





WHAT YOU'LL LEARN
Which ocular conditions commonly masquerade as glaucoma
How to identify glaucoma masqueraders in practice
Introducion
Introduction
It is important to see the bigger picture when evaluating and diagnosing a patient as there are many ocular conditions that can masquerade as glaucoma. By evaluating a comprehensive medical history, case history, and utilizing different multimodal ophthalmic imaging, we will be better equipped to diagnose and manage our patients accordingly. This article will walk through different cases to construct a thought process with which to tackle these diseases.
Case 1
Case 1
- 57 yo BF referred by PCP for glaucoma evaluation.
- POHx: Latanoprost qhs OU, poor compliance. Pt self discontinued since “she did not feel it was helping”.
- MHx: HIV (+), unknown viral load
- BCVA: 20/40 OD/OS
- Pupils: PERRL (+) Grade 2 RAPD OS
- IOP: 19/20
- PACHY OD: 530, OS: 534
- Gonioscopy: Open (-) neovascularization of the angle, angle recession, peripheral anterior synechiae
- Additional findings: Anterior Uveitis OS; asymptomatic. Tritan color vision defect, OS

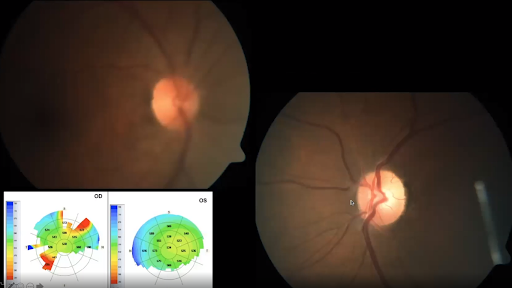
Figure 1.0: Fundus photos (blur due to cataract) and pachymetry (OD 533um, OS 534um)

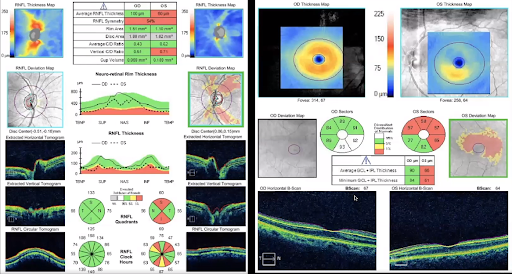
Figure 1.1: Left: OCT RNFL - notice the asymmetry between the RNFL layer of the eyes. Right: Ganglion Cell Analysis - OS shows asymmetry between the superior and inferior portion, respecting the horizontal raphe.

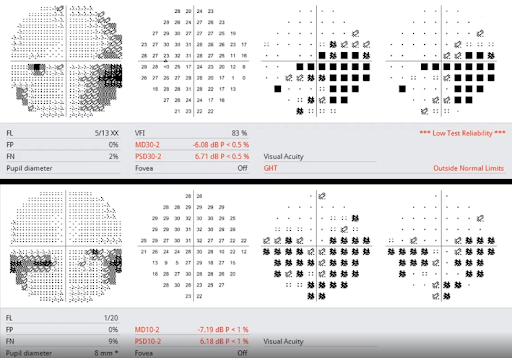
Figure 1.2: Top: 30-2 SITA, OS - dense inferior arcuate defect, and superior nasal step. Bottom: 10-2 SITA, OS - corresponds well with the ganglion cell loss as seen in Figure 1.2. Note: OD visual field not shown, but full without glaucomatous defects.
Conclusion: Still in the gray area, and glaucoma should be put on the differential list. The patient has some outlying data: asymmetry and APD that warrant a closer look at imaging.

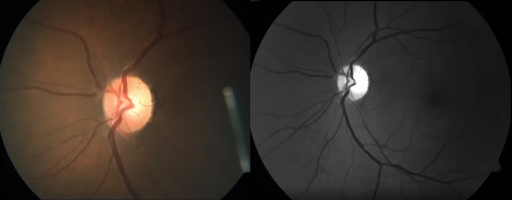
Figure 1.3 Left: Fundus photography, OS. Right: Red-free fundus photography OS - distinct pallor temporal.
Case 1 Discussion
The patient was diagnosed with neurosyphilis. Remember that if you have a puzzling diagnosis that does not look quite right, consider blood work, as well as, neurosyphilis. The ocular manifestations of neurosyphilis are quite diverse:
- Interstitial keratitis
- Episcleritis
- Papillary conjunctivitis
- Granulomatous or non-granulomatous uveitis
- Chorioretinitis
- Retinitis
- Vitritis
- Multifocal choroiditis
- Neuro-retinitis
- Papilledema
- Optic atrophy
- Ocular hypertension
- Argyll-Robertson pupil
- Cranial nerve palsies
Case 2
Case 2
- 52 yo WM
- BCVA: 20/25 OD, 20/20 OS
- Pupils: PERRL (-) RAPD
- IOP: 18/19, Pachymetry: 560/553
- MHx: unremarkable, + smoking (cigarettes)

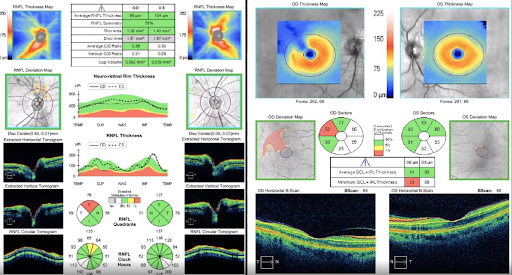
Figure 2.0: OCT RNFL and ganglion cell analysis. Notice the asymmetry in the RNFL thickness from OD to OS.

