



One decade ago, our choices for treating glaucoma patients were very limited; typically, you would start with intraocular pressure (IOP) lowering eye drops, with Argon or selective laser trabeculoplasty as an adjunct. If we needed a lower IOP or the patient could not tolerate eye drops due to side effects, our next step would be a penetrating procedure, such as trabeculectomy. If trabeculectomy failed, glaucoma drainage devices (GDD) would be our next step.
For end-stage uncontrolled glaucoma, which was unresponsive to all the above-mentioned options, cyclodestructive procedures were the last resort.
Traditional surgical procedures are great when successful and free of complications, but sight-threatening complications, such as bleb leak/infection, endophthalmitis, suprachoroidal hemorrhage, and a high rate of treatment failure are innate components of these procedures.
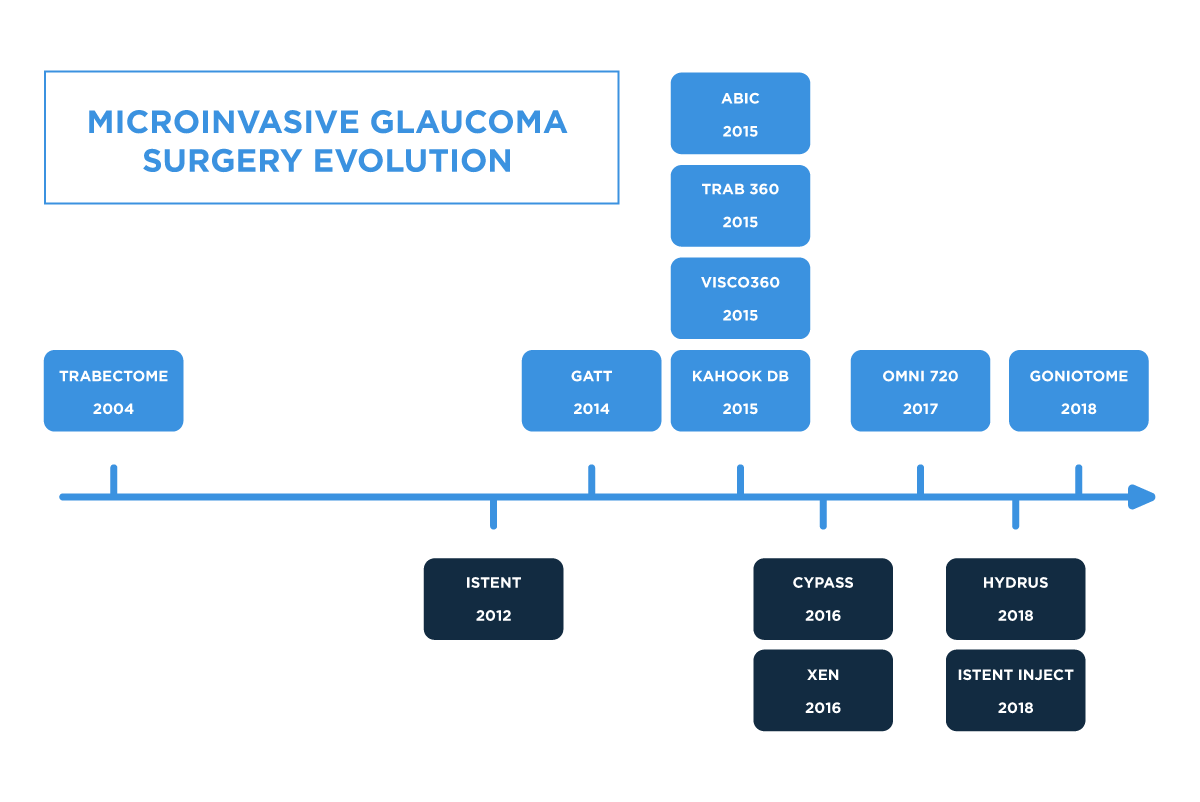
For decades, the glaucoma world has been looking for safe and effective procedures to bridge the gap between drops, laser, filtering, and shunting procedures. This search resulted in the development of a new group of glaucoma procedures called minimally (micro) invasive glaucoma surgeries (MIGS).
The first member of the group was Trabectome which was introduced in 2004. It was followed by iStent in 2012 and many other options, which were introduced during the past decade.

