



WHAT YOU'LL LEARN
The unique characteristics that distinguish various retinal lesions on OCT
How to use the OCT diagnostic report to aid in the management of retinal pathologies
Introduction
Introduction to OCT
Optical coherence tomography (OCT) is a non-invasive ocular imaging method that uses light waves to create cross-sectional images of ocular tissues at a micron level resolution. The OCT images are constructed according to the amount of light that is scattered and reflected from the individual ocular tissues. Scans may be viewed in grayscale or pseudo-color scale, both based on tissue reflectivity. OCT imaging can help identify a pathology, determine the severity, and guide management decisions.
OCT Terminology
An A-scan consists of a single one-dimensional axial scan of the eye, imaging the retina in the anterior-posterior axis. A collection of many adjacent A-scans can be merged to create a two-dimensional cross-section of the retina. This cross-section comprises the B-scan component of OCT imaging. Many adjacent B-scans can be merged to create a volumetric three-dimensional representation of the retina, called a cube scan. Alternatively, a raster scan can provide higher resolution than a cube scan, but is limited to only 5 parallel cross-sections through a given area of the retina. A radial scan is another higher resolution option that images several cross-sections arranged in a radial pattern centered on a particular area of interest, often the fovea.

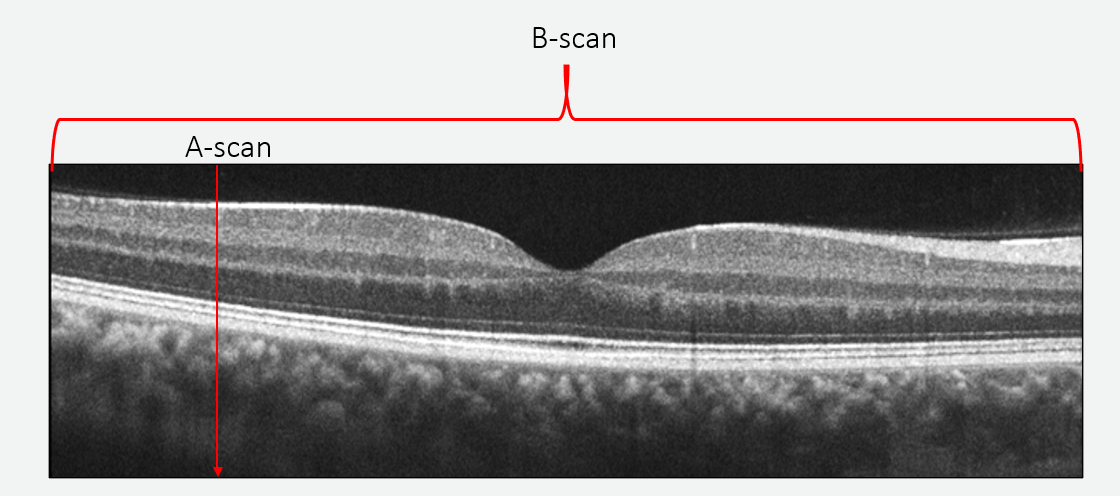
Figure 1: A B-scan is made up of many adjacent A-scans to create a “slice” of the retina.


Figure 2: A cube scan is made up of many adjacent B-scans to create a 3D representation of the retina.
OCT Basics
Homogenous structures allow light to pass through the material relatively undisturbed and therefore reflect little light back to the OCT. These structures appear as either dark grey or black, or as cooler colors. Homogenous ocular tissues include the outer nuclear layer, where the nuclei are tightly packed into a regular structure, and the vitreous. Areas of serous fluid will also appear dark on an OCT B-scan.
Heterogenous structures reflect significantly more light back to the OCT, so they appear as light grey or white, or warmer colors. In a healthy eye, the retinal nerve fiber layer (RNFL) appears nearly white in an OCT B-scan because the layer is very reflective. The outer plexiform layer and any areas of fibrous scarring also appear bright on an OCT cross-section.
The Normal OCT
When viewing an OCT of a healthy retina, layers that correlate to the anatomical and histological structures can be identified and evaluated. For example, the retinal pigment epithelium (RPE), ellipsoid zone, and external limiting membrane can be seen, should always be scrutinized because they correlate very well to visual acuity.

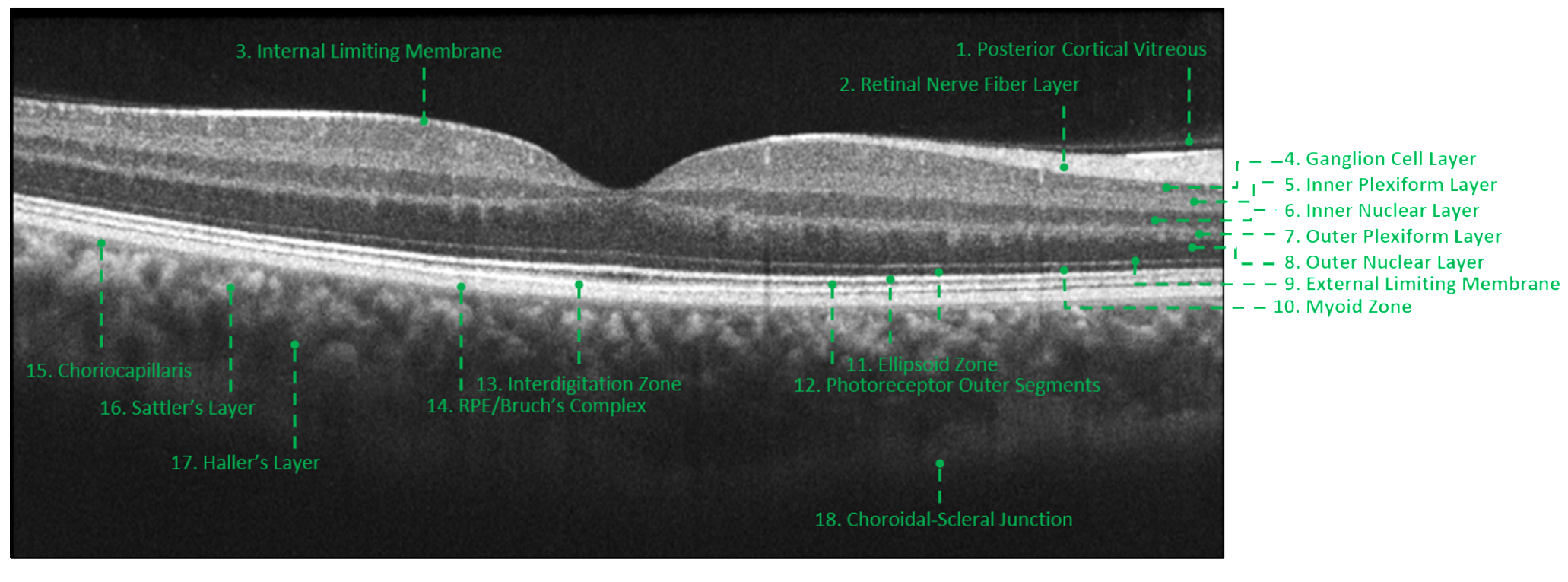
Figure 3: In this healthy macula, each layer of the retina can be distinctly identified due to differences in their reflectivities.
When viewing the OCT diagnostic report, begin by verifying the identifying patient information and date. Ensure the signal strength is acceptable: a strength of 9 or 10 is preferred, but 7 or 8 may be acceptable in certain circumstances. Next, review the retinal thickness map to gain a topographical overview of the area of retina being evaluated, then the quantitative map to ascertain numerical retinal thickness values. Review the B-scans included on the report to ensure the scan placement is accurate and centered over the area of interest. When evaluating a B-scan, it may be helpful to first locate the RPE. This is a useful landmark in most cases because it is relatively thick and bright on the scan, making it easy to identify. Then, depending on the pathology, focus anteriorly or posteriorly to the RPE to locate the layer of interest.

