



Intended for US HCPs only
What is geographic atrophy?
Geographic atrophy (GA) is an advanced form of age-related macular degeneration (AMD) that could lead to irreversible, progressive vision loss.1 Progression can occur rapidly with the characteristic presence of sharply demarcated atrophic lesions (unifocal and multifocal in nature) due to the loss of the retinal pigment epithelium (RPE) and outer retinal loss. In as little as 2.5 years, non-foveal GA lesions (perifoveal) can progress to the fovea, affecting vision dramatically.2 For example, approximately 67% of patients with GA lose their ability to drive due to visual impairment within 1.6 years.3 Current estimates suggest that GA affects approximately 1.5 million people in the United States4—but only 1 in 4 may have been officially diagnosed.
Progression can be relentless with the potential to have a profound impact on psychological well-being coupled with activities of daily living, such as recognizing faces of family and friends, reading, or driving. Patients tend to not see immediate visual acuity changes earlier in the GA disease process, possibly due to the location of the lesions themselves. With this said, GA may still incur a visual deficit that can become more encumbering during certain scenarios or activities.
While some patients report no symptoms, others may note:5
- Difficulty with daily activities
- Blurred vision and/or presence of scotomas
- Reduced contrast sensitivity
- Metamorphopsia
For GA patients, early detection through imaging is key to early intervention and potential effective treatment strategies.
A treatment for GA secondary to AMD that slows the rate of GA progression6
IZERVAY is commercially available as a monthly, intravitreal injection for the treatment of GA secondary to AMD. It is the only approved GA treatment with a statistically significant reduction in the rate of GA progression at the 12-month primary endpoint across two Phase 3 clinical trials.7

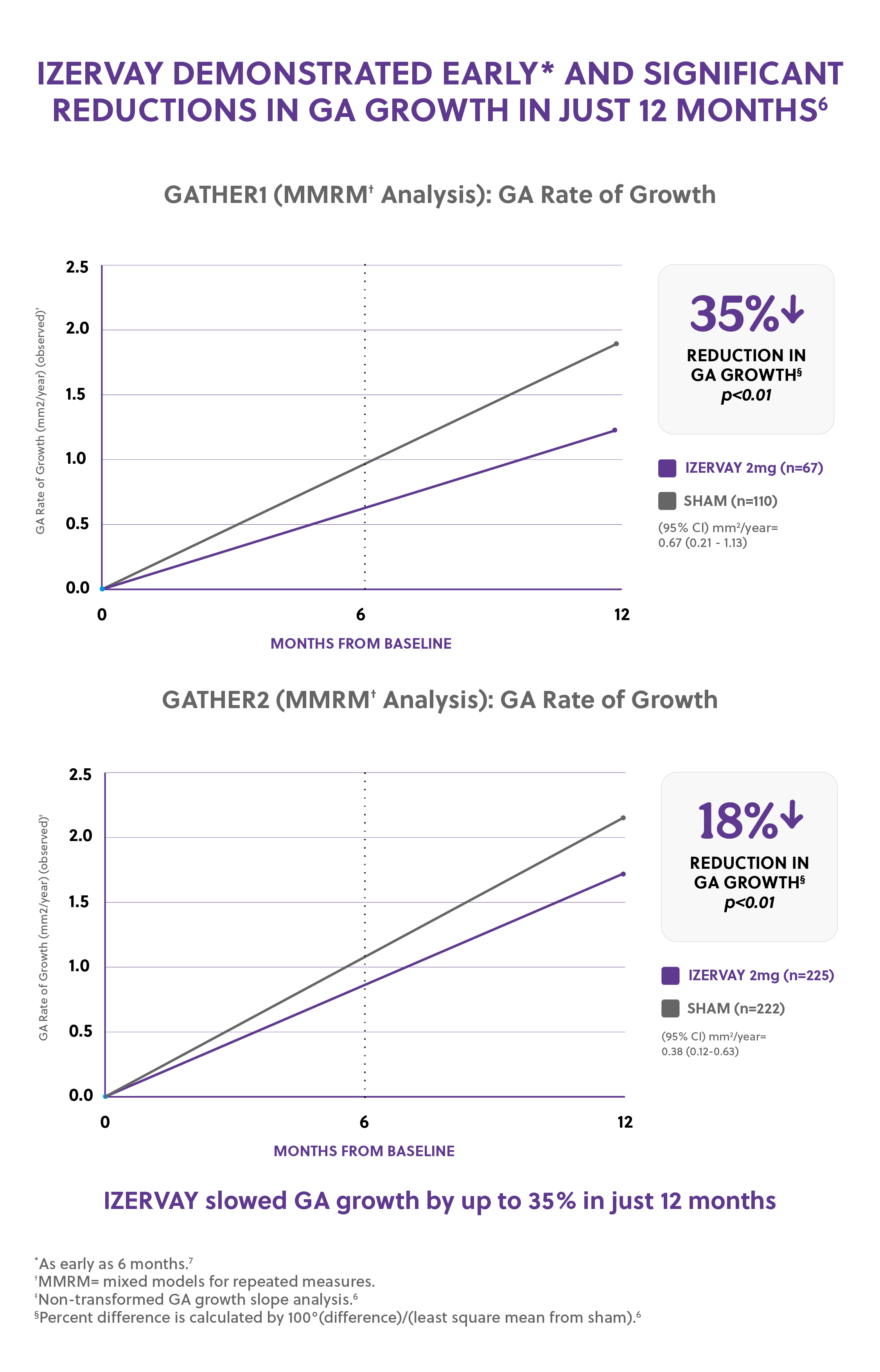
Trial Design: The safety and efficacy of IZERVAY were demonstrated in GATHER1 and GATHER2: two randomized, multi-center, double-masked, sham-controlled studies in patients with AMD. 