Having many tools in our armamentarium is a great win for the glaucoma surgeon, but with so many options comes the challenge of choosing the right one. So, the important question we try to answer in the following sections is how you select the right option for your patients. However, before you can select the right one, it is important to know what is available and what each device does.
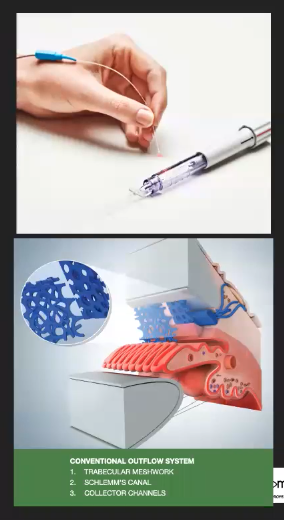
Table 1 summarizes the available MIGS procedures with their mechanism of action: incising or excising the trabecular meshwork (TM) or goniotomy, angle bypass, dilation of the Schlemm’s canal (canaloplasty), access into subconjunctival space or suprachoroidal space, or a combination of these mechanisms.
Table 1. Minimally invasive glaucoma procedures
| Mechanism of action | Product | Distributor | Year approved | Angle anatomy | Stage of Glaucoma | Stand alone | Implant |
|---|---|---|---|---|---|---|---|
| Gonioscopy | Trabectome | Microsurgical Technology | 2004 | Open and Narrow | Early, moderate, Severe | Y | N |
| Gonioscopy | KDB | New World Medical | 2015 | Open and Narrow | Early, moderate, Severe | Y | N |
| Gonioscopy | GATT (with iTracK) | Nova Eye | 2014 | Open and Narrow | Early, moderate, Severe | Y | N |
| Gonioscopy | TrabEx (+) | Microsurgical Technology | 2018 | Open and Narrow | Early, moderate, Severe | Y | N |
| Trabecular meshwork bypass | iStent | Glaukos | 2012 | Open | Early, Moderate | N | Y |
| Trabecular meshwork bypass | iStent inject | Glaukos | 2018 | Open | Early, Moderate | N | Y |
| Trabecular meshwork bypass | iStent inject (W) | Glaukos | 2021 | Open | Early, Moderate | N | Y |
| Trabecular meshwork bypass | Hydrus | Ivantis | 2018 | Open | Early, Moderate | N | Y |
| Canaloplasty | ABIC w/ iTrack | Nova Eye | 2015 | Open | Early, Moderate | Y | N |
| Canaloplasty | Visco 360 | Sight Sciences | 2015 | Open | Early, Moderate | Y | N |
| Subconjunctival space | Xen | Allergan | 2016 | Open and Narrow | Early, moderate, Severe | Y | Y |
| Combination | OMNI | Sight Sciences | 2018 | Open and Narrow | Early, moderate, Severe | Y | N |
| Suprachoroidal space | Cypass* | Alcon | 2012 | Open | Early, Moderate | Y | Y |
*no longer in production
Available devices by mechanism of action
For incising or excising the trabecular meshwork
Trabectome

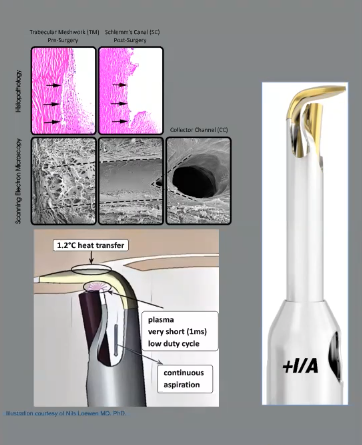
Trabectome was approved by the Food and Drug Administration (FDA) in 2004. This device ablates the TM and reopens the natural aqueous outflow pathway using an electrical current. An irrigation/aspiration system is included in the handpiece for maintaining the anterior chamber (AC) and management of intraoperative hyphema. Because of this AC maintaining property, this procedure is an ideal option for surgeons who are new to the MIGS world. Since AC is well formed during the whole procedure, the risk of hyphema blocking the view is minimized, enabling the surgeon to focus on the angle anatomy.
Kahook Dual Blade (KDB)

