


Ocular Disease Case Study Week—created in partnership with ZEISS Professional Education —brought together eyecare professionals from around the globe to increase disease knowledge through the sharing of unique case studies, diagnostic scans, and workflow protocols.
After presenting the top four cases on the @eyesoneyecare.optometry Instagram channel in early December, followers voted on which was most compelling. Below are the cases that made these top-four finalists stand out.
First place: Madison Abbey Rhoton, OD
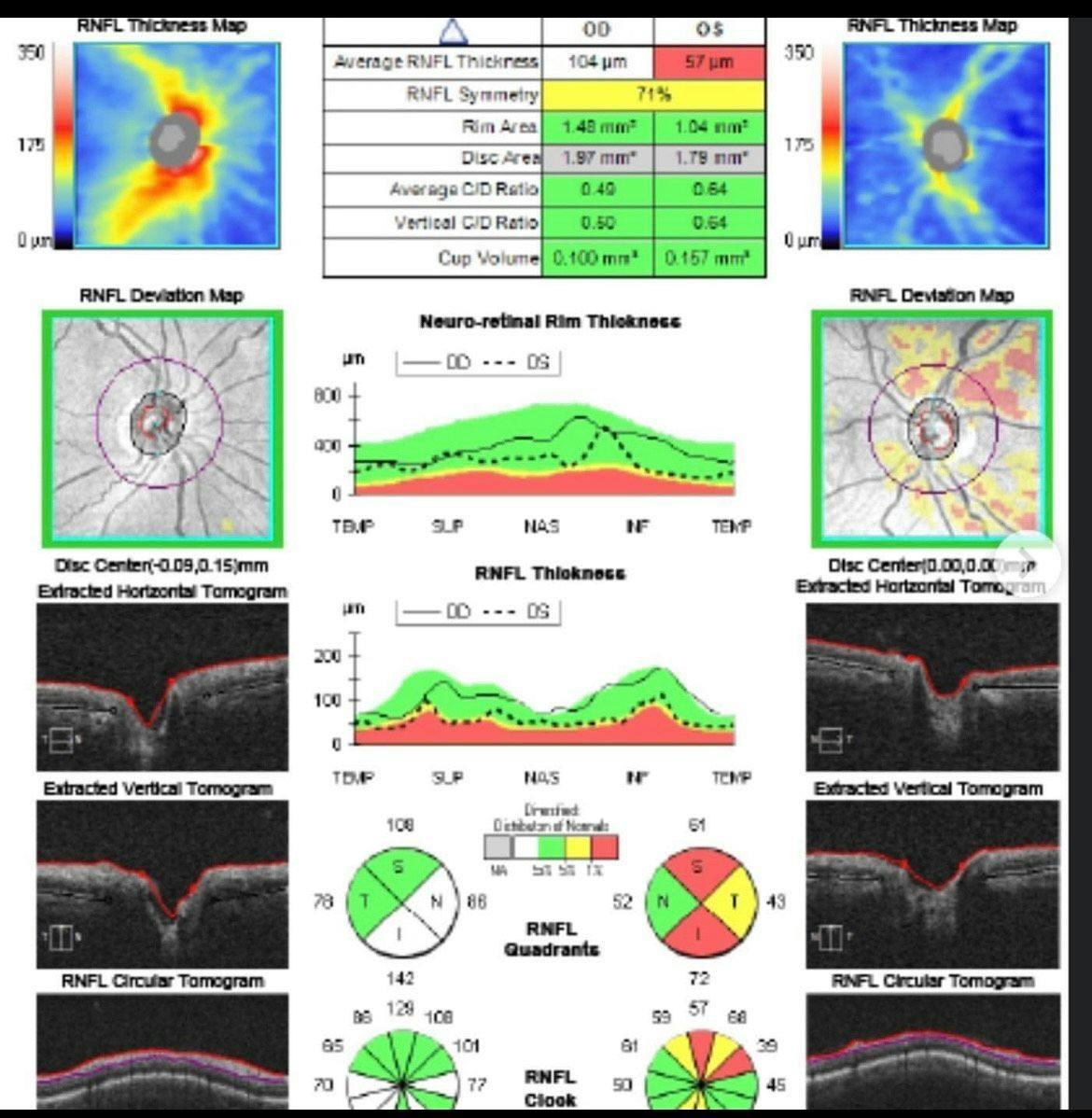
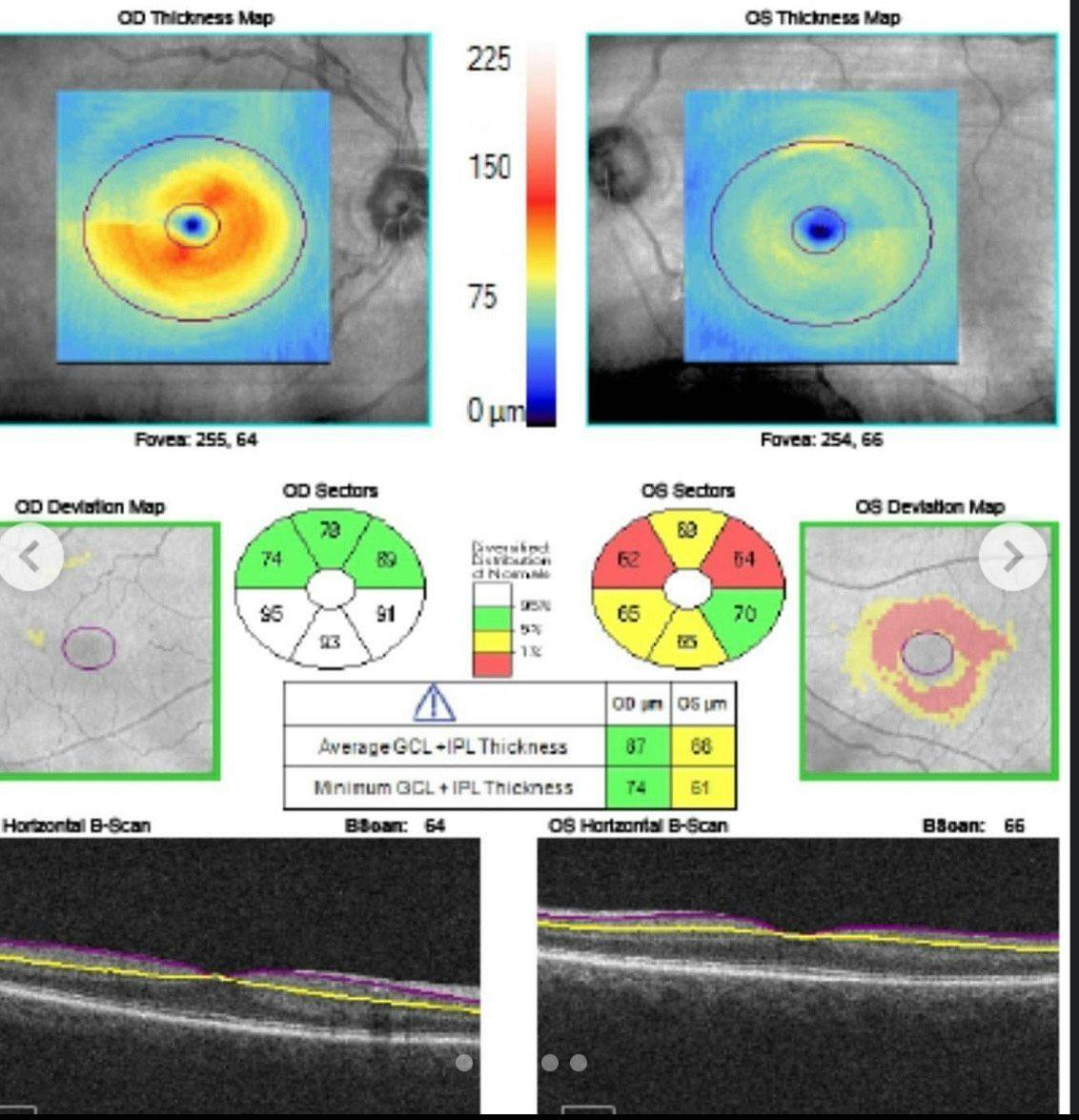
