




Myelination of the retinal nerve fiber layer (RNFL) occurs in about 0.57 to 0.98% of the population.1,2 Fundoscopic exam demonstrates gray or white patches in the distribution of retinal nerves, a finding that is most often unilateral.3
The pathogenesis of myelinated RNFL occurs when myelination of the optic nerve continues beyond the lamina cribosa, which is commonly thought to be a physical barrier to the anterior migration of myelin-producing oligodendrocytes.1,3,4 Faulty lamina cribosa and subsequent myelination of RNFL can be due to embryologic abnormalities or acquired insult.3
Myelinated RNFL are most often found incidentally; however, it can be associated with a broad spectrum of ocular and systemic abnormalities, such as retinal vessel abnormalities, craniofacial abnormalities, Gorlin-Goltz syndrome (basal cell nevus syndrome), and neurofibromatosis type 1.3,5
Of particular note is the triad of findings: myelinated RNFL, myopia, and amblyopia, which is often severe and treatment-resistant.5 Aggressive amblyopia treatment should be pursued.
Amblyopia treatment for myelination
The mainstay of amblyopia treatment is a combination of refractive correction when needed and physical or pharmacologic occlusion of the non-amblyogenic eye.
In recent years, dichoptic therapy has been introduced as a promising addition to the arsenal of amblyopia treatment. The basis of dichoptic therapy is fundamentally different from monocular penalization and focuses on the binocular rebalance of visual stimulation.
Recent studies on dichoptic therapy for amblyopia
Dichoptic therapy studies have shown that prolonged contrast reduction of the sound (non-amblyopic) eye during binocular vision reduces interocular suppression of the amblyopic eye at the visual cortex.6 With the contrast reduction of the sound eye, both eyes are required to rebalance visual stimulation and strengthen amblyopic vision.
A preliminary investigation into the use of dichoptic gameplay was promising.7 Dichoptic therapy was then studied in larger clinical trials conducted by the Pediatric Eye Disease Investigator Group (PEDIG), involving an iPad game, Dig Rush, and contrast reduction glasses. However, the studies failed to demonstrate efficacy, likely due to low interest and poor adherence.8,9
But more recently, two dichoptic therapies implementing contrast reduction during passive consumption of video content did show promise. Luminiopia utilizes a virtual reality headset with programmed contrast reduction and contains a library of movies and TV shows.10 Curesight uses contrast-reducing glasses that incorporate eye-tracking technology to selectively blur the fovea of the sound eye to pair with a digital screen.11 Both devices were recently FDA-approved to treat amblyopia.
Case report: Myelinated RNFL, myopia, and amblyopia
A 6-year-old male presented to the clinic for a second opinion on the treatment of his mixed mechanism amblyopia. He had a history of myelinated nerve fibers of his right eye (OD) and associated myopia.
- His best-corrected visual acuity (BCVA) was 20/70 in this eye, with no improvement with the pinhole, and 20/20 in the left eye (OS).
- The patient’s current prescription was:
- -5.50 + 1.50 x 176 (OD), +2.00 + 0.75 x 064 (OS)
- Cycloplegic refraction was -5.25 + 1.75 x 180 (OD), +4.00 + 0.75 x 065 (OS)
- Stereopsis exam revealed 400 arcseconds. Worth 4 Dot test revealed peripheral fusion.
- No strabismus was observed.
Figure 1a depicts the fundus examination of the right eye. Myelinated retinal nerve fibers are seen along the superior and inferior arcades, and the macula is spared. Figure 1b shows a normal-appearing retina of the left eye.

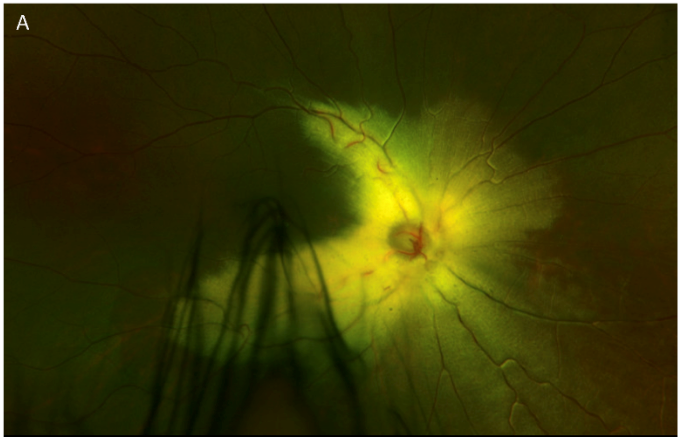
Figure 1a: Courtesy of Courtney Kraus, MD.