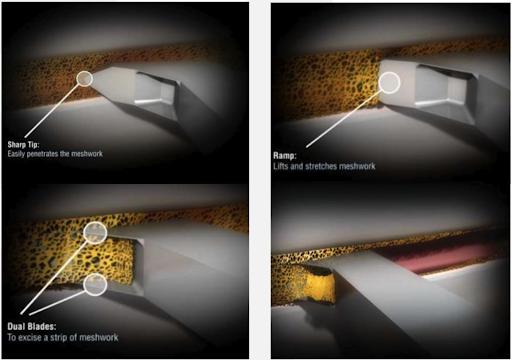


Kahook dual blade was approved in 2005 by the FDA. This device is a single-use stainless steel dual blade with a ramp that is used to manually remove a strip of TM over a 3-4 clock-hours area. The strip could be sent for pathological study of the TM.
Gonioscopy Assisted Transluminal Trabeculotomy (GATT)

First described in 2014 by R. Fellman, GATT cleaves the TM up to 360 degrees, allowing reestablishment of conventional pathway for aqueous. This procedure could be performed either by using the specially designed illuminated catheter-like iTrack from Nova Eye or by utilizing a 5-0 Polypropylene suture for a, cost-effective approach—appropriate when a surgeon masters this angle surgery.
TrabEx/TrabEx+


Approved by FDA in 2018 for surgical removal of a strip of TM, TrabEx—originally called Goniotome—has laser-cut sharp blades for TM excision. TrabEx+ incorporates irrigation-aspiration (I/A) for AC pressurization, management of bleeding, and maintenance of a good angle view while performing the goniotomy.
For bypassing the trabecular meshwork
iStent

The first generation iStent was approved in 2012 by FDA as the first ab interno micro bypass device to restore aqueous physiological outflow for mild to moderate glaucoma performed in conjunction with cataract surgery. This stent is magnetic resonance conditional and is safe in specific MRI machines. iStent can be combined with cataract surgery, and its less steep learning curve makes it an ideal option for comprehensive ophthalmologists.
iStent Inject

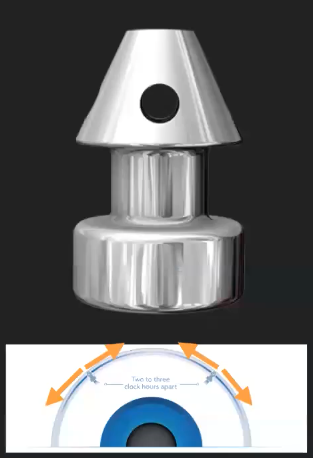
The second generation iStent inject is a biocompatible titanium grade. It was approved in 2018 and is a modification of a previous version. There are two stents instead of one loaded in each injection system, which allows access to more collector channels by placing the stents a few clock hours apart in the Schlemm’s canal. This procedure is only performed when combined with cataract surgery.
iStent Inject W

This is a modification of the iStent inject. The main design change is a wider flange at the base for more stable insertion.
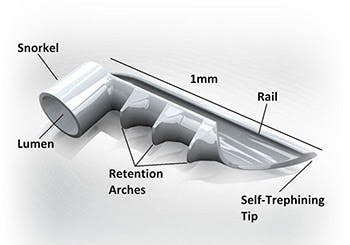
Hydrus Microstent

