What is your lens of choice when performing funduscopy?
One notices that when using the slit-lamp biomicroscope to examine the anterior and intermediate structures of the globe, the microscope base, even in its most forward position, fails to “reach” the back of the patient’s eye. This is due to the highly convergent powers of the cornea and crystalline lens, which cause light to bend to a point before it can be focused on the posterior tissues.
One method to overcome this is by neutralizing the converging power of the subject’s eye, as by placing a high-minus element unto his cornea. This is how the Hruby lens and the central element of the Goldmann 3-mirror contact-lens work.
Given the relative inconvenience of contact funduscopy, however, the author performs such examination only a handful of times per week.
Although limited by a narrow field of view, the fundus representation of the Goldmann is bright, clear, detailed, and stable; it also depicts proper orientation, in which what is seen superior in fact lies superior inside the patient’s eye.
Direct Ophthalmoscopy
Another approach is to directly observe the retina using a hand-held ophthalmoscope, wherein one can contemplate plano light entering the subject’s eye, being concentrated onto and reflected by his retina, leaving the patient as once more plano, entering the doctor’s own eye, and being focused as a clear image on her fundus.
This method yields high magnification by allowing the doctor to be very near to her patient’s fundus (like scanning the details of a penny by holding it a couple of centimeters from one’s eye), however it greatly restricts her field of view (to about ten degrees), and it precludes stereoscopic examination.
The skill of hand-held direct ophthalmoscopy has waned over generations of eye-care practitioners, and the speaker himself admits to exercising it rarely and with limited competence.
The more modern and now ubiquitous approach to the clinical fundus examination is of indirect ophthalmoscopy, either with the head-mounted binocular indirect ophthalmoscope (B.I.O.), or with the slit-lamp biomicroscope (S.L.).
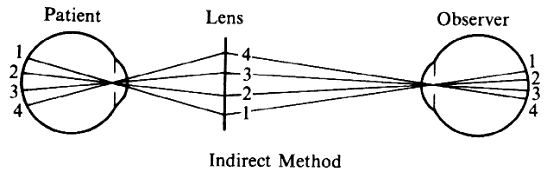
Indirect Ophthalmoscopy
In indirect evaluation, light is shone past a plus-power lens (e.g., 20D, 90D), which focuses it onto the patient’s retina, whence the photons retrace this path to form an aerial picture of the subject’s fundus. The doctor thus examines a physical image of the posterior segment, which by requirement is inversed horizontally and vertically.
The physics of indirect ophthalmoscopy allows far greater field of view than accessible with direct-viewing systems, and stereoscopic analysis remains feasible. Nevertheless, the optical bases of the technique are sometimes forgotten, and practitioners are privy to consternation from the myriad funduscope options available from various manufacturers.
Funduscope Design
A common funduscope is nothing more than a single-element optical system — literally, one piece of glass, contained within a metal ring that facilitates handling.
This is true of both B.I.O. and S.L. lenses, and indeed these devices ought to be conceived along one continuum ranging from around fourteen to one-hundred-and-twenty diopters (Ocular Instruments’ 2004 brochure for its MaxField product-line well elucidates this notion).
Agreeing to the simplicity of the funduscope’s design abets the doctor to look through creative marketing techniques developed to cast products into a vacuum of exciting and enigmatic names, such as Volk’s “Super” and “Digital” series. Successful
companies in any field promote their goods upon an understanding of both the knowledge and the ignorance of their target consumers; therefore, to make an educated decision, it is essential the clinician feel comfortable with the rudiments of the fundus lens.
Properties of Lenses
Finished lenses have several properties, comprising geometric design, coatings, and material, which together influence characteristics such as center- and peripheral-image clarity, thickness, weight, dispersion qualities, scratch-resistance, shatter-resistance, cost, and others. Despite these intricacies (which will briefly be reviewed near the conclusion of this essay), only two fundamental facets of the funduscopy element must be comprehended for pragmatic selection of a lens in the context of clinical practice: power, and diameter.
The power of an element describes the magnitude by which it bends light into focus as an image. In turn, its power commands two traits of the funduscope: magnification and field of view.
Magnification in indirect ophthalmoscopy is calculated under the assumption that the patient’s eye is a plus-sixty–diopter optical unit. From one’s physics coursework, one recalls the equation that enlargement in this scenario equals the power of the patient’s eye, divided by the power of the fundus lens: Powerpatient’s eye ÷ Powerfundus lens = magnification.
Accordingly, the lower the power of the funduscope, the more it magnifies the patient’s retina.