292 patients were treated with IZERVAY 2 mg, while 332 patients received sham. The primary efficacy endpoint in both pivotal studies was the mean rate of GA growth (slope) from baseline to Month 12 over 3 timepoints: Baseline, Month 6, and Month 12. In each study, over a 12-month period, there was a statistically significant reduction of the rate of GA growth (0.10 mm/year; p<0.01 in GATHER1 and 0.05 mm/year; p<0.01 in GATHER2 with square root transformed data) in patients treated with IZERVAY compared to sham.
IZERVAY demonstrates consistent safety data and high patient retention with low adverse effects
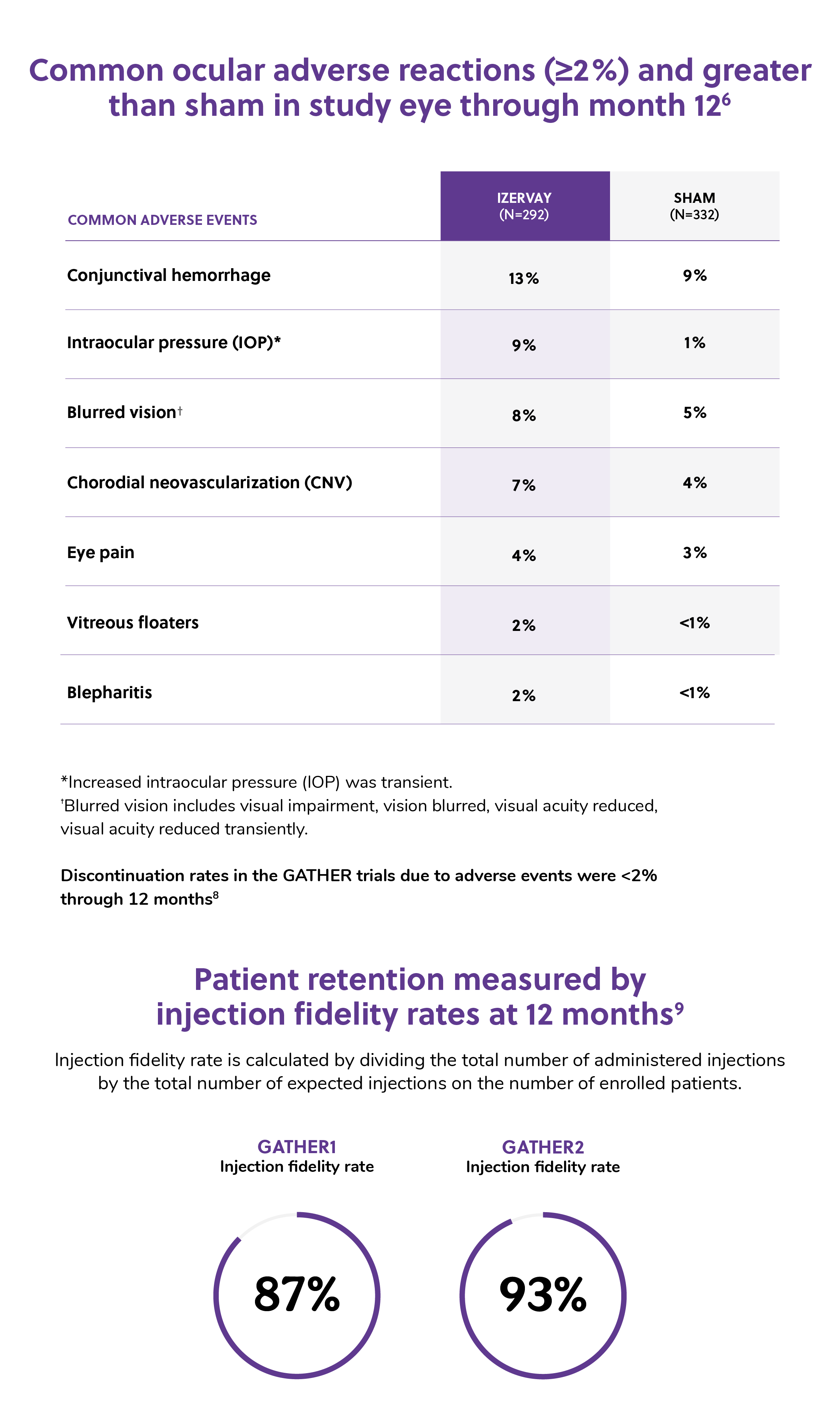
In the GATHER trials, IZERVAY was evaluated across more than 700 patients with GA. IZERVAY demonstrated a consistent safety profile with a high rate of patient retention.
There were no reported cases of ischemic optic neuropathy (ION), vasculitis, or endophthalmitis during the 12-month trial period and only 1 mild case of intraocular inflammation (IOI).8 In GATHER2, if a study participant developed choroidal neovascularization (CNV), they were treated concomitantly with on-label anti-VEGF therapy.