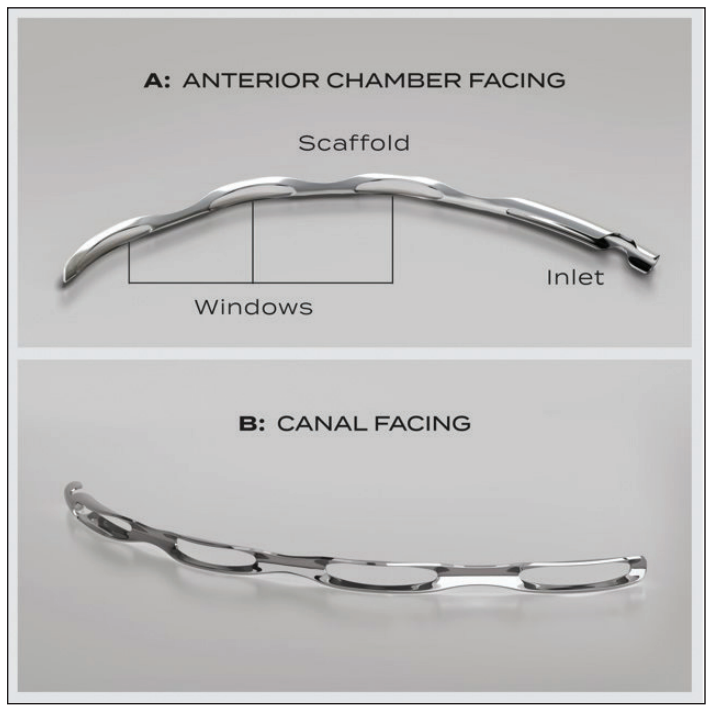

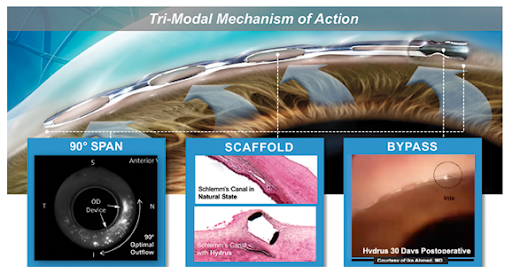
Approved in 2018, the Hydrus is a curved porous stent for mild to moderate open angle glaucoma. The mechanism of action is bypassing the TM and dilation of the Schlemm’s canal over a span of 3 clock hours. Hydrus is made of Nitinol metal alloy, the same material used in cardiac stents which makes it very flexible upon manipulation. It should be used with some caution in patients with nickel allergy.
For dilation of the Schlemm’s canal:
Ab interno canaloplasty (ABiC) with iTrack and Visco 360

This procedure was approved by the FDA in 2018 for mild to moderate glaucoma. ABiC works by injecting viscoelastic into the Schlemm’s canal with the use of an illuminated iTrack catheter to dilate the canal and distal collector channels. It also has the theoretical advantage of breaking micro adhesions in the Schlemm’s canal-collector channel complex as well as flushing the filter TM tissue.
For dilation of Schlemm’s canal and trabecular meshwork removal:
The following devices facilitate aqueous flow by dilating the collector channels in addition to incising the TM for direct access of aqueous to the outer wall of Schlemm’s canal and the collector system.
OMNI