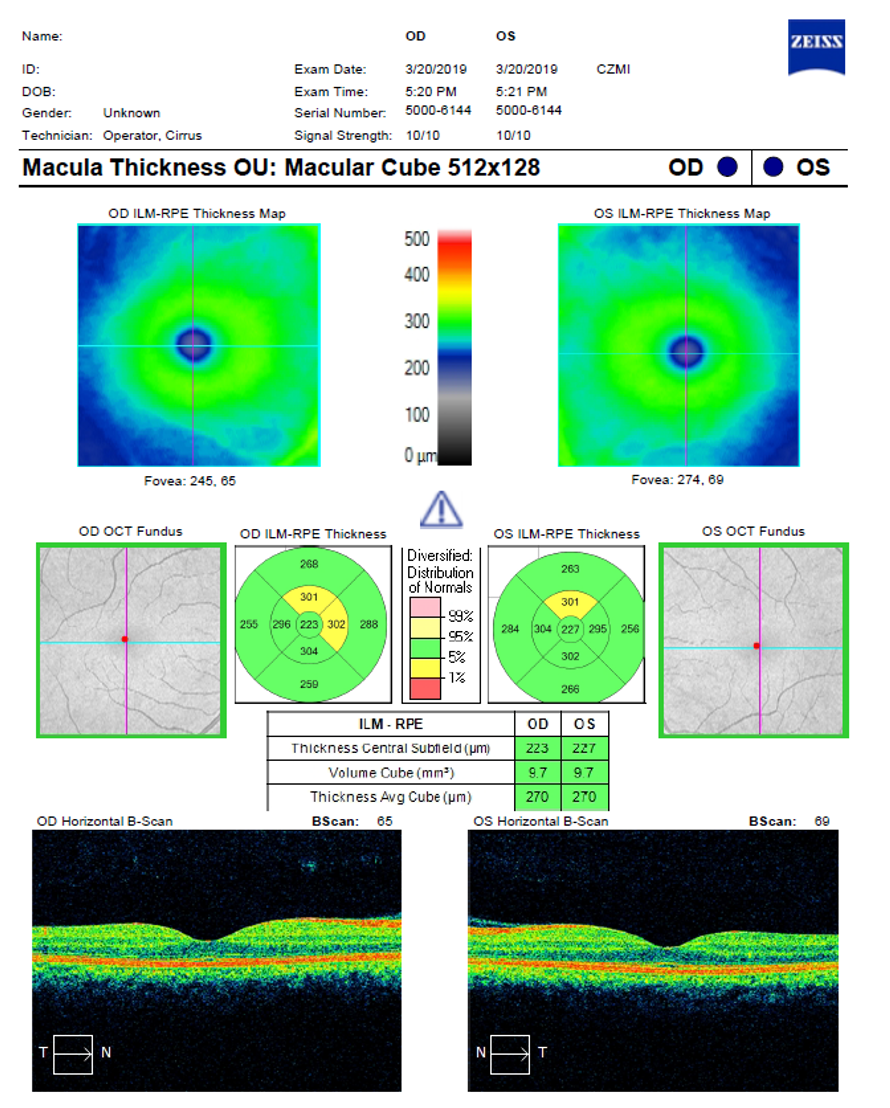
Figure 4: In this OCT diagnostic report, the top box indicates where identifying patient information and signal strength scores are located. The second box identifies the topographical retinal thickness map for each eye. The next box highlights the quantitative or numerical thickness map for each eye. The bottom box indicates where the B-scan image for each eye can be found. This image depicts the use of a pseudo-color scale.
Vitreomacular Interface Disorders
Introducing Vitreomacular Interface Disorders
Vitreomacular interface disorders can be difficult to identify solely with fundoscopy. Though visual acuity may be a helpful indicator, it is not a reliable differentiator in these cases. Under such circumstances, OCT imaging is a valuable tool and will identify the proper diagnosis 100% of the time.

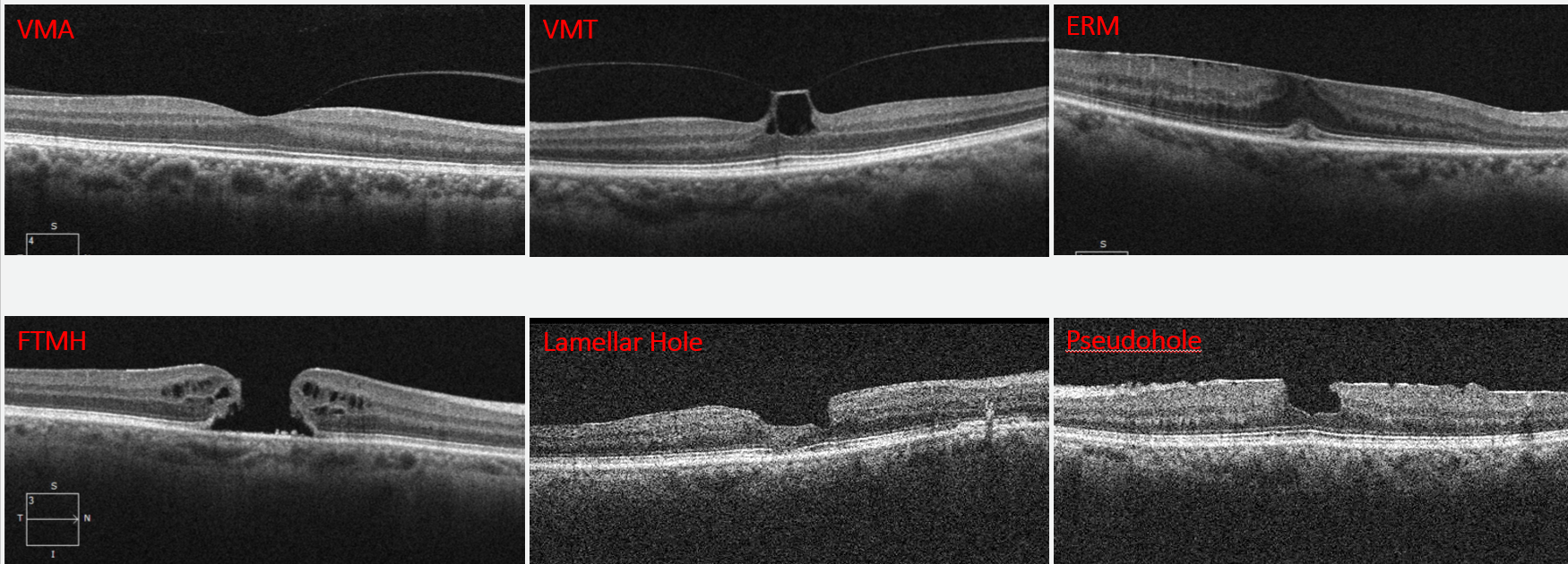
Figure 5: OCT imaging can identify specific characteristics of vitreomacular interface disorders that are crucial to differential diagnosis.
Vitreomacular Adhesion
Vitreomacular adhesion (VMA) is non-pathological. The vitreous and the retina are inherently attached, and at some point during a patient’s lifetime, the vitreous will likely pull away from the retina, leading to a posterior vitreous detachment (PVD). If the vitreous and macula are attached and there is no compromise to the macular contour during this process, this stage of PVD formation is labelled VMA and considered a benign finding.
Vitreomacular Traction
When the posterior cortical vitreous actively pulls on the retina, distorting retinal architecture, it is termed vitreomacular traction (VMT). VMT can easily be identified at the vitreoretinal interface on the B-scan. This traction can disrupt the retinal contour and cause thickening. When viewed on the retinal thickness maps, any area of central thickening will correlate with the area of traction on the B-scan.

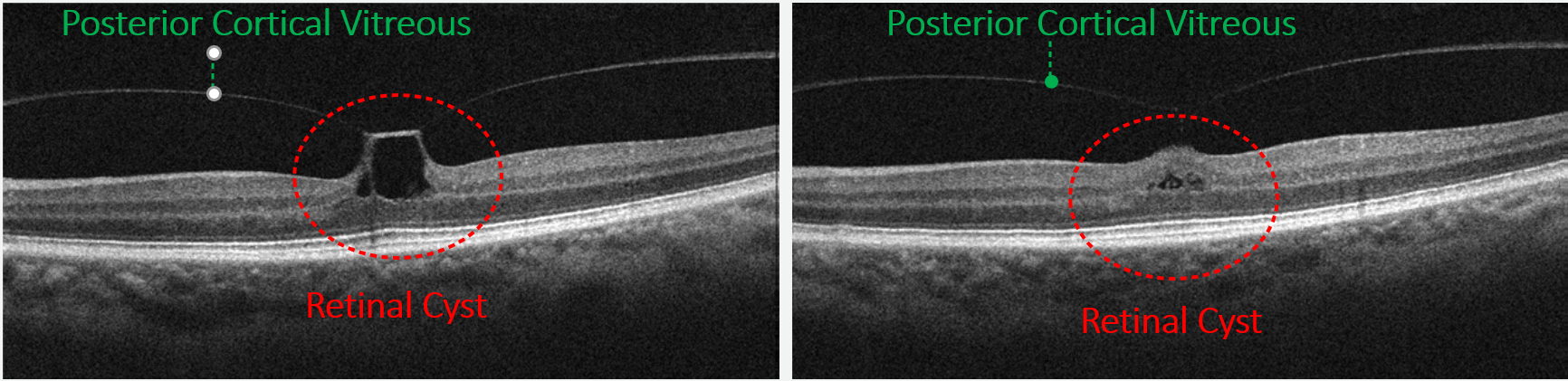
Figure 6: Here a case of VMT has been imaged with a raster scan, allowing multiple views of the entire affected area. Anterior to the RPE, retinal cysts may develop secondary to the traction. Vitreomacular traction can resolve spontaneously without intervention, and in such cases, any remaining cysts may be observed for resolution.
Epiretinal Membrane
In the case of an epiretinal membrane (ERM), the fibrous sheet at the vitreomacular interface can be identified on the scan. This membrane may cause no traction, and therefore no impact on visual acuity. In these cases the ERM may be monitored. As progression occurs, some thickening may be seen on both the B-scan and the retinal map. OCT imaging can be helpful to diagnose the severity of the ERM and the Macular Change Analysis can be used to guide management.