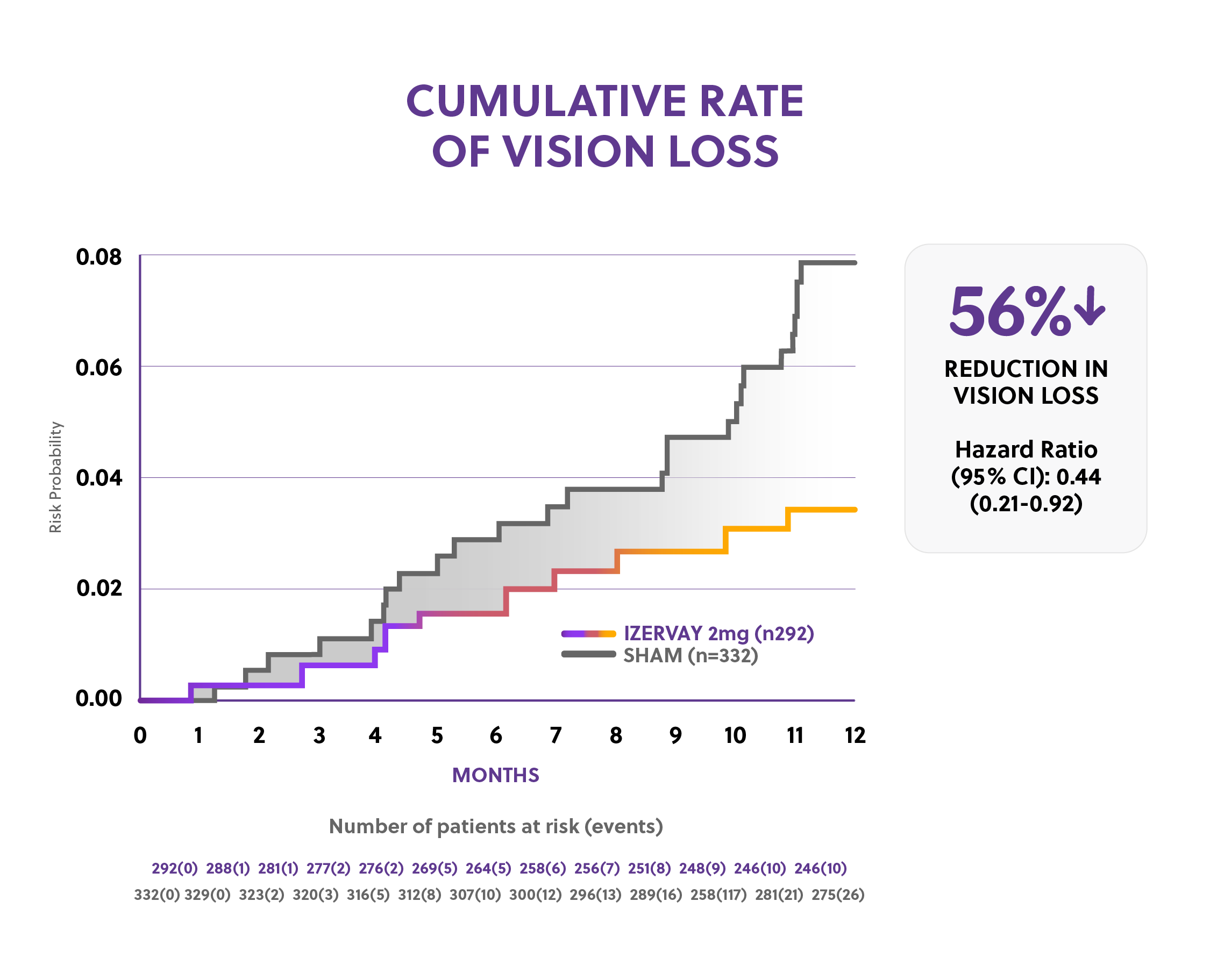
Post hoc analysis signaled a reduction in risk of persistent vision loss
In a post hoc analysis, a 56% risk reduction in persistent vision loss was observed with IZERVAY versus sham over 12 months. Persistent vision loss in this pooled analysis was defined as a loss of ≥15 letters (ETDRS) in BCVAfrom baseline measured at any 2 consecutive visits up to Month 12.

Special Notes:
- Masked image and adverse event analysis completed to further ensure vision loss was consistent with disease progression.10
- Given the exploratory post hoc nature of the data, these results should be interpreted with caution and cannot be considered conclusive.
* A loss of > 15-letter in BCVA is equivalent to doubling of visual angle and the gold standard for clinical meaningful visual acuity loss in pivotal ophthalmology studies.
†Persistence of vision loss is an indicator that vision loss was not acute and/or transient.
†Persistence of vision loss is an indicator that vision loss was not acute and/or transient.