Approved in 2017, OMNI was introduced as a single device with a dual mechanism of action to facilitate a tissue-sparing and implant-free procedure that could be performed as either stand-alone or in combination with cataract surgery.
For shunting aqueous into the subconjunctival space:
This group works by allowing access of aqueous fluid into the subconjunctival space.
Xen Gel Stent
This 6-mm long Xen gel stent was approved in 2016 and is made of Porcine gelatin. Mitomycin C (MMC) is used to increase the survival of the bleb. Being more effective compared to other MIGS procedures, Xen Gel stent can be used to treat moderate to severe forms of glaucoma, such as pseudoexfoliation and pigmentary which have been unresponsive to other procedures.
The value of learning more than one MIGS procedure
There are multiple factors in glaucoma patient care that should be kept in mind when choosing a MIGS procedure, including the patient’s needs, stage of disease, angle anatomy, ability to perform stand-alone versus combining with cataract surgery, patient’s insurance, and hospital or surgery center availability.
Patients who are not able to stop their anticoagulants/antiplatelet medications and/or require a faster recovery might be a good candidate for a stent procedure (iStent Inject W or Hydrus) or an angle procedure with lower risk of bleeding, such as canaloplasty with viscodilation only (ABiC). Pseudophakic glaucoma patients are only able to benefit from options which are approved for stand-alone use.
In some patents, their insurance company might only cover certain procedures, and this can limit you if the patient will only allow what is covered by insurance. However, note that if there is a particular type of glaucoma surgery you strongly recommend that is not covered by insurance, consider letting the patient know, in case they want to pay out of pocket. Also, some surgery centers might not have the equipment or technology like Trabectome, which makes a single use device such as KDB, OMNI or TrabEx+ a more reasonable option.
For these reasons listed above, it is my opinion that every MIGS surgeon should learn at least one MIGS procedure in each of the various mechanisms of action: goniotomy, canaloplasty, and stents. If you practice glaucoma more intensely, learning subconjunctival stenting (Xen) is also strongly recommended. In this way of learning multiple MIGS, you have an advantage with procedures combined with cataracts, as stand-alone, in early to moderate or even severe glaucoma cases to serve your glaucoma patients individually.
Deciding on which procedure works best
By reviewing the previous studies in more detail, we can see that most of the MIGS procedures are similar in terms of IOP-lowering effect and reduction in number of glaucoma medications when performed on the right candidate. So how do you choose?
Figuring out device to select
It is important in a preoperative conversation with your patient to set realistic expectations. This applies to glaucoma surgeons too. We should keep in mind that MIGS procedures will be able to decrease IOP by 20-30% and/or reduce one glaucoma drop, so if a patient needs a higher degree of IOP lowering or has high IOP despite being on maximally tolerated medical treatment (MTMT), MIGS might not be the right answer unless there is nerve reserve.
Nerve reserve means that the patient still has ample nerve tissue to work with and a CDR of 0.8 or below, which is typically mild to moderate glaucoma. When the IOP is uncontrolled, the CDR is 0.9, the patient is on MTMT, and visual fields and OCT show significant loss, one may want to consider a subconjunctival based stent (Xen) or a traditional glaucoma surgery (trabeculectomy or tube shunt) first to really aim for a low target and reducing medications for long term benefit.
Some other important aspects of selecting a device first have to do with the familiarity and comfort level of the surgeon. Once you decide to add a MIGS device to your surgical armamentarium, it usually takes 10 cases for one device to become certified and about 30+ to master it. It is also helpful to review your surgical outcomes to be able to know what to confidently expect with the device and in which patients. Even if you do not have the opportunity to train on MIGS in your residency or fellowship training, the good news is that with company support and experienced surgical trainers, you can continue learning and mastering MIGS well out of your training.
Identifying the ideal patient for MIGS
A patient with open angle on gonioscopy, good nerve fiber layer reserve, early-to-moderate glaucoma, and who is on one to three eye drops is the best candidate for MIGS. The goal would be to achieve a 20-30% reduction in IOP or mid-teen IOP and/or decrease the number of glaucoma medications.
Good MIGS candidates can also have narrow angles, as they can open with cataract removal or combining with goniosynechialysis. They can also be high or normal tension glaucoma patients.
A less than ideal candidate is a glaucoma patient with severe OAG on MTMT, heavy synechial angle closure (uveitis or chronic angle closure glaucoma), neovascular glaucoma, congenital anomalies (e.g., Axenfled-Reiger), or severe corneal opacity. Note, although less than ideal, there are some MIGS procedures that can work well for synechial angle closure.
Using clinical exam findings to choose the right MIGS device
There are clinical findings that help us choose the right procedure for the patient. These include number of medications, preoperative IOP, stage of glaucoma (cup-to-disc ratio), visual field, and OCT. Also consider the presence of secondary characteristics, like pigment dispersion or pseudoexfoliation and status of the lens (e.g., cataract versus pseudophakia).