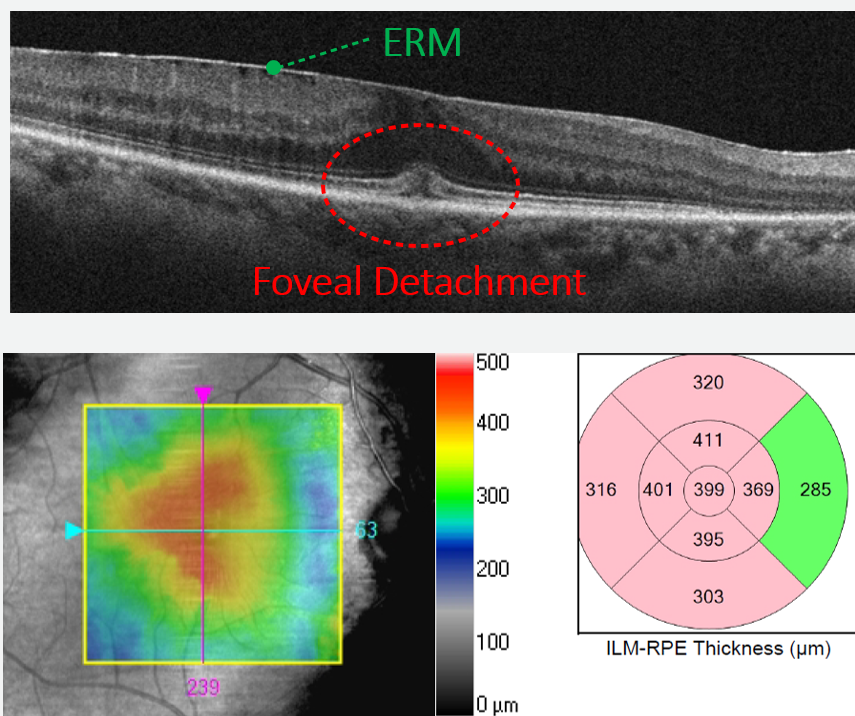
Figure 7: The traction of this progressed ERM has caused the fovea to begin to detach. Thickening may be seen on both the retinal map and the B-scan image.

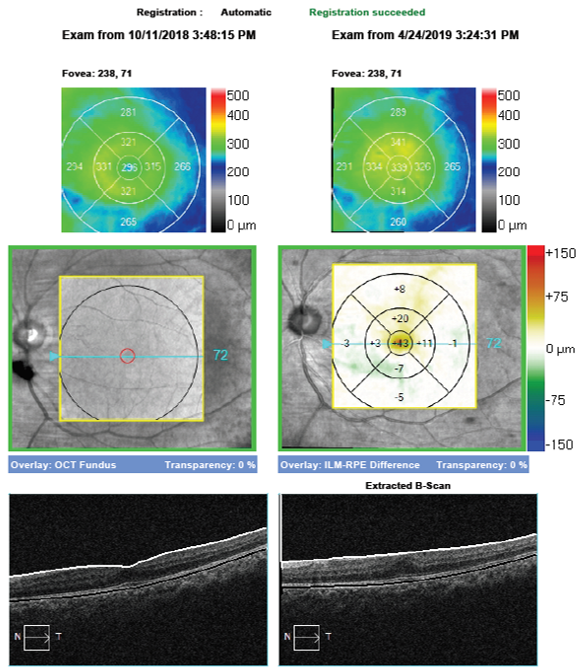
Figure 8: The Zeiss Cirrus OCT is capable of providing a progression or change analysis map to highlight changes in the OCT over time. Central thickening can be seen where the ERM is growing and causing increased traction on the retina. In such cases, retinal consult and surgical intervention may be warranted to minimize vision loss. If a progression map is available, it is important to ensure the scans are registered, meaning they can be accurately compared from point to point. This allows easy detection of increased or decreased retinal thickening, which can help guide management decisions.
Pseudohole and Lamellar Hole
A pseudohole occurs when contraction of an ERM changes the foveal contour, distorting the macula into an excavated configuration, but results in no tissue loss or visual acuity compromise. A lamellar hole is characterized by an irregular foveal contour with a break in the inner retina. The tissue loss is limited to the inner retina, while the outer retinal layers remain relatively unaffected.
Full Thickness Macular Hole
A case of vitreomacular traction or epiretinal membrane may progress to a full thickness macular hole (FTMH). The patient may develop tissue loss foveally, identified as central thinning on the OCT maps. Retinal cysts may remain within the area of retina affected by traction, causing perifoveal thickening that can be pinpointed on the macular thickness maps as well as the B-scan.

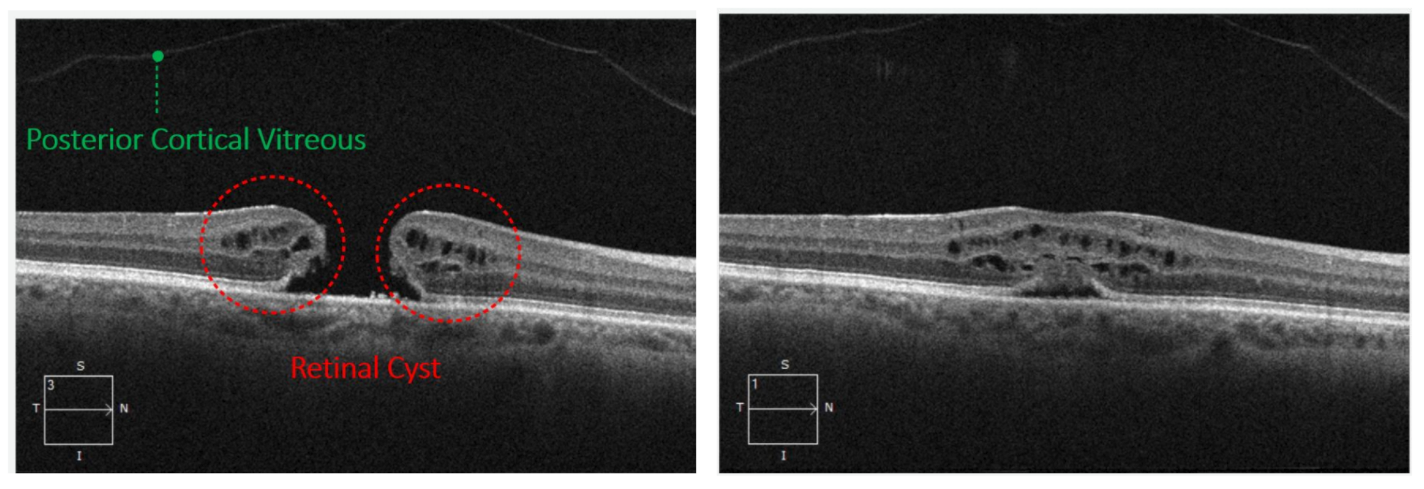
Figure 9: Raster and radial scans provide multiple B-scans allowing a high resolution view of the pathology from several different angles. In this raster scan, a full thickness macular hole can be seen. The view on the left is through the foveal center, while the view on the right is off axis. If only the off axis view is evaluated, the patient appears to have solely macular edema. However when viewed in tandem, it becomes apparent this patient has a full thickness macular hole and the off axis scans are simply the peripheral portion of that macular hole. In the image to the left, a full thickness macular hole is associated with perifoveal cysts. The posterior cortical vitreous has completely pulled away, releasing the traction and indicating the presence of a PVD.
Masquerader
Solar retinopathy can masquerade as a macular hole because it causes central cavitation of the macula. However, the retinopathy is simply a loss of outer retinal tissue. The inner retinal tissue remains unaffected and there is no traction causing the cavitation, as in macular holes. These differences can be seen on B-scan imaging.

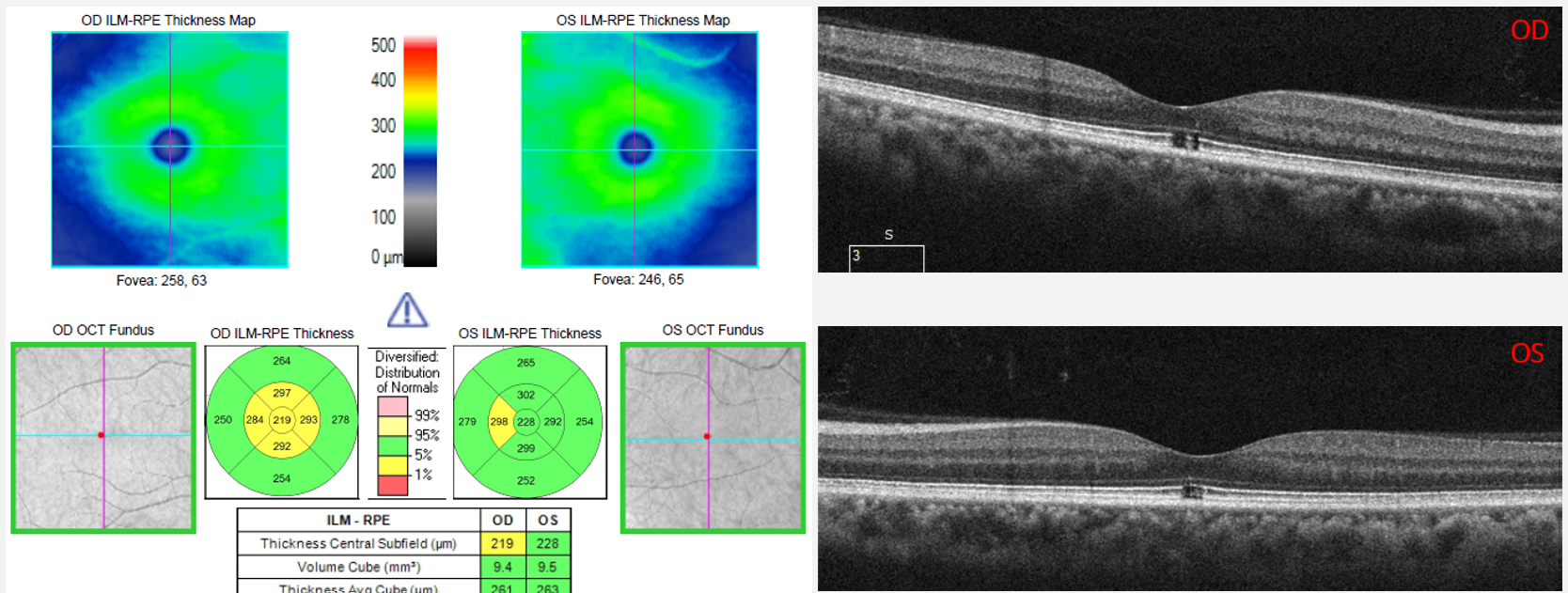
Figure 10: This case highlights the importance of always reviewing the B-scans in relation to the macular thickness maps on the diagnostic report. The B-scan image clearly shows outer retinal loss without traction.
Differential Diagnosis of Lesions
Introducing Differential Diagnosis of Light Colored Retinal Lesions
Differential diagnosis of yellow or white lesions can be especially difficult on fundoscopy, especially if the patient has media opacities or poor fixation. However, OCT imaging can provide lesion location and characteristics that help identify the correct pathology.