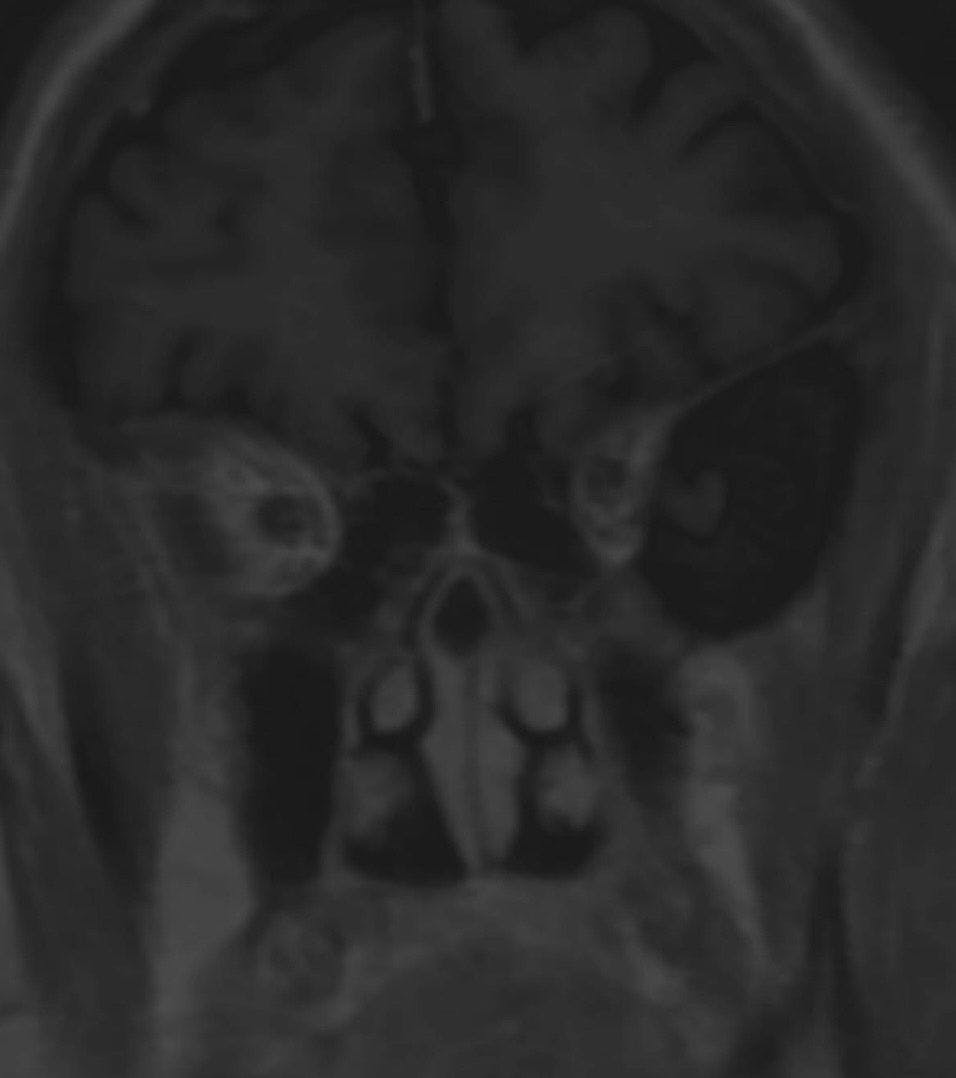
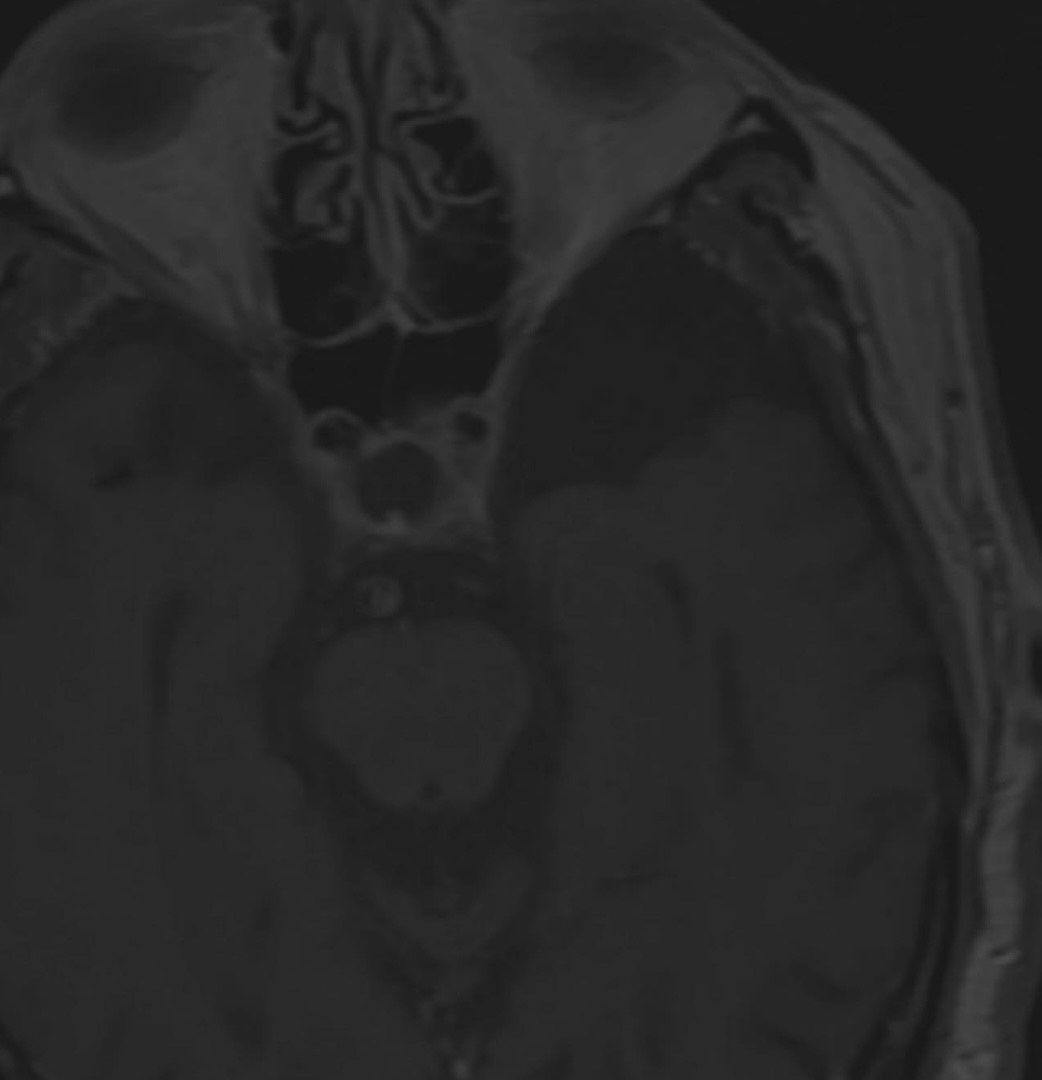
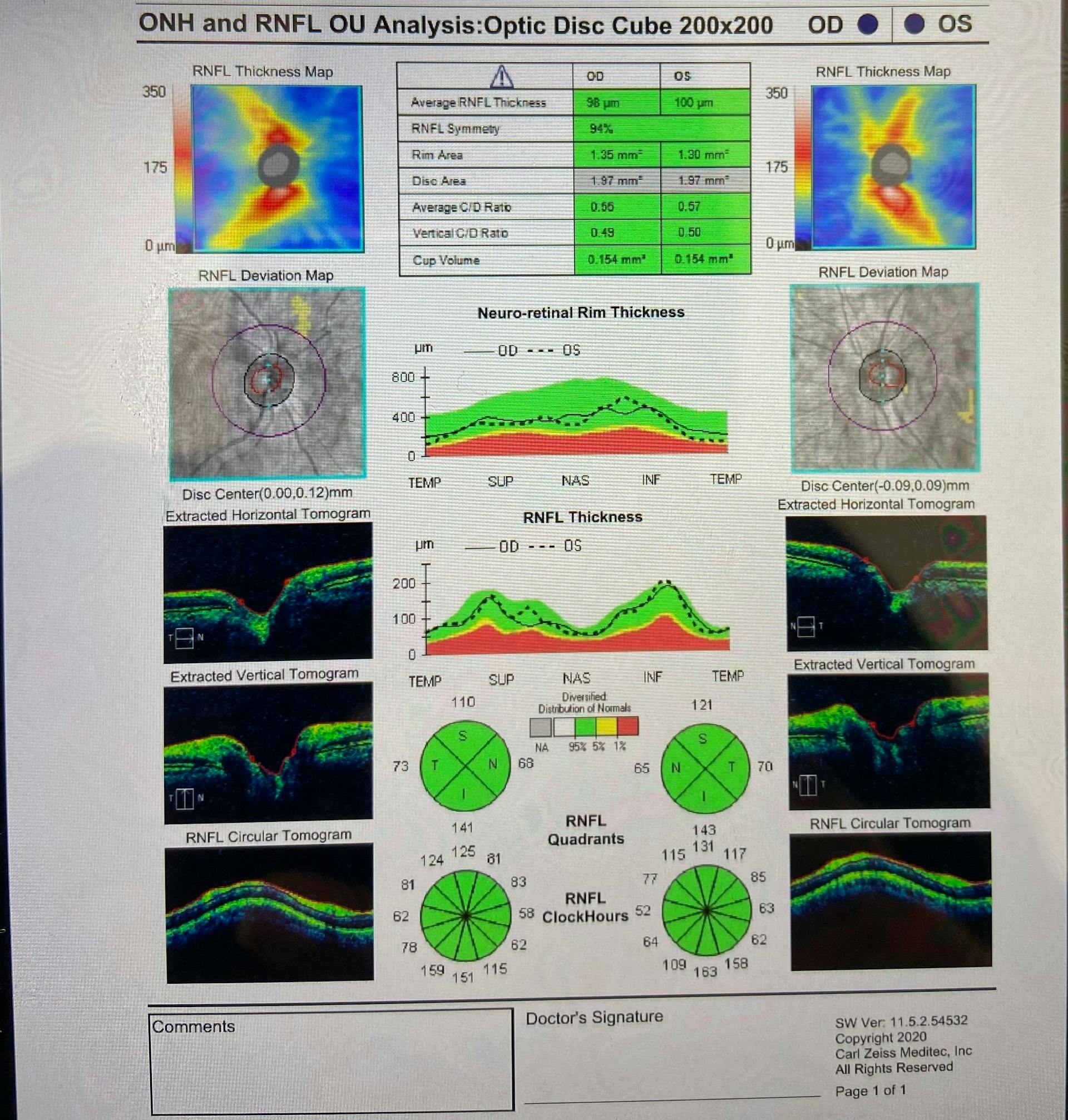
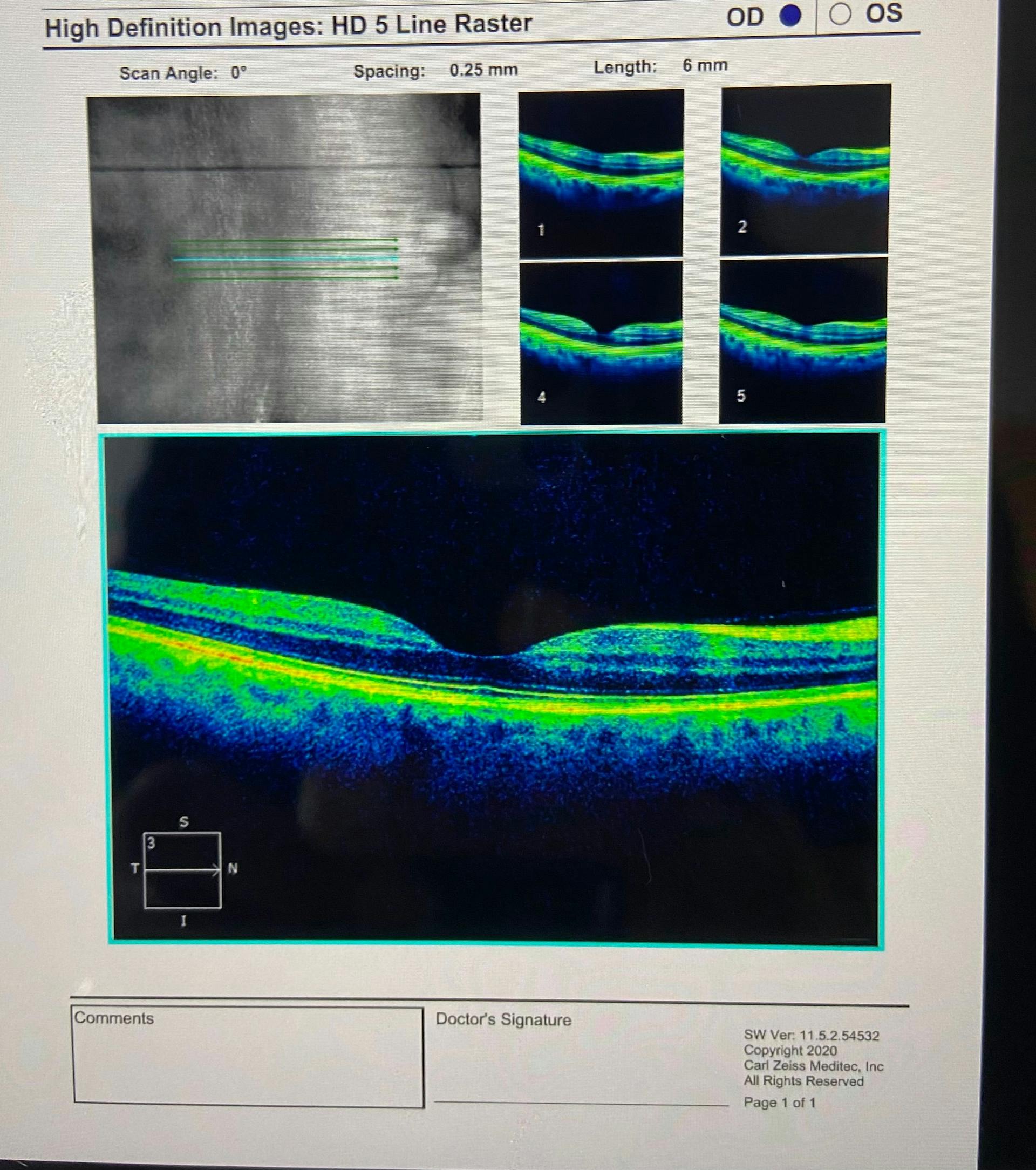
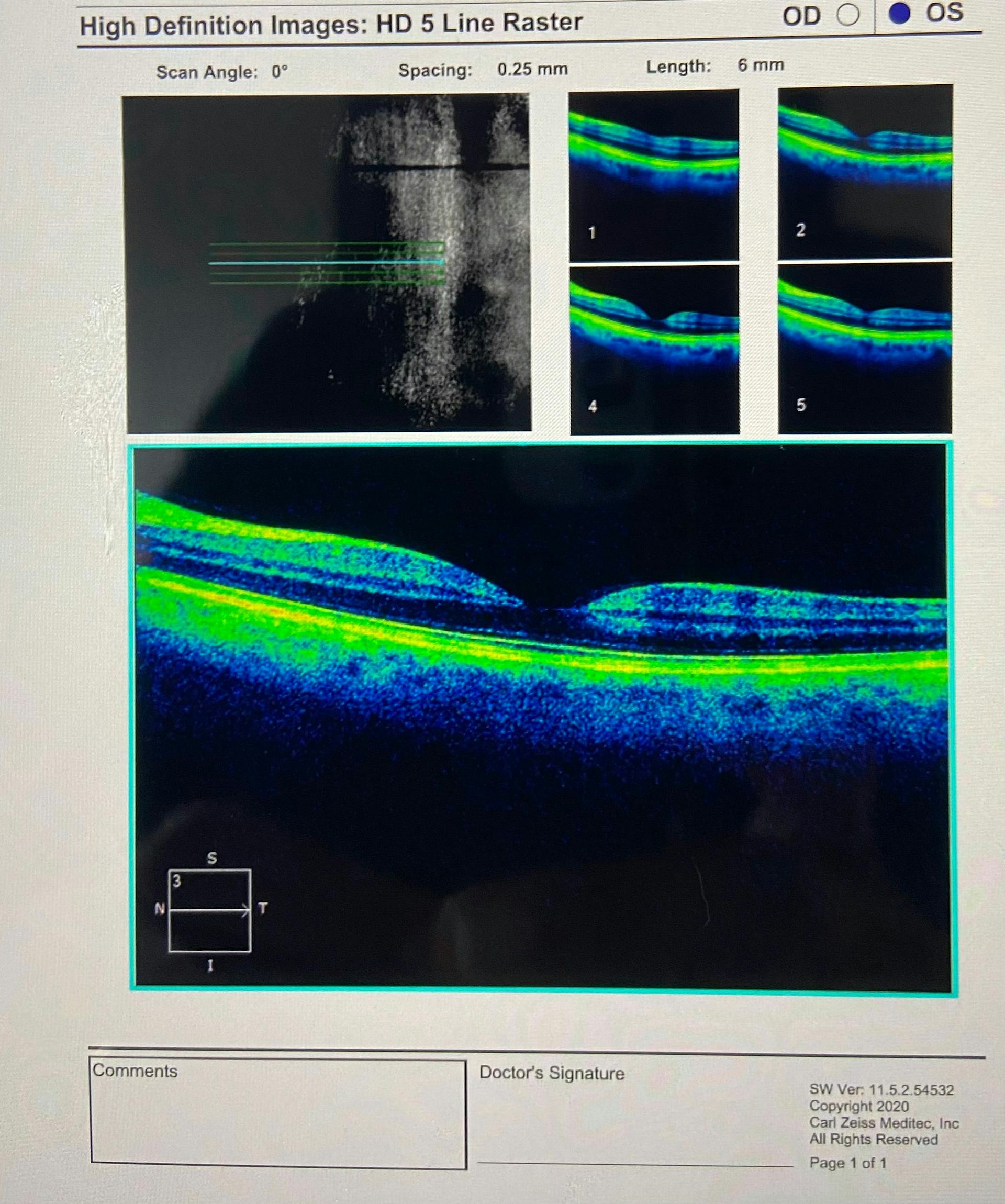
Dr. Rhoton’s case demonstrates the importance of preliminary testing as well as OCT imaging in a 72-year-old patient who had normal exam findings—except for an afferent pupillary defect that revealed a brain cyst.