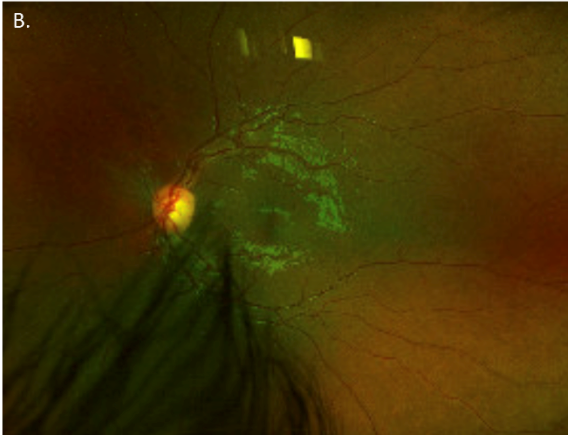
Figure 1b: Courtesy of Courtney Kraus, MD.
Optical coherence tomography (OCT) is shown in Figures 2a and 2b. The patient’s OCT is shown on the top and the normal layers of an OCT are depicted on the bottom.

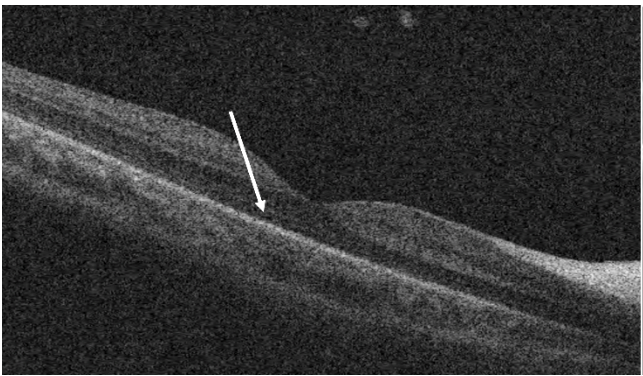
Figure 2a: Courtesy of Courtney Kraus, MD.