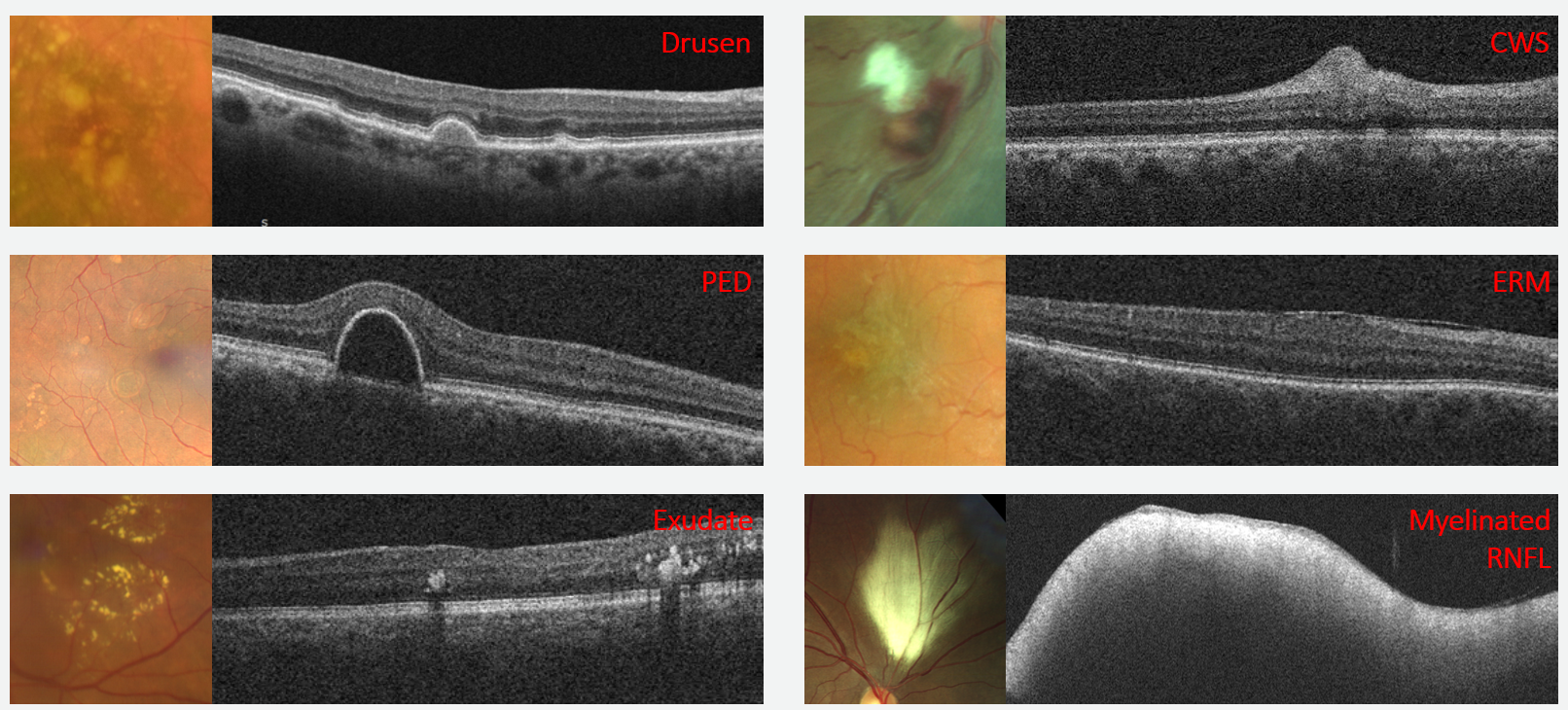
Figure 11: Note the similarities in lesion appearance on the fundoscopic view to the left, and B-scan characteristics that easily differentiate the pathology on OCT imaging to the right.
Drusen
Drusen are located in the outer retina under the RPE and push the RPE anteriorly. The drusen are hyperreflective due to lipids and other byroducts, and can be seen as a grey area under the bright RPE.
Pigment Epithelial Detachment
A pigment epithelial detachment (PED) may look very similar to a druse. PEDs are also located in the outer retina under the RPE, and push the RPE anteriorly. However the PED is hyporeflective due to the underlying serous fluid, and can be seen as a black area under the bright RPE. This difference in reflectivity makes it easy to differentiate between drusen and PED.
Exudates
Exudates are usually located in the middle retina, above the RPE and near the outer plexiform layer. They are extremely hyperreflective, to the extent that the OCT signal cannot penetrate the lesion. This shadowing of structures posterior to the lesion is characteristic of exudates.
Cotton Wool Spot
Cotton wool spots (CWS) are located within the retinal nerve fiber layer, and therefore appear very anterior on the OCT. It is important to remember, these hyperreflective elevations can be seen within the RNFL (not above or below it) and this can help differentiate them from other pathologies.
Masqueraders
An ERM may appear as an area of whitening that can be confused with a CWS on fundoscopy. However, on OCT the ERM is visible as a fibrous layer on top of the RNFL, helping to differentiate it from a CWS.
While some areas of myelinated RNFL are large and isolated, making them easy to identify, others can masquerade as cotton wool spots on fundoscopy. However, with OCT the myelination becomes obvious. Myelination is very hyperreflective, so much so that no light penetrates the myelination, causing complete shadowing with no view of any structures posterior to it. In contrast, all retinal layers posterior to the RNFL are still visible on OCT in the presence of a CWS.
Differential Diagnosis Of Pigmented Retinal Lesions
Introducing Differential Diagnosis Of Pigmented Retinal Lesions
Like light colored lesions, pigmented lesions of the retina can be difficult to differentiate by appearance alone. The use of OCT aids in identification of the involved retinal layers, allowing the clinician to correctly diagnose the lesion.