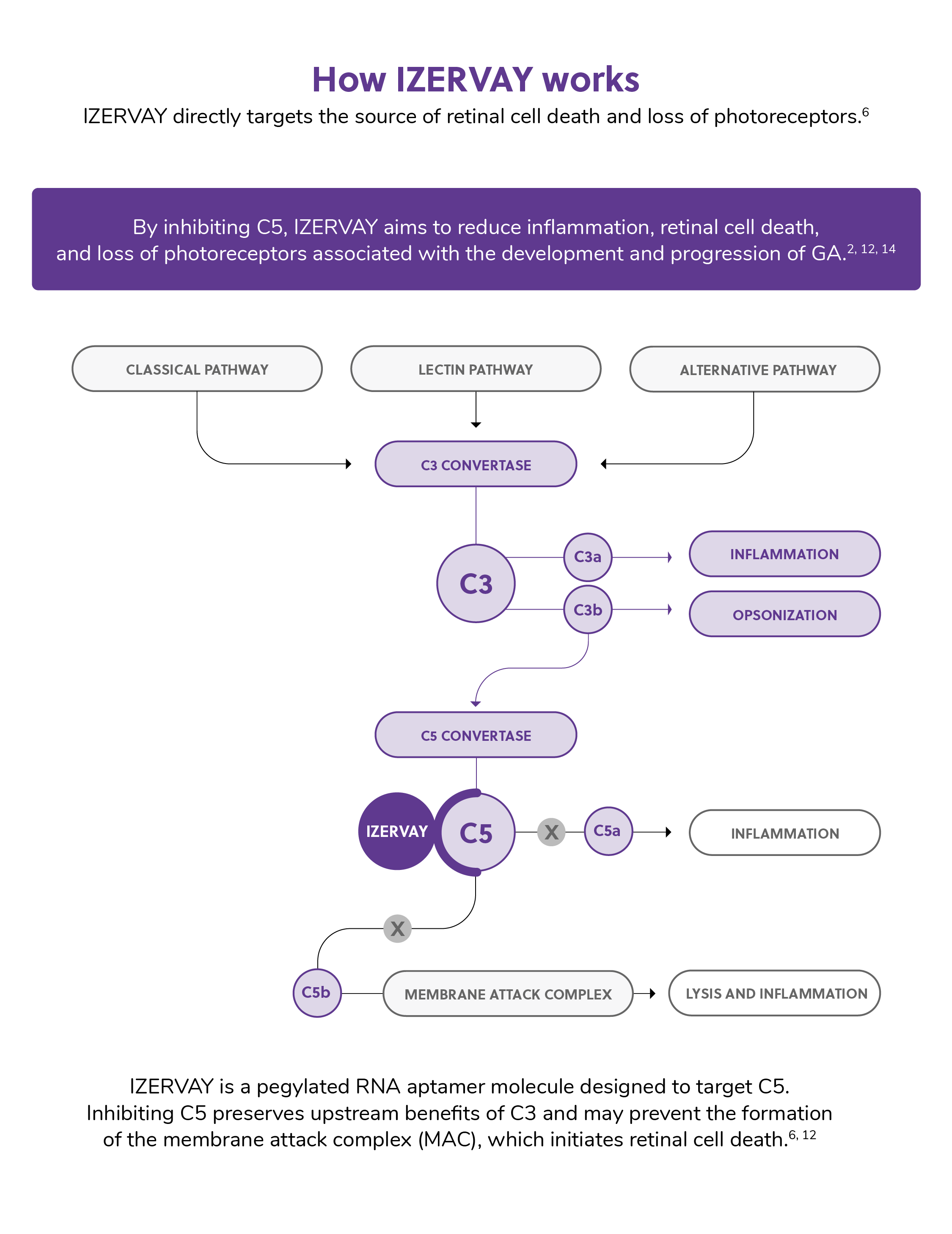
How does IZERVAY work?
Overactivation of the complement cascade, including C5 protein, is thought to play a role in initiating retinal tissue damage and eventual morbidity associated with geographic atrophy.11 IZERVAY, a pegylated RNA aptamer, targets C5 with the intention of potentially preventing formation of the membrane attack complex (MAC) which initiates retinal cell death.12

GA referral patterns: the collaborative care approach
Optometrists play an essential role in the early detection of GA, including patient education, building appropriate treatment and visual expectations, and proactively referring for treatment consideration depending on case presentation. Multimodal imaging can offer a comprehensive approach to early detection of GA and is critically important for understanding and monitoring disease progression.
Once GA has been detected, timely communication and collaboration with a retina specialist can assist with formulating an appropriate treatment plan based on disease severity.