The case
A 72-year old white male presented for his annual exam with no complaints or neurological symptoms. All exam findings were normal, including visual acuity of 20/20 OD/OS. The only abnormality was an afferent pupillary defect (APD) in the left eye as well as early cataracts in both eyes. The nerves looked healthy, but an OCT scan revealed a diffuse thinning in his retinal nerve fiber layer and ganglion cell layer in the left eye. Following that, I ordered an MRI of his brain and found he had a large, arachnoid cyst on the left side.

Second place: Stephanie Rowe, OD
Dr. Rowe’s case highlights how the COVID-19 virus was believed to lead to diplopia and cranial nerve palsy in one 45-year-old patient.
The case
A 45-year-old female presented with a chief complaint of diplopia and blurry vision OU for the past seven days. The diplopia was described as constant, horizontal, and resolved when covering one eye. The patient was accompanied by a family member who also noticed nystagmus, sluggish pupillary reactions, and an ocular motility deficit.
Eight days prior to the examination, the patient developed symptoms of coughing, sore throat, and fatigue. Testing confirmed COVID-19 infection. Ocular history was remarkable for myopia. Medical history was remarkable for depression. Medications included Wellbutrin XL, Layolis Fe, Naltrexone, Vitamin D3, Delsym, and Afrin nose spray.
The exam
The patient’s entrance visual acuities were 20/20 OD and 20/20-1 OS. Pupils were round, equal in size, and sluggish in reaction OU. No APD was noted. Confrontation fields were full to finger count OU. Extraocular motilities revealed a horizontal nystagmus. Limited abduction of the left eye was noted. Cover test results revealed a constant left esotropia at distance (10 prism diopters) and near (8 prism diopters). Color vision results were 14/14 OD and 14/14 OS via Ishihara. Intraocular pressures were 14 mmHg OU. Anterior segment results were normal OU. Trace cortical cataracts were noted OU. Dilated fundoscopy showed healthy optic nerves, blood vessels, macula, and peripheral retina OU. Zeiss CIRRUS 5000 OCT confirmed healthy optic discs and healthy macula
The diagnosis
Sixth nerve palsy, left eye; nystagmus and binocular diplopia.
Management
An urgent referral was made to our local hospital emergency department for neuroimaging. Our office called the emergency department to inform them of the patient’s condition and her office notes were faxed to the emergency department.
Follow-up
The patient went directly to the hospital emergency department. The hospital’s emergency physician called our office with the test results. Computed tomography, magnetic resonance imaging of the brain and orbits, and magnetic resonance angiography results were unremarkable. The patient’s symptoms were concluded to be associated with her COVID-19 infection. The patient was prescribed an oral steroid with tapering instructions and was discharged from the hospital the following day. On follow-up call with the patient, she stated that her symptoms of diplopia, blurry vision, and nystagmus had completely resolved over the next six days following our initial encounter. She requested to schedule a follow-up visit with us after her systemic symptoms resolved.
The sixth cranial (abducens) nerve provides innervation to the lateral rectus muscle. The most common causes of a sixth nerve palsy in adults are diabetes, hypertension, traumatic brain injury, stroke, Lyme disease or other infection, brain tumor, multiple sclerosis, or meningitis. Our patient in this case developed an acute sixth nerve palsy in the absence of those comorbidities other than a diagnosis of COVID-19. The medical literature mentions that most nerve palsies associated with COVID-19 are temporary and the symptoms gradually resolve when compared to other neurological deficits associated with COVID-19. Despite the low incidence of nerve palsies associated with COVID-19, the number of individuals presenting with nerve palsies has increased since the COVID-19 outbreak.
Third place: Cassondra Lux-O’Callaghan, OD
Learn about a 91-year-old male one week post-cataract surgery, presenting with increasing ocular irritation and reduced acuity secondary to a retained lens fragment in the eye along with the resulting treatment approach.