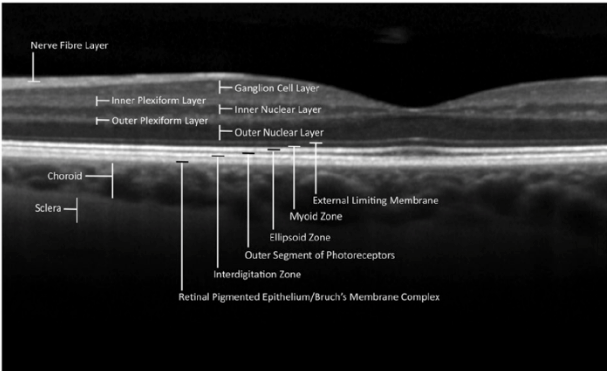
Figure 2b: Courtesy of William et al.
Patient treatment history
Regarding his amblyopia treatment history, the patient has been wearing glasses continuously since age 2 with excellent compliance. By wearing glasses alone, BCVA OD improved from 20/400 to 20/125. He had undergone a patching regimen of 2 to 4 hours per day for 2 years with intermittent compliance.
With the addition of patching, his vision improved from 20/125 to 20/100. Patching was then substituted for atropine, initially started with weekends only and titrated to four to five times per week, and the patient’s BCVA improved from 20/125 to 20/70. At this point, this patient presented to our clinic for further management. A plano lens OS was added to his atropine penalization regimen, and his BCVA improved from 20/70 to 20/60.
Luminopia, a virtual-reality-based dichoptic therapy, was initiated in addition to his 4x/week regimen of atropine and plano lens. At 3 months follow-up, BCVA OD improved from 20/60 to 20/40+. The atropine/plano lens regimen was titrated to 2 to 3x per week. The most recent follow-up visit at 5 months of dichoptic therapy, BCVA, was 20/30-2 OD.
Myelinated retinal nerve fiber and anisomyopic amblyopia
Amblyopia associated with myelinated RNFL has a worse visual prognosis than cases without myelinated RNFL.5,12,13 These associations have primarily been studied in small case series due to the rarity of their nature.
The triad of myelinated RNFL, myopia, and amblyopia, also called Straatsma syndrome, includes several associated signs, such as unilateral axial myopia and optic disc hypoplasia.12-14 Strabismus, and less commonly, hyperopia instead of myopia, may accompany myelinated RNFL.14,15
Although anisometric amblyopia is usually responsive to therapy, the anisomyopic amblyopia associated with myelinated RNFL is particularly refractory. Early researchers postulated such refractory amblyopia may be due to myelination of the macula.16,17 OCT further underscores foveal involvement, particularly at the ellipsoid zone.
The photoreceptor inner segment ellipsoid, known as the ellipsoid zone (EZ), appears on OCT as a hyper-reflective line.18 Damage to the ellipsoid zone is implicated in several retinal pathologies.18 Bass et al. reported a case series of three patients with myelinated RNFL and amblyopia in which all three patients had disrupted or absent ellipsoid zone on OCT.13
Despite the severe amblyopia associated with myelinated RNFL, aggressive amblyopia therapy should be attempted.
Treatment modalities to manage amblyopia
The first step in treatment for amblyopia is optimal refraction correction. According to the Amblyopia Treatment Study (ATS)-05 conducted by the PEDIG, anisometric amblyopia treated with refraction correction alone improved ≥2 lines in 77% of patients in patients ages 3 to 7 years old.19 One-third of patients had fully resolved amblyopia.
Our patient demonstrated several lines of improvement by wearing glasses alone, improving vision in the amblyopic right eye from 20/400 to 20/125. Though at his young age, it is reasonable to assume some of this was from test-retest improvement.
Occlusion therapy with patching
In addition to refractive correction, occlusion therapy with patching is often the next treatment addition. The ATS-05 clinical trial also evaluated the addition of 2 hours of patching the non-amblyogenic eye in children whose BCVA had plateaued after 16 weeks of refractive correction.20
Compared to the control group, which continued to wear full-time glasses only, the study found that the addition of patching modestly improved moderate to severe amblyopia.20 Regarding patching duration, patching for 6 hours/day showed greater improvement than 2 hours/day;21 however, more than 6 hours/day did not appear to show any difference in improvement.22
Despite being an inexpensive and accessible treatment option, patching can often be difficult due to poor compliance, and 2 to 6 hours of patching may not be feasible for some patients. Our patient improved from 20/125 to 20/100 over 2 years, and patching compliance was intermittent.
Pharmacologic penalization with atropine
An alternative to patching is pharmacologic penalization with atropine. The ATS-01 multicenter clinical trial randomized 419 children younger than 7 years with amblyopia to patching or eye drop atropine to non-amblyopic eye for 6 months.23 Treatment after 6 months was up to the discretion of the investigator, and the patients were followed until age 15.24
Both atropine and patching groups showed similar magnitudes of amblyopia improvement at 6 months of treatment, and visual acuity progressed with similar degrees of improvement at age 15 years of age.23,24 With substitution to atropine, our patient improved from 20/125 to 20/70.
In addition to atropine, a plano lens can be added to the sound eye for additional refractive occlusion. The clinical trial ATS-08 randomized 180 children with moderate amblyopia to the use of weekend atropine with plano lens or the use of weekend atropine alone.25 At 18 weeks, the atropine with plano group demonstrated minimal improvement compared to the atropine alone group.25 Our patient improved from 20/70 to 20/60-.
Dichoptic treatments
Luminopia
Luminopia is a virtual-reality-based amblyopia treatment incorporating dichoptic contrast reduction into a library of video content.10 Through the virtual reality (VR) headset, the image presented to the sound eye has a total contrast reduction of 15% compared to the image presented to the amblyopic eye, as represented in Figure 3.26
Figure 3 illustrates the use of Luminopia. Panel A shows the external view of the VR headset. Panel B shows the internal window of the VR. Panels C and D depict the contrast reduction and complementary dichoptic masks programmed in each eye.