Hallmark signs that may be indicative of GA
Progression from intermediate AMD (characterized by large drusen >125 μm and/or any AMD pigmentary abnormalities) to GA is defined by the presence of sharply demarcated atrophic lesions.13 Atrophic lesions represent a loss of the retinal pigmented epithelium, overlying photoreceptors, and underlying choriocapillaris, which can be visualized by various biomarkers on imaging modalities commonly available in most clinics.2,13
| Imaging Modality | Signs |
|---|---|
| Color fundus photography (CFP) | Sharply demarcated lesion, typically circular with increased choroidal visibility |
| Fundus autofluorescence (FAF) | Hypofluorescence with a sharply demarcated border |
| Hyperfluorescence surrounding atrophic lesion/indicative of lipofuscin accumulation and prognostic of GA | |
| Swept-source or spectral-domain optical coherence tomography (OCT) | Choroidal hypertransmission: increased light transmission into the choroid where the retinal pigmented epithelium (RPE) is attenuated or absent |
| Loss of RPE, photoreceptor (PR), and choriocapillaris layers |


Figure 1: Color fundus photography: Sharply demarcated lesion, typically circular with increased choroidal visibility.13 (Image credit: Paulo Stanga, MD, The Retina Clinic London.)

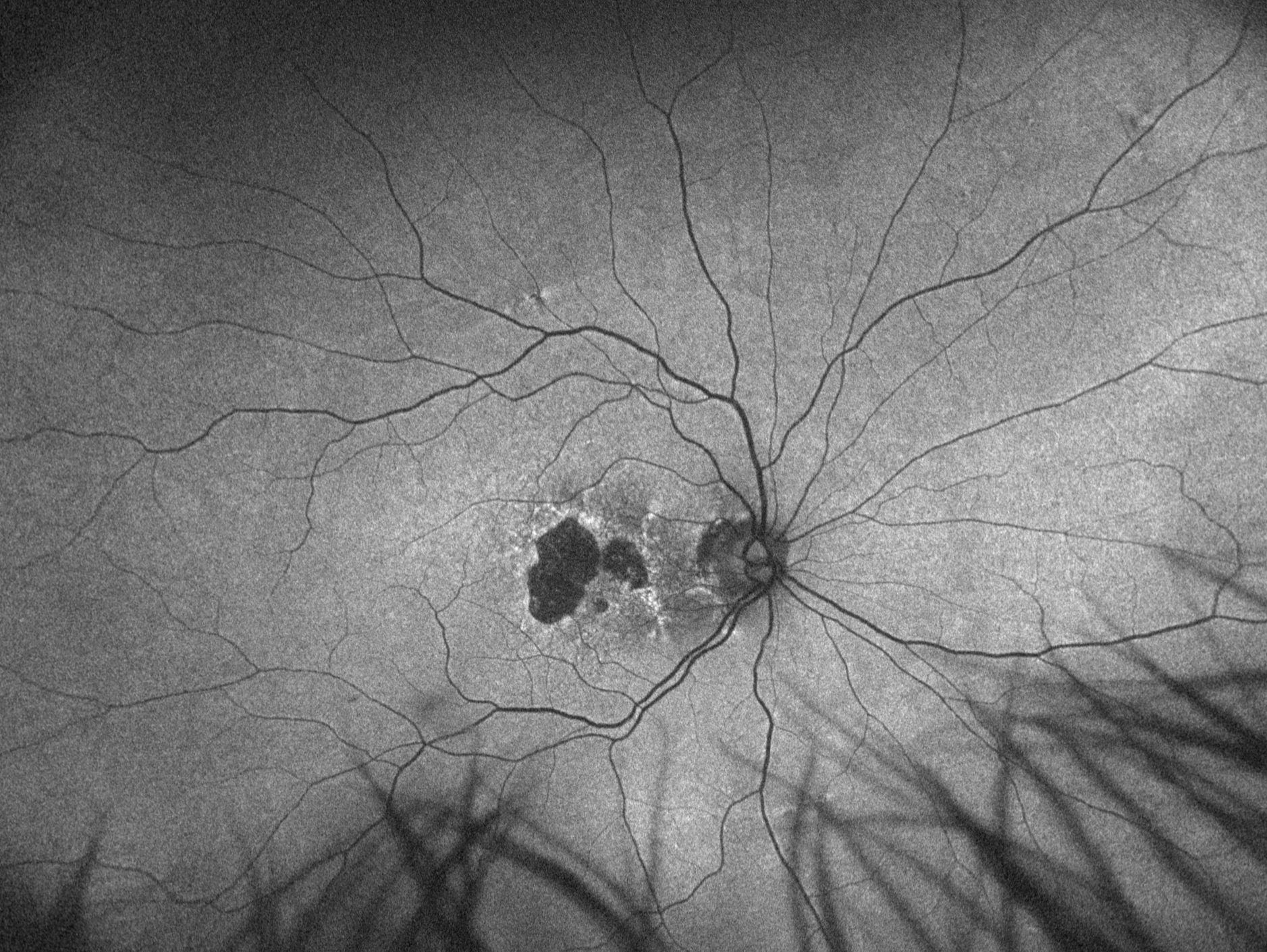
Figure 2: Fundus autofluorescence (FAF): Hypofluorescence with a sharply demarcated border. Hyperfluorescence surrounding atrophic lesion can be indicative of lipofuscin accumulation and prognostic of GA.13(Image credit: Paulo Stanga, MD, The Retina Clinic London.)

