traditionally utilized to understand the type of FCNP have not been validated for diagnostic purposes. Most widely used is the Parks-Bielschowsky three-step test, which, when evaluated, has only a 50% to 70% sensitivity.9,10 Looking only at hypertropia in primary gaze and in head tilt increases sensitivity to 84%.9 Larger vertical fusional amplitudes were previously thought to be paradigmatic for congenital FCNP, but are not consistently so.7 Torsional misalignment is another factor with mixed diagnostic reliability.7,11

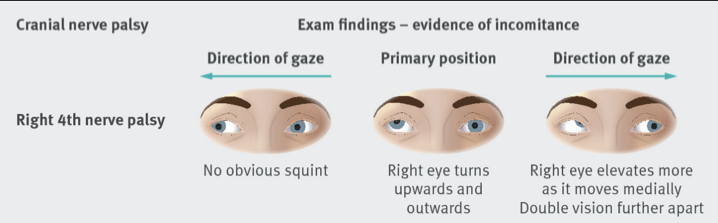
Source: The BMJ
Work-up and Treatment
Gathering pertinent information from your clinical exam is foremost, with special emphasis on patient history and binocularity testing. It is important to check for comitancy with cover testing in multiple positions of gaze. The phone app called 9 Gaze is a great supplementary tool for documenting extraocular motility testing. The three-step test, vertical fusional amplitudes, and torsional misalignment can add pieces of the puzzle, but should not be used to hang our hats on.
Management options focus on restoring binocular function and diplopia. For children with a congenital FCNP, early intervention is warranted for binocular vision development and ergonomic posture. Strabismus surgery has the potential for large changes in the amount of vertical deviation and head tilt.12 Watchful waiting for isolated FCNP can be appropriate, as clinical courses can normalize with time. The majority of FCNP due to microvascular disease can resolve spontaneously within 10 months without any intervention.14 Similarly, prognosis is favorable for recovery from traumatic FCNP within 6 months.15 While waiting for resolution, prisms up to 15 prism diopters can provide relief for patients with symptomatic diplopia.13 Occlusion can also be considered as an option to eliminate diplopia and improve torticollis.
Conclusion and References
The Role of Neuroimaging
The role of neuroimaging is evolving with emerging evidence and the variability of presentation of FCNP. Imaging is undeniably indicated for non-isolated (i.e., without other neurological deficits) FCNP and MRI would be the preferred evaluation method over CT. The yield for imaging on isolated FCNP is generally low,16 although there are studies and case reports supporting the use of neuroimaging to detect other potential comorbid causes.5,17,18 In conclusion, the level of concern should be driven by the total clinical picture, and neuroimaging can be used to corroborate clinical findings.