Let us note, with respect to indirect ophthalmoscopy, magnification describes the ratio of the size of the aerial image to that of the patient’s actual retina.
Thus, magnification less than 1X implies minification, 1X states the image and the fundus are equal in proportion, and more than 1X indicates enlargement.
This is different from how the mag. of direct ophthalmoscopy is described (e.g., “15X” enlargement with a hand-held instrument), which contrasts size observed using the instrument, with that which would be seen from a standard viewing-distance (i.e., 25cm). Magnification between indirect and direct ophthalmoscopy therefore cannot be readily compared.
With respect to indirect funduscopy, let us consider a 60D S.L. lens: By our equation, we compute, 60 ÷ 60 = 1X magnification; regarding a 90D lens, one would find 60 ÷ 90 = .67X enlargement. Applying the same reason to B.I.O. funduscopes, the 20D lends 3X magnification, and the 30D gives 2X. It seems counterintuitive, however, upon one’s clinical experiences, that the 60D produces a smaller image than the 20D.
The reason S.L. funduscopes yield greater amplification of detail than B.I.O., is the former itself imbues considerable magnification, whereas using her headset the doctor relies upon only her naked eye to evaluate the aerial image of her subject’s retina.
For example, with a 50D element giving 1.2:1 representation of a patient’s 2mm-tall optic disk, the doctor may dial her slit-lamp to 10X mag. or to 16X, creating net enlargement of 12X or of 19.2X (i.e., 1.2X times 10X, or 1.2X times 16X). (It would be a bit incorrect to say the disk becomes 24mm or 38.4mm tall, as S.L.-magnification describes angular- rather than linear-enlargement, similar to direct ophthalmoscopy, discussed above.)
In fact, certain lenses, such as the 30D and 40D will function adequately with both B.I.O. and S.L. fundus examination. With respect to B.I.O., the 30D will appear to effect extensive minification, in comparison with typical lower-power B.I.O. lenses like the 20D and 25D; when the same 30D is applied to S.L. funduscopy, details will look extravagantly magnified, in contrast with higher-power S.L. lenses, such as the 60D and 90D.
Knowing the inconsistency and opaqueness of product naming, it is insurmountable to directly compare funduscopes by simply their titles. Instead, the doctor can manipulate the manufacturer’s statement of lens-magnification to determine the power of any element, should she choose to contrast dioptric values (the approach works well even across the items of different companies): The power of a lens will be equal to sixty diopters (the converging prowess of the patient’s eye), divided by the enlargement generated by the funduscope.
For example, Volk cites its Pan Retinal 2.2 lens as yielding 2.68X expansion, and its Digital ClearField as lending 2.79X; sixty divided by either of these quantities reveals that each funduscope is approximately twenty-two diopters in power. Further, the field of view of the former item is fifty-six degrees, and of the latter is fifty-five.
One thus concludes that, despite possible subtle differences in geometric curvatures, these two products will offer extremely similar clinical experiences. One also would understand given equal magnification and field of view, not only the powers but also the diameters of these two elements will be nearly identical (diameter will be discussed further, later in this essay).
As element-power increases, the focal point of the item is reduced, such a 20D is ideally held approximately 5cm from the patient, whereas a 60D is positioned much closer.
As well, the aerial image the lens produces itself lies roughly this same distance from the funduscope, in between the lens and the doctor. For this reason, high-power B.I.O. lenses (e.g., 28D, 30D) must be maintained closer to the patient’s eye, and the clinician herself might benefit from allowing her head slightly nearer to her patient.
In addition, early slit-lamp biomicroscopes were more restricted than modern instruments in how far back from the patient they could be manoeuvered, which sometimes impeded the possibility of using the 60D funduscope. This fact helped lead to the development of the higher-power 90D lens, which would become established as a workhorse piece in clinical ophthalmoscopy.
It must be recognized that classic S.L. funduscopes’ powers were calculated with inaccurate formulae, and the names of these lenses therefore do not correctly reflect the magnification they provide.
For example, rather than the expected 1X, 0.77X, and 0.67X, Volk’s 60D, 78D, and 90D products respectively provide 1.15X, 0.93X, and 0.76X magnification — each lens is of lower power than one supposes.
Further, other companies’ homonymous pieces vary in their own dioptric values: Ocular Instruments produces two versions of a 78D lens — one that is similar to Volk’s offering (yielding 0.98X mag.), and the other a truer seventy-eight–diopter element (giving 0.77X enlargement). Nikon’s 90D also is substantially more converging than Volk’s model, and is nearer to being ninety diopters. (In the remainder of this essay, for simplicity and consistency, we shall assume 60D, 78D, and 90D fundus lenses in fact are dioptrically equivalent to their titles.)