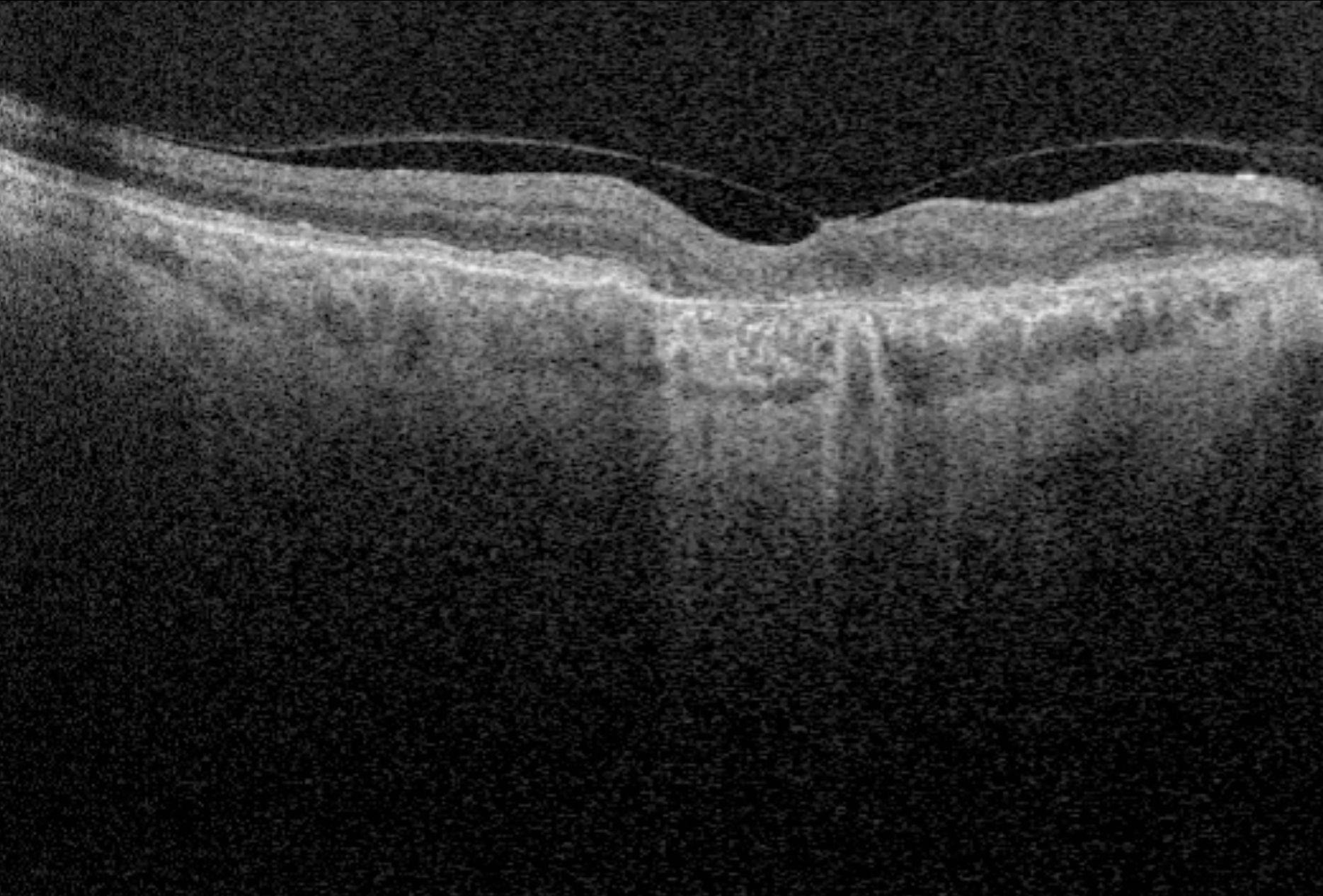
Figure 3: Optical coherence tomography (OCT): Choroidal hypertransmission can be characterized by an increase in light transmission into the choroid where the retinal pigmented epithelium (RPE) is attenuated or absent. Loss of RPE, photoreceptor (PR), and choriocapillaris layers. may also be seen.13 (Image credit: Paulo Stanga, MD, The Retina Clinic London.)
The role of patient education in GA identification and treatment
Patient education is a critical component in managing and treating GA. By empowering patients with knowledge and speaking to them with compassion as they prepare to live with a progressive disease, they may be equipped to better understand symptoms, potential impact on their vision and the importance of compliance with follow-up care and treatment plans.
Consider the following tips or protocol when educating patients:
Tip #1: Inform: Explain the condition in terms that resonate, and do so with empathy. Remember that your patient is likely overwhelmed with different emotions and fear. Reassure them that you will be there at every step to support them and explain to them there are treatments available now that offer more hope to patients with this disease.
Tip #2: Educate and set expectations: It is important to share with patients that symptoms of GA may not be overt.
- Highlight the need for consistent follow-up to monitor progression.
- Provide them with a GA symptom guide with simplified terminology (and definitions, if needed, for medical terms).
- Explain that GA can interfere with daily routines and independence very quickly. In 1.6 years, 67% of patients with GA lose the ability to drive3, and in two years, 50% of patients with GA may lose up to two lines of vision.3
- Set proper expectations for the referral with patients giving them a clear understanding of the process involved and potential outcomes.