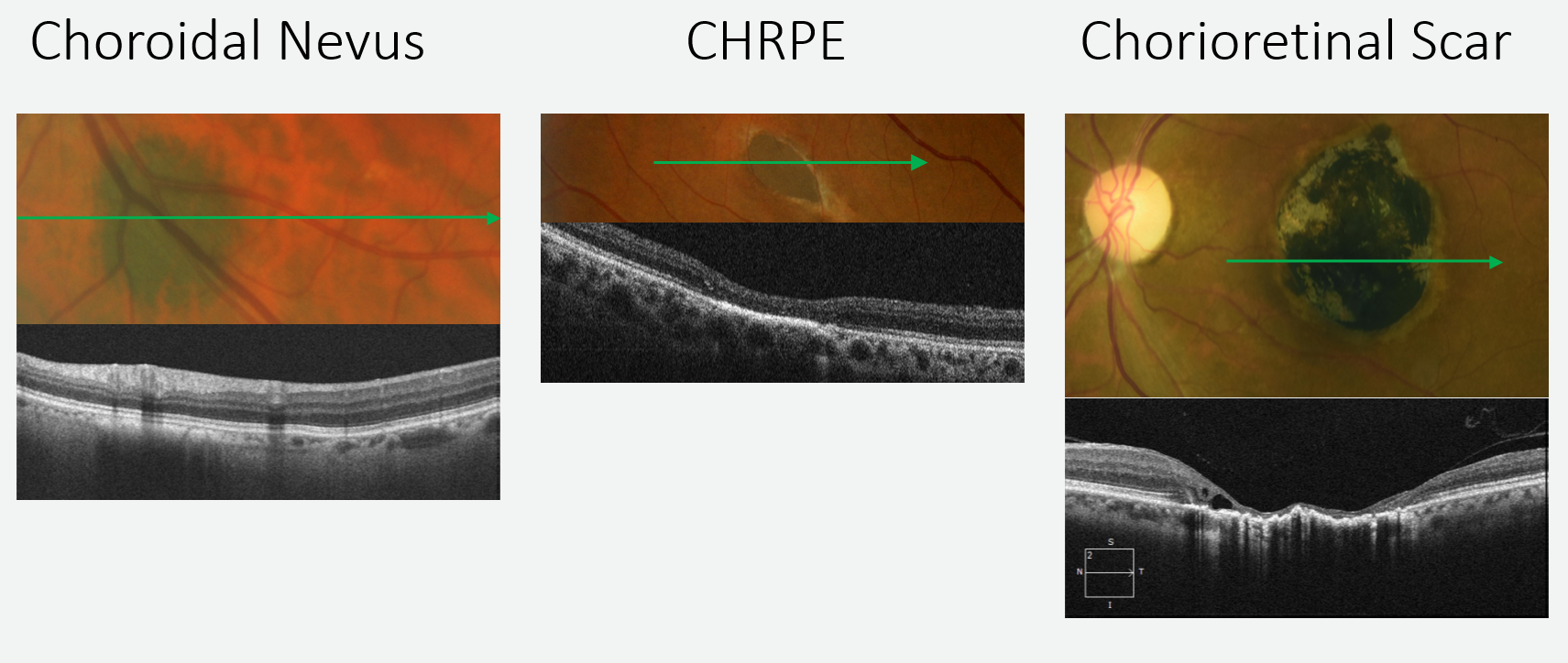
Figure 12: On the left, choroidal thinning can be seen anterior to a flat nevus, both of which are posterior to the RPE. The middle image shows outer retinal thinning with an underlying thickened RPE, representing a CHRPE. In the image on the right, a chorioretinal scar has caused significant inner and outer retinal atrophy and a distorted RPE.
Choroidal Nevus
Choroidal nevi are a common retinal finding. These highly pigmented lesions are located posterior to the RPE, and are typically flat or minimally elevated. The dense pigment of the nevus absorbs the light wave signal, causing shadowing which impedes the view of the choroid posterior to the nevus. Overlying choroidal thinning is evident in many cases.
Congenital Hypertrophy of the RPE
Congenital hypertrophy of the RPE (CHRPE) represents enlarged or hypertrophic RPE cells that contain increased pigment, causing a very dark appearance on fundoscopy. The RPE of a CHRPE is nonfunctional, preventing nourishment of the outer retina and leading to outer retinal atrophy with collapse of the overlying inner retina. With OCT imaging, the RPE appears thickened, with overlying outer retinal thinning.
Chorioretinal Scar
Chorioretinal scars can occur due to inflammation, causing pigment migration and RPE hyperplasia. The irregular area of RPE hyperplasia is associated with severe thinning of the overlying retina. Retinal cysts can form as the atrophied retina collapses onto the RPE.
Macula Edema
Introducing Macular Edema
Macular edema is a nonspecific term for any fluid within the macula. The OCT diagnostic report can show pockets of thickening on the retinal thickness map, which correlate with thickening on the quantitative map. However, different types of edema cannot be distinguished simply by viewing these maps. It is important to evaluate the areas of fluid on the B-scan for distinguishing properties.
Diabetic Macular Edema
Diabetic macular edema (DME) is a consequence of increased vascular permeability associated with diabetic retinopathy. The OCT diagnostic report will reveal pockets of thickening on the retinal thickness and quantitative maps, while areas of fluid filled cysts appear on the B-scan. The areas of edema are often irregular and may not be centered on the fovea. Exudates may be present as well.

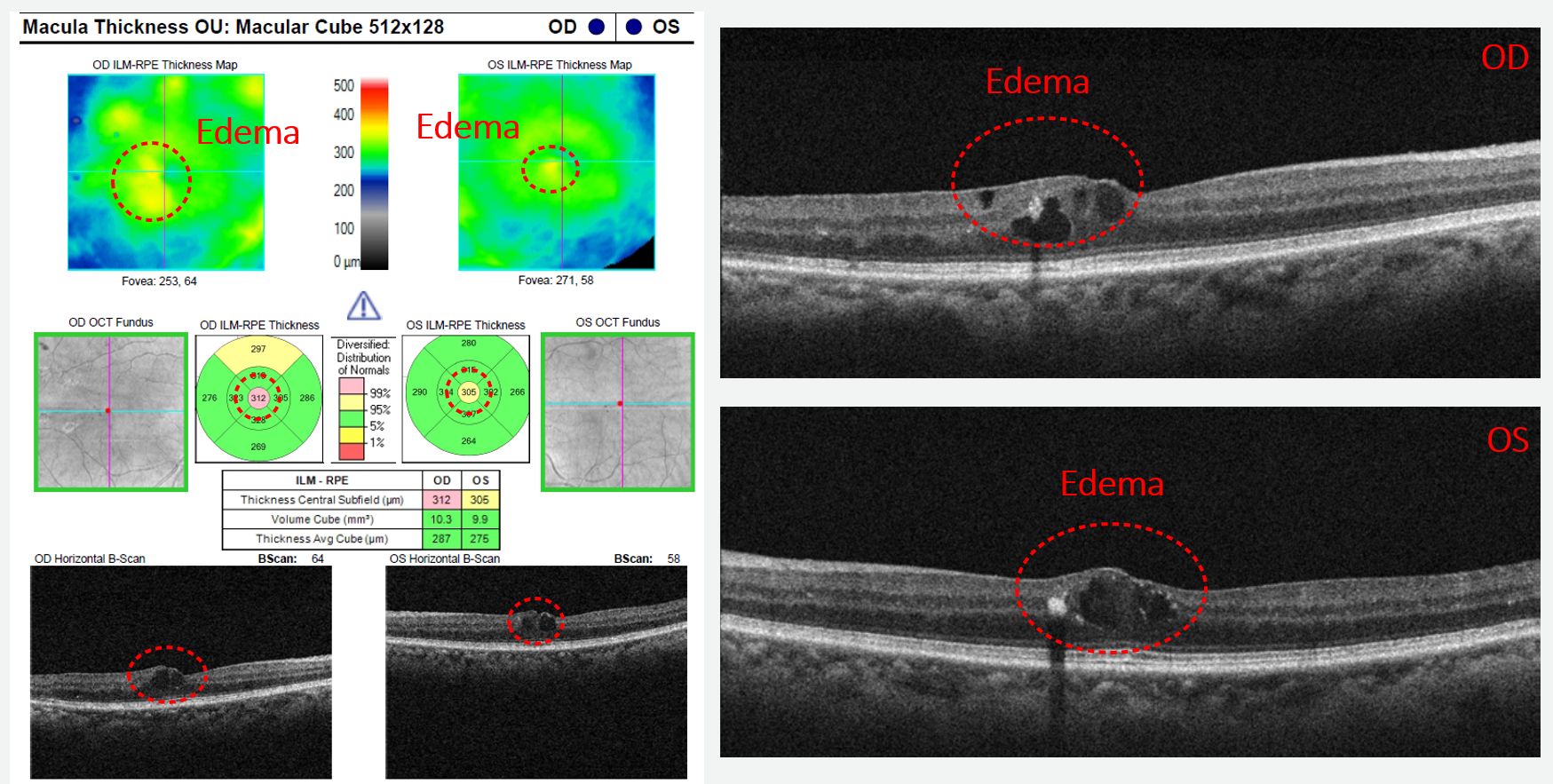
Figure 13: Areas of irregular edema are circled on the thickness map, the quantitative map, and the B-scan. Note that the location of the edema is correlated in each component of the report.
Pseudophakic Cystoid Macular Edema
Cystoid macular edema (CME) is characterized by petaloid shaped cysts that can help distinguish it from other types of macular edema. These cysts are best viewed on the B-scan. Pseudophakic CME occurs in patients who have had cataract surgery.

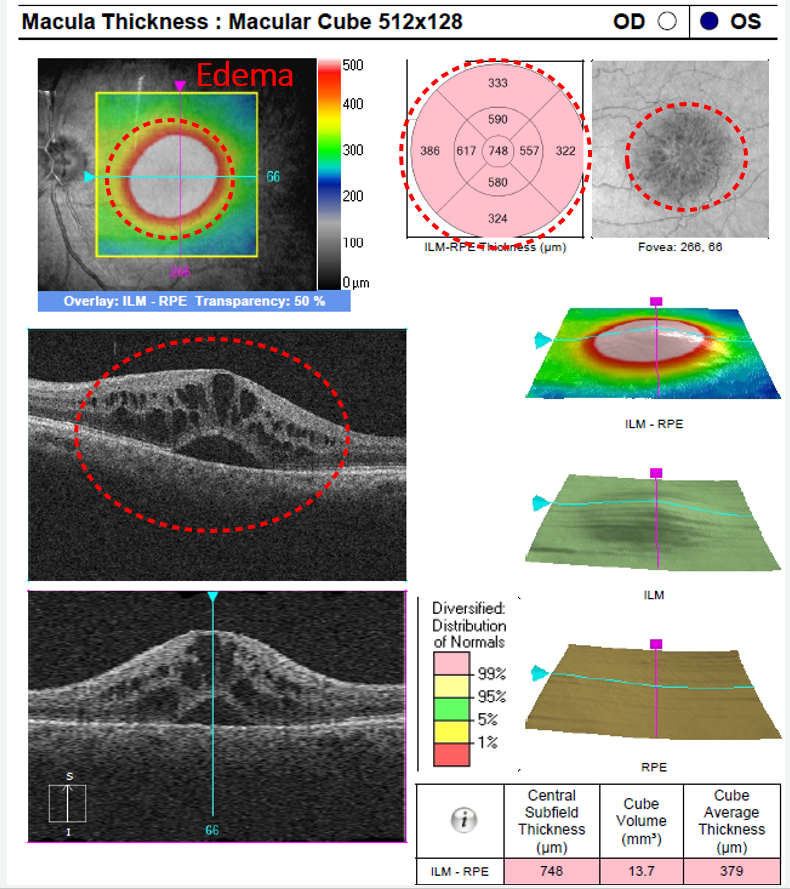
Figure 14: The pataloid shape of cystoid macular edema is well illustrated in the enface image.
Branch Retinal Vein Occlusion
Edema secondary to branch retinal vein occlusion (BRVO) can resemble DME in that it is irregular and asymmetric. However, the location of the edema can help establish the cause, as the edema will present near an occlusion or area of vascular remodeling.