In part for such reasons, the essayist strongly disfavors the application of “conversion factors” to compute the supposed “real size” of retina structures, such as often is suggested regarding the vertical height of the optic disk.
Rather, one recommends documenting linear dimensions as read from the scale of the biomicroscope, in conjunction with specifying exactly which funduscope (brand and model) was used to acquire the value.
Further, it is erroneous to assume that even once a lens power is correctly determined, the same conversion factor should be applied to all eyes, given the significant inter-patient variability of ocular tissues. For example, a true sixty-diopter funduscope will yield 1X enlargement only when imaging an emmetropic patient with eye-power around this same magnitude.
In the case of a highly myopic patient, fundus detail would be greatly minified with any form of indirect ophthalmoscopy, and the matter would be further confounded (though not ameliorated) by whether the subject is wearing refractive correction.
The second consequence of element-power is upon field of view.
As it bends in closer proximity to one another the pencils of light leaving the patient’s retina, a higher-power funduscope will increase field of view.
For example, a 78D lens allows the clinician to see more of the patient’s posterior segment at once than does a 60D. Unlike concerns magnification, however, field of view depends not only on the power of a lens, but also on its physical diameter (this will be further discussed, later).
Each of these two factors can, in fact, amplify or nullify the effects of the other. For example, one would predict a 90D lens will offer greater field than a 78D; yet, manufacturer data, as well as clinical observation, reveal the opposite to be true — more retina can be viewed at once with the 78D lens (given sufficient mydriasis).
Indeed, a 90D and a 78D of the same diameter would lend field-of-view advantage to the latter; however, most 78D funduscopes are larger than 90Ds by enough margin that their sheer size allows the collection of pencils of light from farther peripheral patient-retina.
Another complicating factor concerning field of view is introduced by the size of the light source used to illuminate the patient’s fundus. Consider a slit-beam that is 2mm tall as read on the biomicroscope’s dial.
The markings of the dial correspond to constant linear values; that is, if the S.L. states 2mm, the light will in fact be 2mm in size in all circumstances — the beam will not be influenced by the magnification properties of the doctor’s funduscope.
If a 2mm-beam then is used to image the patient’s optic-nerve head — which we shall say itself also is 2mm high — and a 90D lens is applied to achieve this, the light-beam will exceed the height of the disk: the nerve-head will be imaged with 0.67X magnification, such it stands only 1.33mm, and therefore the slit-beam, to cover the disk exactly from bottom to top, will have to be decreased from 2mm to 1.33mm. (This geometric–optical phenomenon is why some doctors would apply a conversion-factor to the disk-measurement — multiplying the slit-height by the inverse of lens magnification [that is, by 1.5X] would carry the 1.33mm reading to its “true” value of 2mm. As mentioned above, the writer dismisses such behavior for several reasons.)
Further rumination reveals that this phenomenon — where funduscope magnification affects only the size of the patient’s retina, not of the doctor’s light-source — means a spot of light held at constant size will “cover” more of the subject’s posterior segment when used with a high-power lens than with a low-power.
In other words, the overall field-of-view comparison between a 90D and 78D funduscope is made such that: If the two lenses were of equal diameter, the 90D would create greater field; however, because the 78D is substantially larger than the 90D, it actually generates greater field of view; and, within the boundaries of a constant spot-size of light, the 90D at any time will contain more of the retina than will the 78D, however when the light-size is increased to fill the maximum space available for either funduscope to produce an image, the 78D will show greater field of view than the 90D.
Fields of View
Finally, a remark should be made on “static” versus “dynamic” fields of view, as these terms often are cited by manufacturers.
Static field describes the concept intuitive to most readers — that is, when the funduscope is held in place over the middle of the patient’s pupil, this is how much edge-to-edge retina can be captured. With B.I.O., the doctor usually can see this full real estate simultaneously, whereas with S.L., she must scan the area with her light-beam.
For these computations, a given pupil-size may be held constant, and the patient usually is assumed to remain looking straight ahead, and not to be altering his gaze-position. Contemplating manufacturers’ descriptions of dynamic field is a bit akin to interpreting the digital-zoom of a camera (which photographers will agree is a futile endeavor) — generally, it is most natural when comparing fundus lenses with one another to mind only the static field of view.
The field is “static” because the clinician does not move her funduscope, but rather leaves it centered over the patient’s pupil.
Dynamic field typically describes how much can be visualized by moving the fundus lens from one edge of the patient’s pupil to the other.