For early to moderate glaucoma, TM removal (Trabectome, KDB, GATT), TM bypass (iStent Inject W, Hydrus), viscocanalostomy (ABIC with iTrack), or a combination procedure (OMNI) all work well. For moderate to advanced glaucoma, TM removal, viscodilation (ABIC with iTrack), or a combination procedure (OMNI), or Xen Gel stent are more suitable options, whether as stand alone or in conjunction with cataract surgery.
Both open or closed angle could be treated with TM removal procedures or Xen stent, but bypassing, viscodilation, or combination procedures are only approved for open angle glaucoma.
All MIGS procedures could be used as standalone, except for iStent Inject W and Hydrus, which is indicated by FDA to be combined with cataract extraction.
Previous laser trabeculoplasty results can serve as important information, as a successful history might be an indicator that the post-TM pathway is functional, and an angle-based procedure might be the right choice. On the other hand, multiple laser trabeculoplasty treatments might cause PAS formation or scarring within the lumen of Schlemm’s canal and this patient might not be a good candidate for canaloplasty.
Chronic stable uveitis cases might be amenable to MIGS and it has been shown that goniotomy procedures such as Trabectome, KDB, and GATT work well in these cases.
Antiplatelets (Aspirin, Plavix, etc) or anticoagulants (Warfarin) could result in significant intraoperative bleeding; if possible, these agents should be stopped prior to surgery. Consulting with a primary care physician or cardiologist in these cases is recommended. History of easy bruising may also be an indicator of more severe bleeding during the procedure. If not able to stop the antiplatelets or anticoagulants, performing a stenting procedure or canaloplasty might be safer compared to goniotomy procedures.
My personal preference of choosing MIGS
For narrow angle with or without presence of PAS:
In these patients, MIGS options are limited to goniotomy with a hand piece (Trabectome, KDB, TrabEx +/-), combined with cataract extraction if phakic and stand-alone if pseudophakic. With these procedures, the glaucoma surgeon has the ability to break peripheral anterior synechia (PAS) if present by performing goniosynechialysis with the tip of the device exposing the TM for incision.
I avoid the use of stents, as they may not be safe for the corneal endothelium in these narrow angle patients. I also avoid viscodilation as the anatomy may not allow for smooth catheterization of the canal.
For mild POAG/OHTN with cataracts:
With the consideration of leaving the trabecular meshwork and outflow system intact, but being able to expand outflow and lower IOP, viscodilation is a great option for early glaucoma. iStent Inject W and Hydrus are also procedures that have a higher safety profile, justifying their use in patients with no to minimal glaucomatous damage. I tend to use iStent Inject W for POAG /OHTN patients controlled on one or two meds. With Hydrus, I tend to use this for controlled mild POAG patients on two-three meds OR moderate POAG controlled on one-two meds. I could also consider goniotomy or canaloplasty for this latter category as well.
For pseudoexfoliation:
My go-to procedure after SLT has failed to control IOP is goniotomy, which has multiple options (Trabectome, KDB, TrabEx+, GATT, OMNI).
For uncontrolled glaucoma on three + medications:
Consider GATT, ABIC with iTrack or OMNI if phacoemulsification is uneventful, normal angle anatomy, and absence of severe disease (MD>15). Other goniotomy procedures such as Trabectome, KDB, and TrabEx+ are reasonable options in early to moderate disease. I consider Xen if angle anatomy is favorable, moderate to severe glaucoma, patient not able to tolerate many eye drops and/or maxed on drops, and lifestyle is compatible with having a bleb in the eye.
Consider combined phacoemulsification with Hydrus or goniotomy and leave Xen as back up if the first combined procedure fails. Data shows combined phacoemulsification with Xen is not as successful as standalone Xen.
For patients on antiplatelets/anticoagulants that cannot come off or who easily bruise:
iStent/Hydrus or canaloplasty (ABiC).
Controlled mild to moderate glaucoma on one-three medications:
Stents (Hydrus, iStent), canaloplasty (ABiC), goniotomy or combination with OMNI .
Controlled severe glaucoma on one-three medications:
Goniotomy (Trabectome, KDB, TrabEx), canaloplasty (ABIC), combination with OMNI, or Xen.
For patients with a prior history of glaucoma drainage devices:
Ciliary body ablations such as transscleral cyclophotocoagulation (e.g., CPC MP3) or endoscopic cyclophotocoagulation.
Putting it all together
These are some key tips to summarize choosing the right MIGS with action steps.
1. Start learning about new MIGS techniques/procedures
- Master the goniotomy, as this is the most versatile group.
- The more procedures you master, the more choices you will have.
- Take time for MIGS mastery—you need to perform at least 30 cases.
- Set a goal of mastering one to two MIGS per year, taking at least 6 months to focus on one.
2. Start looking for ideal patients for each MIGS procedure
- Set the right expectations and goals for you and your patient.
- Use the tips we mentioned above.
- Review your results to find out which MIGS has better outcomes in your hands.
3. Check out these additional resources
The Building Blocks of Trabectome Surgery (Kugler publications; ISBN-10: 9062992536, ISBN-13: 978-9062992539) authored by Dr. Constance Okeke is an excellent resource to learn more information about MIGS in general and Trabectome specifically.
Also, the iGlaucoma YouTube channel (iGlaucoma - YouTube) is another resource that could be utilized to master MIGS with instructional videos.
Check up the upcoming video series called MIGS Success Surgical Secrets:
- MIGS Success Surgical Secrets Video Series Trailer - A Must See for MIGS Glaucoma Surgeons!
- and the video on mastering surgical gonioscopy for MIGS: 5 Key Steps to Mastering Surgical Gonioscopy in MIGS