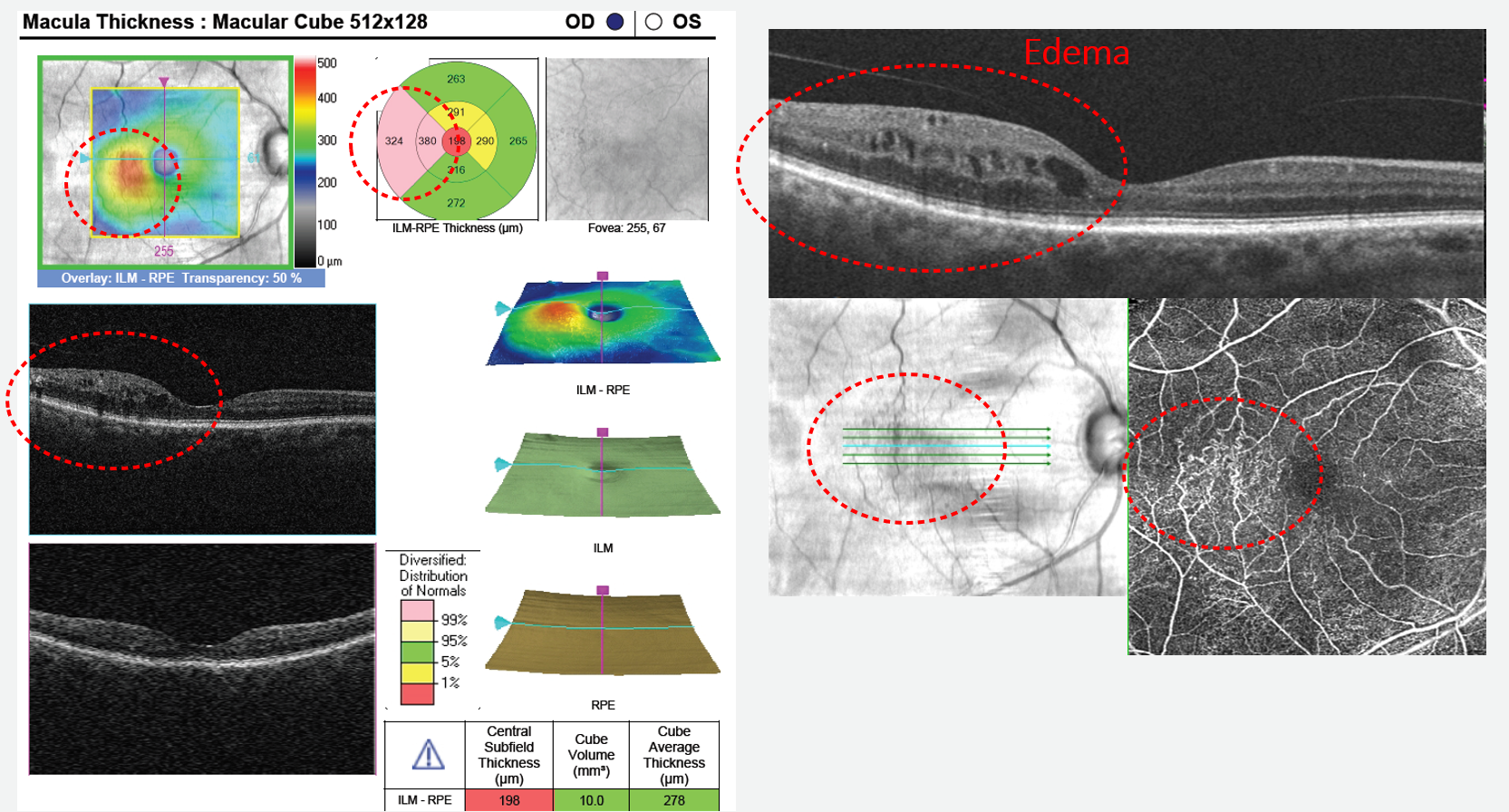
Figure 15: The edema is isolated to an area of vascular remodeling.
Choroidal Neovascularization
On fundoscopy, a mild case of choroidal neovascularization (CNV) may present with blunting of the foveal reflex, but can be subtle and easily missed. On OCT, the fluid accumulation is readily apparent. The edema is associated with a hyperreflective neovascular net composed of the growing blood vessels and fibrous tissue. There may be associated exudates, or even a hemorrhagic PED.

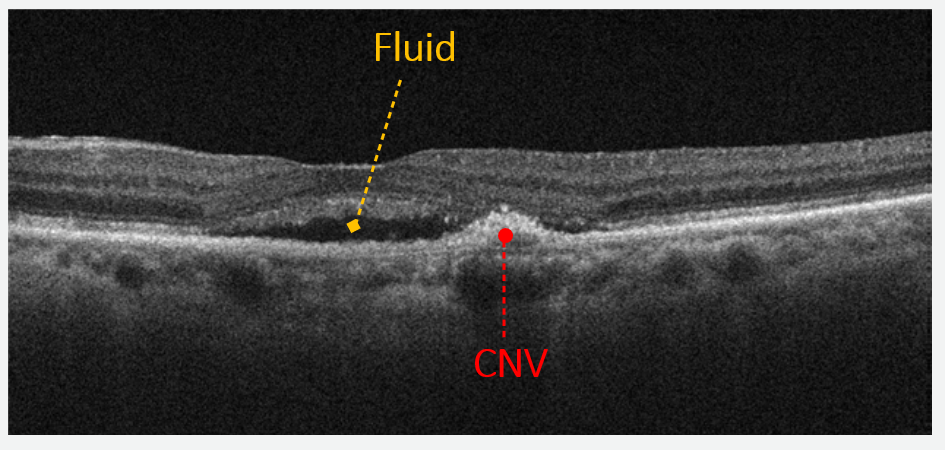
Figure 16: A small neovascular net can be seen with adjacent retinal edema.
Central Serous Chorioretinopathy
Central serous chorioretinopathy (CSC) can be difficult to detect and differentiate solely with fundoscopy. On OCT, subretinal fluid can be seen on the retinal maps as well as the B-scan. A non-hemorrhagic PED may be apparent on the B-scan as well. CSC is typically managed by observation, for which the use of OCT progression maps are crucial, as worsening of the edema indicates a need for retinal consult.

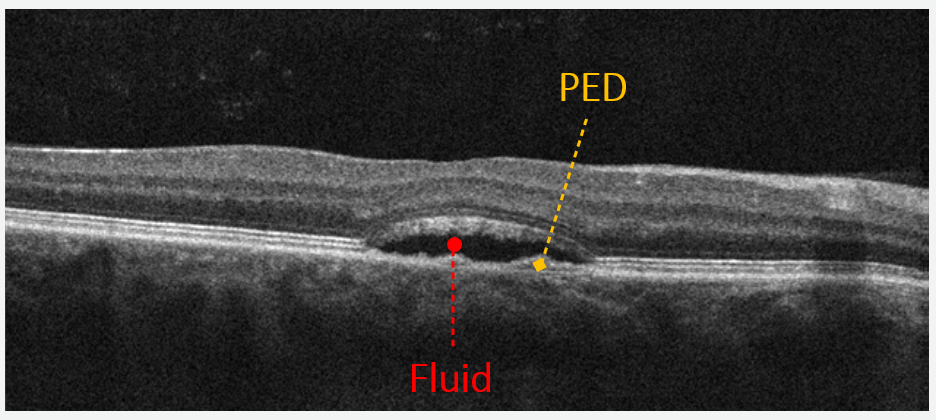
Figure 17: A serous detachment of the macula is accompanied by a PED in the presence of central serous chorioretinopathy.
Macular Edema Masqueraders
On fundoscopy, both macular telangiectasia and choroidal folds can appear similar to retinal edema, but emerge as distinct entities on OCT imaging.
Macular telangiectasia type 2 (MacTel) may present with dot hemorrhages temporal to the fovea, prompting further evaluation by OCT. Small retinal cysts that appear similar to early retinal edema may be present on the B-scan, but the retinal thickness map does not demonstrate the expected thickening typically associated with edema. Instead the area shows atrophy or thinning, and it is this thinning that defines the pathology.