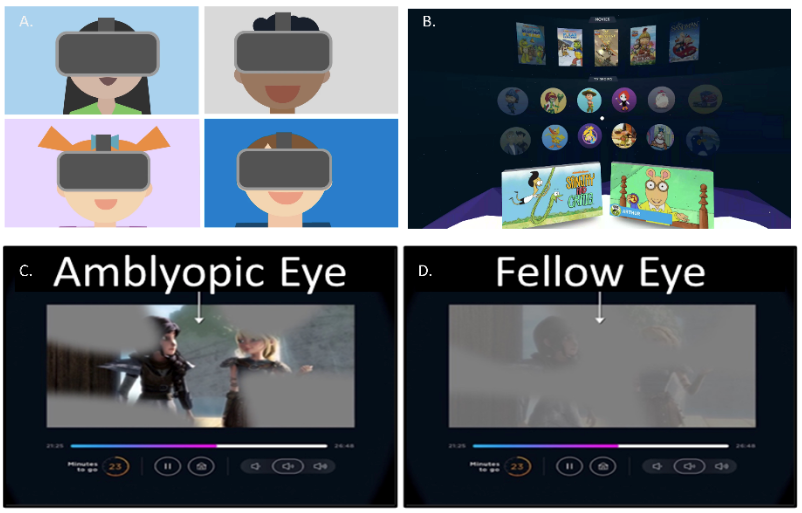
Figure 3: Courtesy of Luminopia.
In addition, complementary dichoptic masks were imposed such that binocular viewing is required to view the content fully.26 A multicenter phase 3 clinical trial randomized 105 participants aged 4 to 7 years old with amblyopia to either a treatment group, which used Luminopia for 1 hour/day, 6 days/week with full-time spectacle correction, or a control group, who wore full-time glasses.10 Of note, this study was designed similarly to the ATS study with the Dig Rush iPad game.8,9
At 12 weeks, the treatment group demonstrated visual acuity improvement of 1.8 lines compared to 0.8 lines of the control group (P = 0.0011).10 The authors noted a high adherence to the Luminopia therapy, which may be partly because VR is an immersive experience or because participants can select a variety of content that suits their interests.10
Our patient had improved from 20/60 to 20/40+, and stereoacuity improved to 140 arcsecs at the 3-month follow-up. After 5 months of Luminopia, BCVA improved to 20/30-2.
Curesight
While Luminopia compared dichoptic therapy to spectacle correction, Curesight compared its dichoptic device to patching.11 Curesight utilizes a combination of an eye-tracker and special contrast reduction glasses to allow children to passively watch video content on a paired 11.6-inch monitor (Figure 4).11
Figure 4 illustrates the Curesight monitor with a programmed eye tracker and contrast reduction glasses. In the non-amblyopic eye, the eye-tracker shifts the contrast reduction of certain images based on the patient’s focus. The amblyopic eye shows images with normal contrast.


Figure 4: Courtesy of NovaSight.
The Curesight noninferiority trial studied 103 participants 4 to 9 years of age, randomized to either a patching regimen of 2 hours/day or dichoptic therapy for 90 minutes per day for 5 days per week.11 Visual acuity was monitored at 16 weeks.11
This study demonstrated similar efficacy for visual acuity improvement between Curesight and patching and higher adherence to Curesight than patching.11 Improvement in the patching group plateaued at week 12, but the Curesight group continued to show improvement until week 16.11
Conclusion
When comparing these dichoptic therapies, both Luminopia and Curesight are FDA-approved to treat amblyopia. Dichoptic VR headsets like Luminopia are portable and immersive; however, content is limited to its library.
Special glasses allow Curesight to blur only the fovea of the non-amblyopic eye more precisely, and there is wider video content availability, but it is limited to its paired device.
Another limitation of both devices is the potential increased screen time. The American Academy of Pediatrics recommends children 2 to 5 years should be limited to no more than 1 hour/day of digital media use.27
With appropriate use, these novel dichoptic therapies are promising additions to the arsenal of amblyopia therapy. They may be particularly efficacious in the treatment of severe amblyopia such as those associated with myelinated RNFL syndrome.