Tip #3: Manage Expectations:
- Ensure patients understand that GA is a progressive disease that cannot be halted or reversed at this time.2
- Explain that with treatment, the rate of progression might be slowed, and that the goal of early intervention is to attempt to preserve the vision they have for as long as possible.3,5,10
Tip #4: Follow up: Emphasize the need for continuous care. Have an honest dialogue with your patients. Working with your patients to understand what is most important to them from a vision standpoint provides reassurance that you are dedicated to help preserve their sight for longer. Explain that this journey is a partnership where they need to be open to continuous monitoring and long-term treatment.
Summary
While we might not be able to reverse or fully halt GA progression, IZERVAY can potentially slow the progression and may preserve a patient’s vision for a longer period of time than if they received no treatment.
Here are some helpful takeaways:
- Proactively look for GA and document diagnosis.
- Work with your retina specialist to understand preferred practice patterns.
- Collaboration between optometrists and retina specialists when sharing image studies and chart notes is important as are consistent communication and appropriate patient care management.
- Align with your retina specialist on which patients will be given priority.
The sooner you can detect GA, the greater the opportunity to slow GA progression and provide some level of hope for your patients.
Acknowledgments
This article was peer-reviewed by Michael S. Cooper, OD, President, Visionary Medical Education, LLC.
This article was peer-reviewed by Michael S. Cooper, OD, President, Visionary Medical Education, LLC.
Copyright © 2024 Astellas Pharma Inc. or its affiliates. All trademarks are the property of their respective owners. All Rights Reserved. US-AP-2300423 01/24