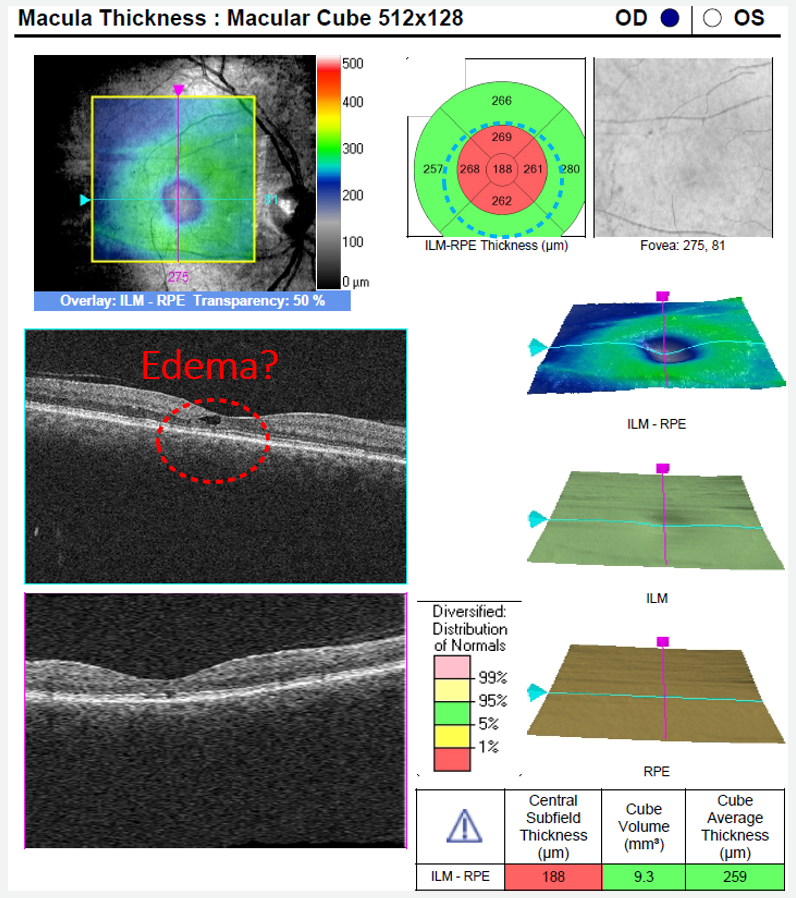
Figure 18: Note the central retinal thinning on the topographic and thickness maps of this macular cube OCT. This thinning is due to atrophy of the retina, indicating MacTel.
Though rarely occurring, choroidal folds can resemble macular edema. On fundoscopy, dark bands present across the fundus and may appear thickened. Most choroidal folds are horizontally oriented and may not appear on the standard horizontal OCT scan; some irregularity of the RPE may be seen but no obvious folds or retinal edema will be present. However, when a vertical scan is performed through the folds, outer retinal and choroidal disruptions can be visualized and the RPE appears undulated. Choroidal folds are often idiopathic, especially if they present symmetrically between the eyes. Still it is important to rule out scleritis or retrobulbar mass.

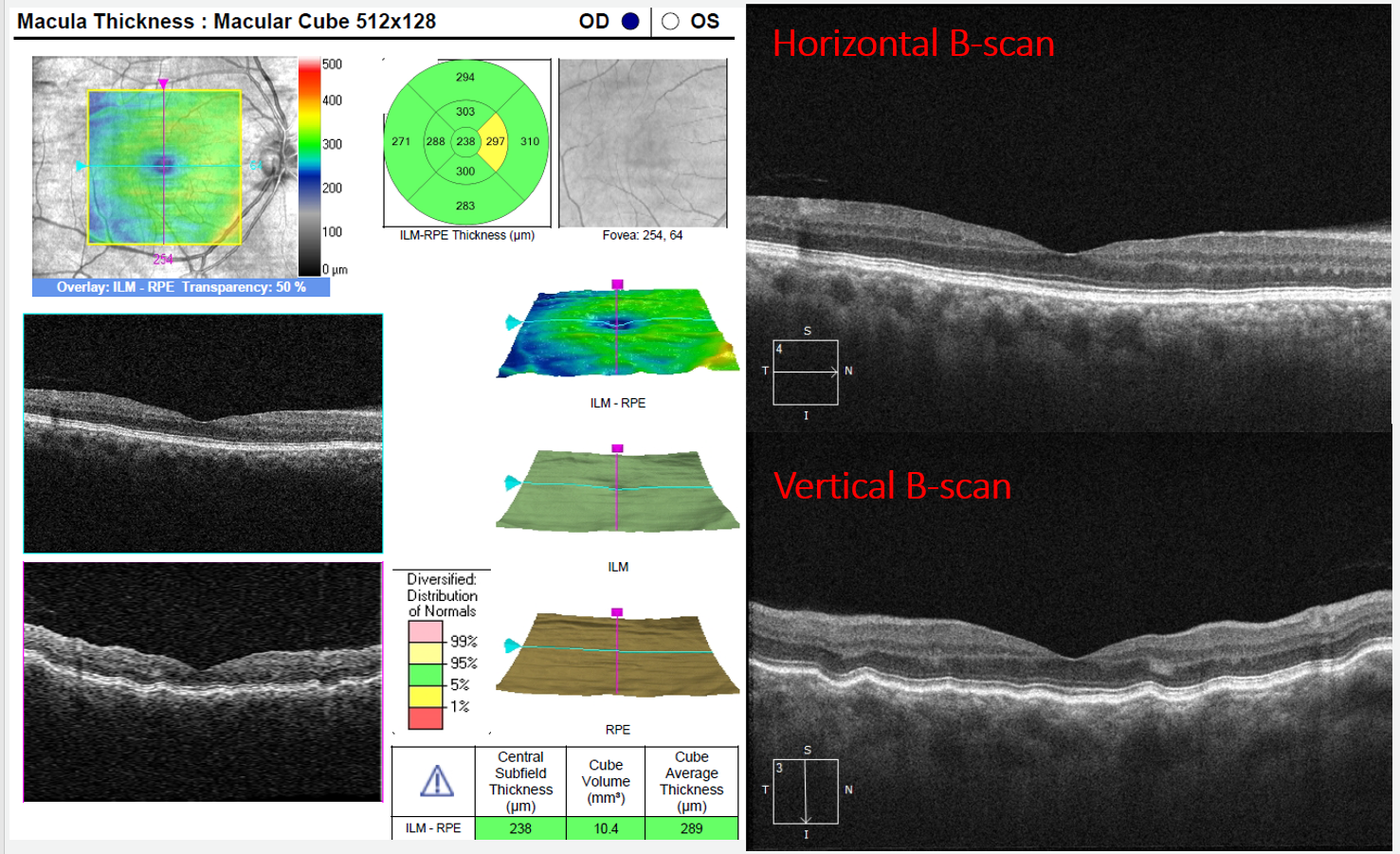
Figure 19: In this case of choroidal folds, minimal RPE disruption is seen on the horizontal scan while the vertical scan makes the choroidal and retinal effects apparent.
Age-related macular degeneration (AMD) can present with a combination of the pathologies listed above. Both light colored and pigmented lesions can be present, and in cases of CNV, macular edema and exudates may also be seen.
Drusen
There are several types of drusen, each with a distinct appearance on OCT and a distinct risk associated with AMD progression. Therefore differentiation of the drusen type is important to AMD management. Cuticular or hard drusen is characterized by an intact RPE overlying a single druse with Bruch’s membrane at its base. There is characteristic thinning of the RPE at the apex of the druse. Soft drusen tends to be larger and fluffy in appearance. The overlying RPE remains consistent in thickness over the entirety of the druse. Again, Bruch’s membrane sits at the base. Subretinal drusenoid deposits look similar to hard drusen, however the RPE does not overlie the lesion, but instead lies posterior to the lesion.

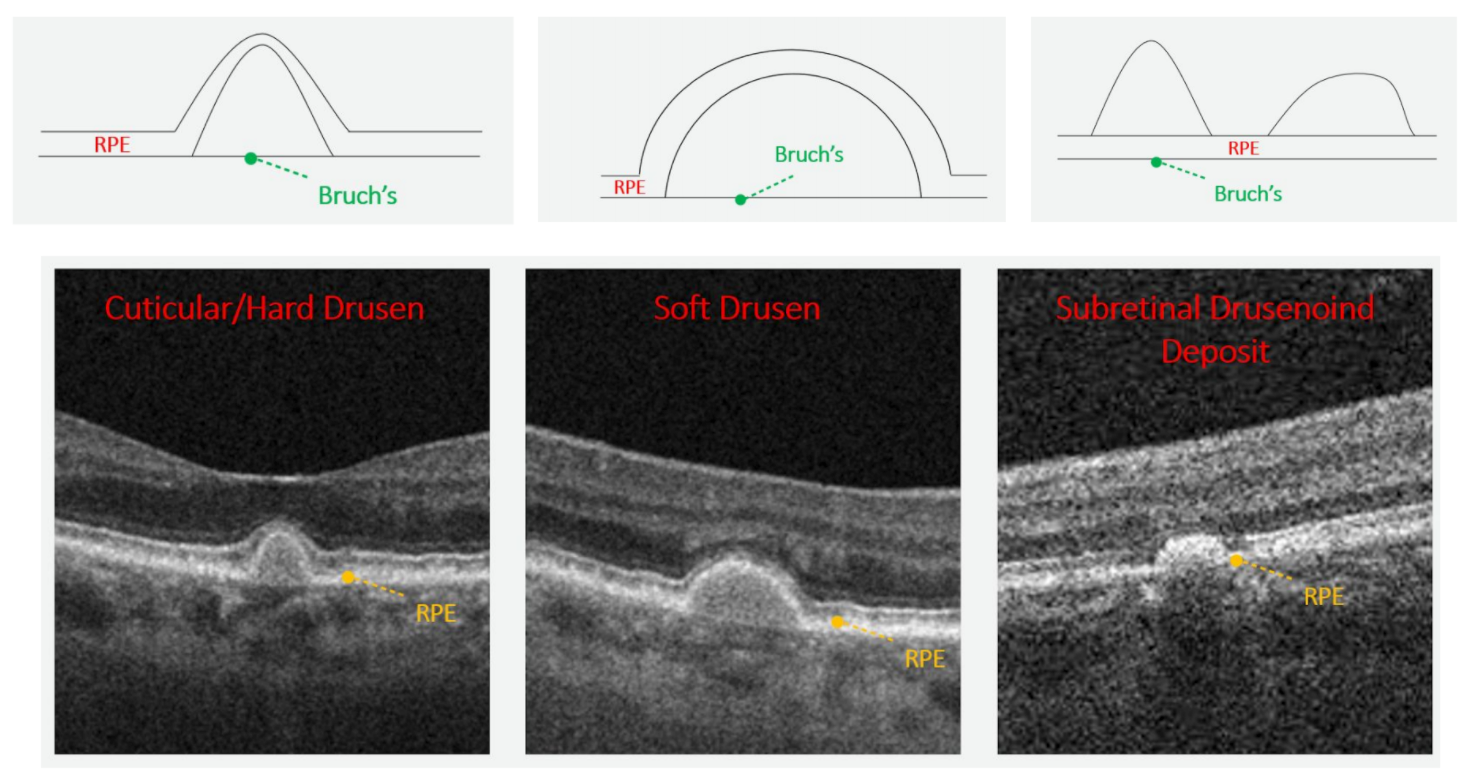
Figure 20: Note the distinct appearance between each drusen type when imaged with OCT.
Geographic Atrophy
Geographic atrophy (GA) is associated with the appearance of retinal thinning on OCT. This stage of AMD is characterized by loss of the RPE and degeneration of the outer retina, which leads to collapse of the inner retina.