The case
A 91-year old white male presented for a one-week post-operative cataract surgery right eye as scheduled. The patient had noted, over the last few days, that he was having more irritation and blur out of his most recent surgery eye. He was still compliant with his surgical drops, right eye, but was finished with his drops, left eye.
The exam
The patient’s vision right eye was 20/40-2, and left eye was 20/20-1. Ocular pressures were 17 mmHg and 12 mmHg, right and left eye respectively. Anterior segment evaluation right eye presented with 2+ cells without flare along with 1+ diffuse corneal edema and increased conjunctival injection.
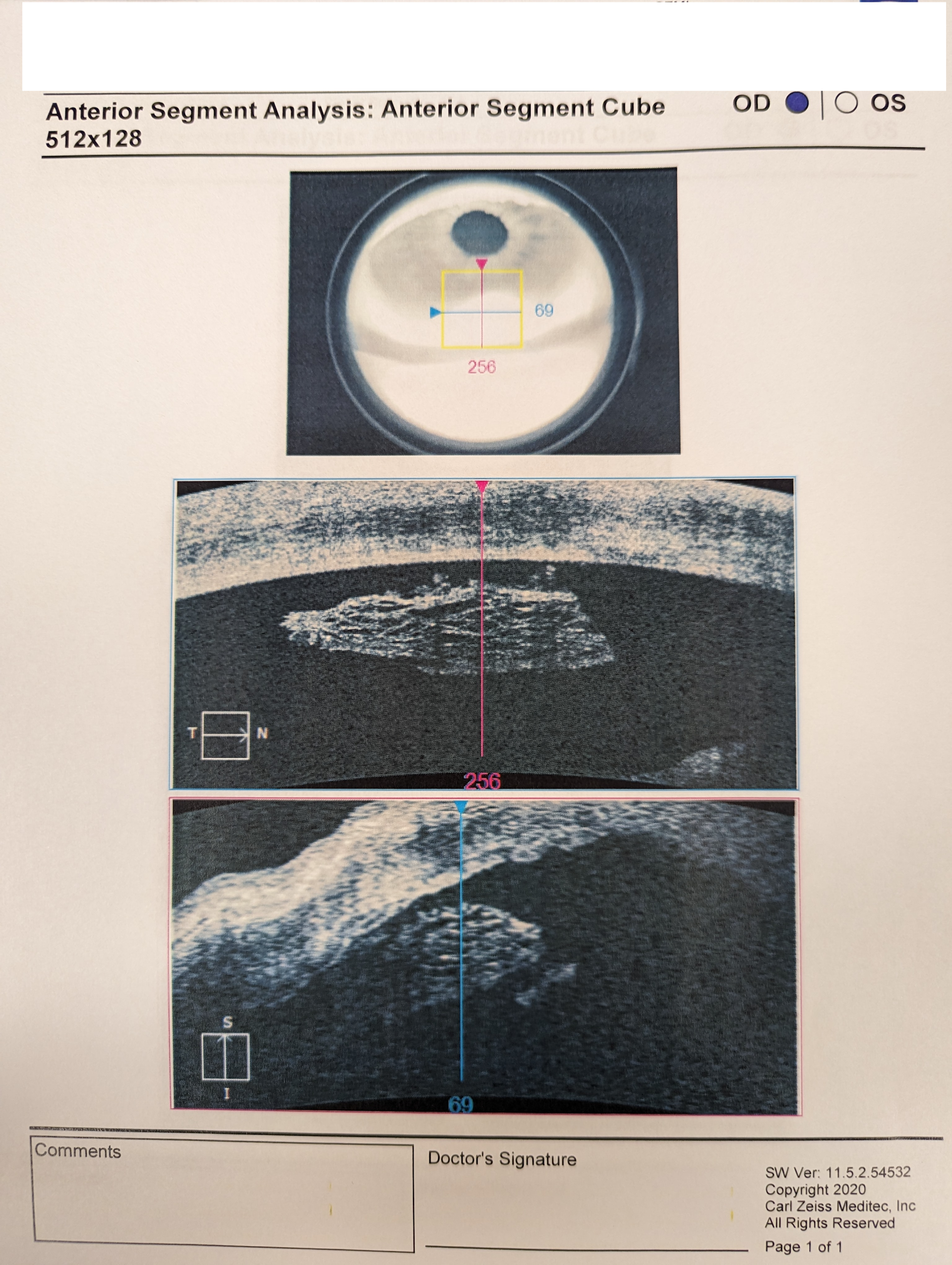
No Seidel’s sign was present. In the anterior chamber, inferiorly, a small fragment of debris was noted. It was free floating and around 1 mm in size. An anterior segment analysis: anterior segment cube 512x128 was performed to rule out residual viscoelastic versus retained lens fragment (see specialty testing). A macular OCT was also performed, both eyes, to rule out macular edema causing the reduction in vision—but was unremarkable.
The diagnosis
The irritation was determined to be from a retained lens fragment status-post cataract surgery. The patient was referred back to the surgeon for further evaluation and possible treatment. The patient was diagnosed with cataract extraction status, right eye (Z98.41), cataract extraction status, left eye (Z98.42), cataract (lens) fragments in eye following cataract surgery, right eye (H59.021).