The second major facet of funduscopes is diameter. Unlike power, which oversees both magnification and field-of-view, lens-diameter has command essentially over only the latter.
Volk’s “SuperField,” for instance, is identical to its classic 90D lens, however the element occupies a greater physical space, thereby giving the same amount of magnification but a more encompassing field. The 30D funduscope, as well, is offered in two iterations — “large” and “small,” with the former offering enhanced field, at the possible expense of more difficult handling.
Whereas the field-of-view afforded by a lens’s dioptric power is quite independent of external factors, that created by enlarging the diameter of the funduscope is restricted by the size of the patient’s pupil. Accordingly, with an undilated patient, the large and small 30D may reify identical surface areas of the subject’s retina. Similarly, the SuperField may fail to deliver greater expanse than the 90D given a miotic pupil, however a 120D fundus lens (e.g., Ocular Instruments’ MaxField 120D, Volk’s Super Pupil XL) in fact should image more peripheral regions.
Brightness
In addition to field of view, an element’s diameter has bearing upon the brightness of the image it produces. In contrast with the 90D, the larger size of the SuperField not only captures photons reflected from more peripheral locations of the subject’s fundus, but also channels the light that was returned from central tissue however that followed a more peripheral path. In addition, small-diameter lenses, such as the 90D, often are easier for clinicians to use, particularly given poorly-dilated patients or those with obstructive media (e.g., anterior-capsule phimosis), as it is mechanically simpler to align the center of a small object over the middle of the subject’s pupil. Lower-power funduscopes tend not to be developed with very minimal diameters, given the compounding ills of decreased field-of-view and diminished image-brightness.
To the inquiry of the “ideal” funduscope, the doctor must recognize not only the above rudiments of lens-design, but also understand her own clinical preferences of ophthalmoscopy. For instance, the author enjoys gaining gestalt realization of his patient’s posterior segment with the B.I.O., and appreciating subtle details with the biomicroscope.
For this purpose, the former necessitates adequate field, and the latter sufficient magnification. Other clinicians may more frequently lean upon the S.L. to achieve sweeping landscapes of the retina, or may require the B.I.O. to analyze fine details in bed-bound patients. The proper tool is not a fixed entity, but a fluid concept that must fill the distinct needs of an individual clinician.
Doctors do face a handful of other questions when considering funduscope choices, which will now be briefly reviewed.
Lenses might be available in glass or in plastic, with the vast majority incorporating the former.
Glass has only a slightly higher refractive index than plastic, which allows these elements to be slightly thinner. Its dispersion constant (Abbe value) is negligibly higher, however as net chromatic aberration depends upon Abbe and lens-thickness, glass funduscopes induce slightly less than dispersion than plastic.
Perhaps most noticeable, the specific gravity of glass is more than one and a half times that of plastic, meaning these lenses are quite heavier than the latter. In addition, glass is far harder than plastic, and consequently is less prone to imbibing scratches over time.
Another concern may rise over optical quality from lens-design. Modern funduscopes, like camera lenses and progressive spectacles, incorporate computer-guided algorithms to determine which curvatures will negotiate the greatest balance between central and peripheral image-clarity (the two commonly compete with each other), as well as will minimize distortion.
As a practical matter, the images produced by classic funduscopes (e.g., 60D) appear fully suited to clinical purposes.
Design enhancements of newer models indeed may produce technically sharper images, however these are not necessarily within the tolerance of the doctor’s visual system.
Instead, such detail would be welcome in ophthalmic-imaging applications, as when one captures photographs that will be enlarged to immodest-size prints or digital representations.
Finally, fundus elements sometimes are found that have been imbued with yellow-light filtration, such the probability decreases of high-energy phototoxicity to the patient’s retina upon prolonged exposure to the doctor’s illumination beam.
Pragmatically, the likelihood of damage given typical funduscopy duration is very low, and, in the author’s experience, the yellow tint of such lenses can obfuscate the analysis of certain details.
In piloting among her choices of funduscopy lenses, it is important the eye doctor apply her rich knowledge of optics principles.
Despite their meretricious names and proliferating numbers, funduscopes are only single-element entities whose two most basic properties — magnification and field of view — are dictated by their power and their diameter; if these data are not clearly indicated by the company, the informed clinician will extrapolate them with knowledge of the lens’s magnification and its field of view, which typically are provided.
Ultimately, each doctor’s quintessential library of lenses will be led both by her understanding of funduscopes, and by the realization of how she herself favors to perform the ophthalmoscopic examination.