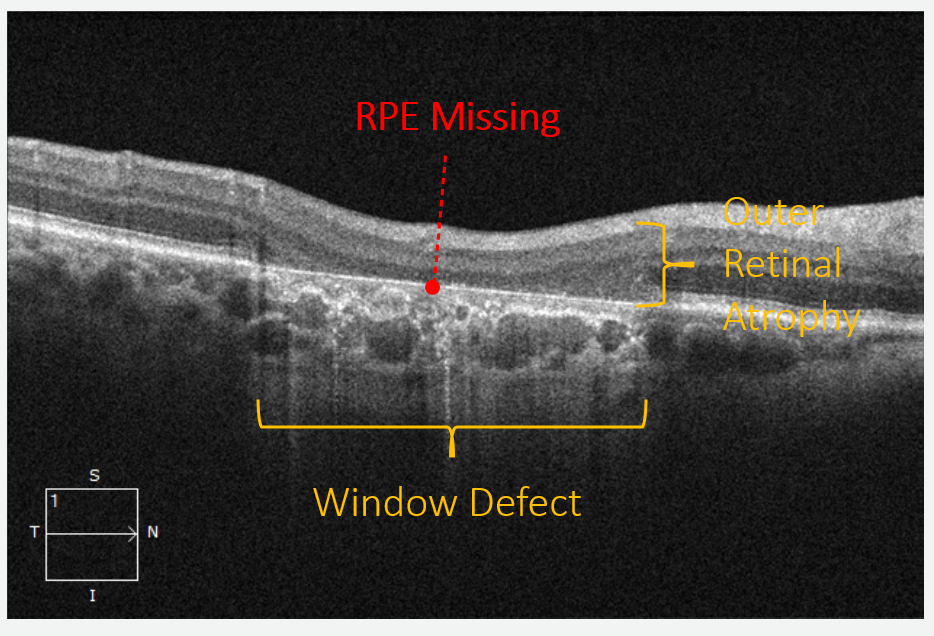
Figure 21: In this view of geographic atrophy, note the window defect and increased visibility of choroidal detail due to the missing reflective signal of the RPE.
Choroidal Neovascularization
As discussed above, choroidal neovascularization is characterized by a hyperreflective neovascular net and a collection of fluid and exudates.
Masquerader
Adult Onset Foveomacular Vitelliform Dystrophy can mimic the appearance of AMD. The associated lesions are foveal and tend to be very symmetric between the two eyes. They appear round and yellow in color on fundoscopy, and on OCT they are isolated to the level of the RPE and photoreceptors. Because this dystrophy shows minimal progression in adults, it is important to differentiate this disease entity from AMD to ensure unnecessary management protocols, such as AREDS2 therapy, are not enacted.

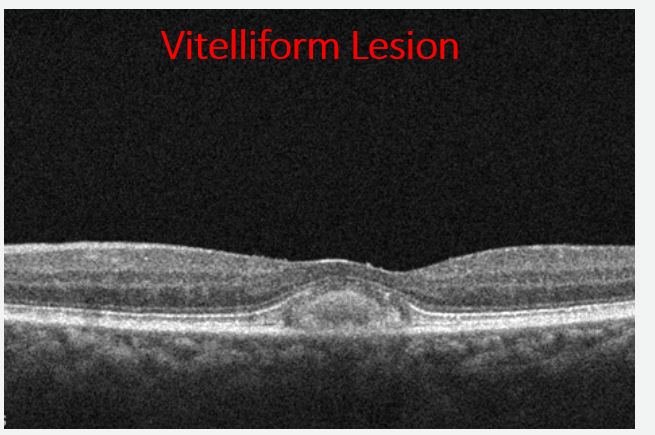
Figure 22: Note the distinct appearance of the vitelliform lesion. Compare it to the drusen above.
Pachychoroid Pigment Epitheliopathy is a pachychoroid spectrum disorder. These are macular disorders that display related choroidal pathologies, including choroidal thickening and RPE abnormalities. The macular changes can resemble the drusen and pigment changes present in AMD, however patients with pachychoiroid spectrum disease tend to be younger than AMD patients. . Thickening of the choroid occurs secondary to dilated choroidal vessels, called pachyvessels, and thinning of the choriocapillaris overlying these pachyvessels can be seen on OCT.

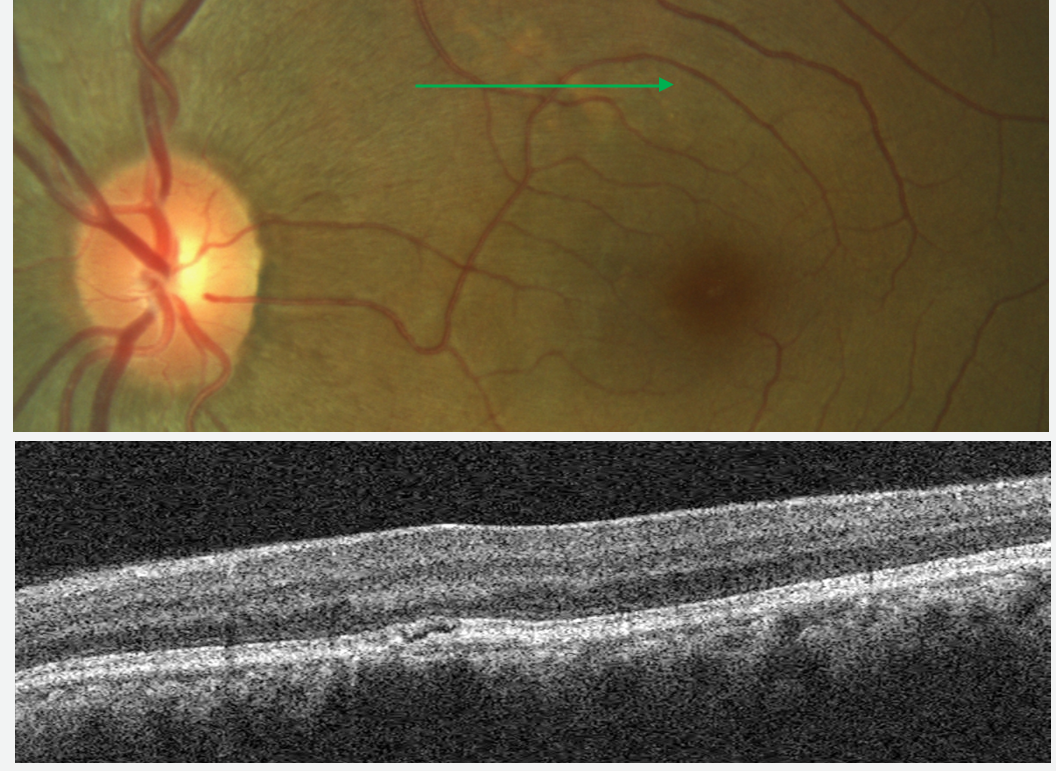
Figure 23: Pachychoroid Pigment Epitheliopathy: The fundus photo shows a light-colored lesion that may be confused for drusen in AMD, while the B-scan image resembles the appearance of retinal edema.
Conclusion
Conclusion
Optical coherence tomography (OCT) has become indispensable for eyecare providers practicing in the medical model. Whether it is used to detect central serous chorioretinopathy, to accurately identify vitreomacular interface disorders, or to assist in the diagnosis of the many diseases and conditions treated by ODs, OCT is one of the many key tools in the ECP’s armamentarium.