After further evaluation, through professional correspondence letters, we were informed that the co-managing surgeon increased the patient’s postoperative steroid medication and planned on monitoring closely for improvement in inflammation and dissolving of the fragment over time. The patient is at a slightly higher risk of macular edema after cataract surgery due to the increase of inflammation, but will be monitored closely for signs of edema as well.
Discussion and conclusion
The OCT was important to help identify what material the fragment consisted of. Retained viscoelastic from the cataract surgery would most likely have presented as a uniform, solid mass. In this case, the fragment presents with jagged borders and layers, indicating it is most likely a lens fragment after phacoemulsification. If a fragment is unable to be viewed on a routine slit lamp exam, but is suspected as a differential diagnosis for worsening vision and increased inflammation or edema at follow up, an anterior segment OCT (along with gonioscopy) may be warranted for further evaluation. In this case, the fragment was large enough to be observed in a slit lamp exam and was easily noted with anterior segment OCT, therefore gonioscopy was not needed for the diagnosis. This patient was easily assisted with increased steroid drops and overall was happy with his surgical outcomes for both eyes. Per the last correspondence received, he did not need to undergo further surgery such as a pars plana vitrectomy and/or lensectomy. This is the best outcome to reduce risk of further complications with repeat surgeries.
Fourth place: Carolina Mercado, MD
Discover how a chief complaint of ocular irritation and clinical findings of inferior symblepharon turned into a diagnosis of latent tuberculosis.
The Case
An 80-year-old male patient, presented with 3-month irritation OD. He had no previous ocular history.
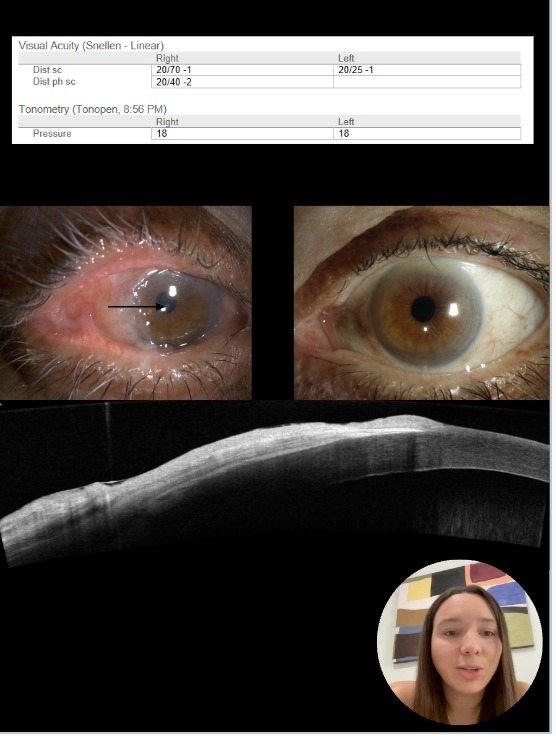
The exam
On exam, the patient showed evidence of anomalous temporal conjunctiva and inferior symblepharon. On anterior segment ocular coherence tomography using the ZEISS CIRRUS, a diffusely thickened and hyperreflective epithelium was noted along with subepithelial hyperreflectivity.
The patient was biopsied for concern of malignancy and granulomatous inflammation was noted on histopathological analysis. For this reason, malignancy was excluded and further testing ordered for sarcoidosis, tuberculosis(TB), and syphilis.
The diagnosis
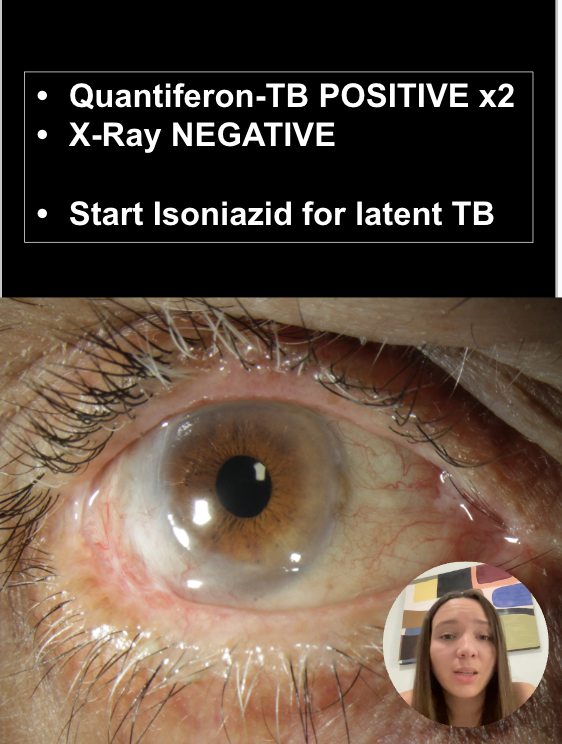
Quantiferon beta was positive twice, a chest x-ray was normal, and a diagnosis of latent TB was made.
Management
The patient started a course of oral isoniazid. Early after starting treatment inflammation subsided noticeably in the temporal conjunctiva.