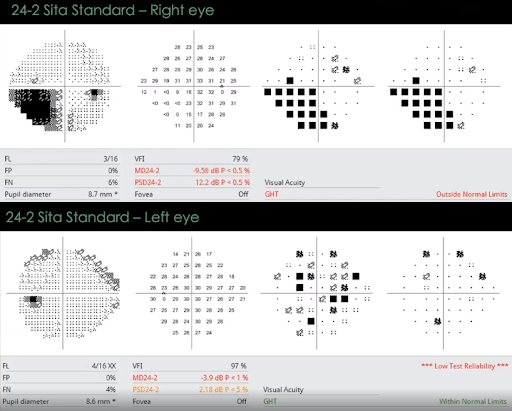
Figure 2.1: VF 24-2 absolute defect inferior nasal, OD. Recall that glaucoma starts as a relative defect.

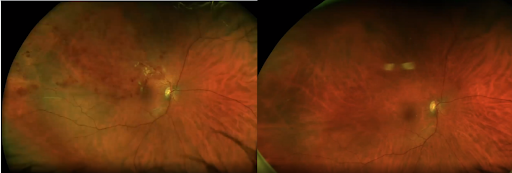
Figure 2.2: Before and after resolution of BRVO.
Case 2 Discussion
This patient had a branch retinal vein occlusion (BRVO) of the right eye. The occlusion starts very close to the optic nerve head (Figure 2.2), and branches off to the peripheral retina with damage to capillary beds as seen by the deeper hemorrhages. Due to the size and extent of damage, there’s been a lot of retinal ischemia.
Cases like this one can be glaucoma masqueraders when the patient walks into your office after resolution of the condition. You want to be able to pick up a history of retinal vein occlusion so the patient doesn’t get misdiagnosed with a different condition. With careful analysis of the fundus photo post-resolution, you can see the arterials were attenuated. A fundus autofluorescence image (Figure 2.3) also makes the tiny collateral vessels pop out. It is important to use different imaging techniques to assess the overall picture, and to evaluate from quadrant to quadrant to pick up on subtle signs.

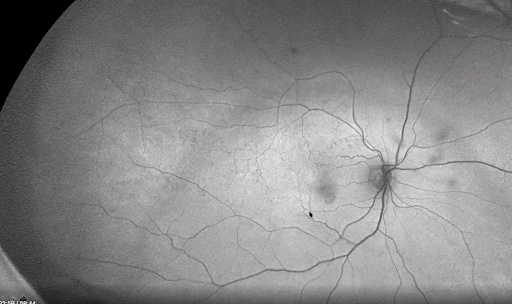
Figure 2.3: Fundus autofluorescence, OD. Cursor is pointed at collateral vessels.

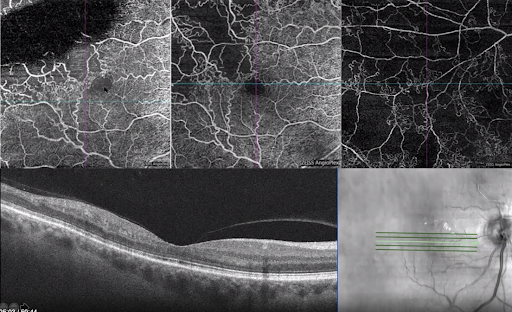
Figure 2.4: OCT angiography, OD. Top left: 3 day presentation after RVO. The black area denotes swelling of the retina. You can see collateralization near the macula to drain and perfuse the retina. And identify that there are at least 5 disc diameters of capillary dropout (clinical sign of BRVO). Top middle: 2 months after the initial presentation. Note the capillary dropout. Top right: Along the superior arcade. Although there is no capillary bed there, notice the microvascular changes.
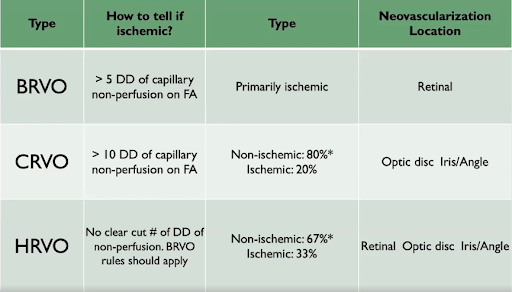
Recall that the average patient with vein occlusions is over 50 years of age. BRVO does not come from the same etiology as a CRVO or an HRVO. BRVOs are primarily ischemic and retinal. CRVO will affect the optic disc, iris, and angle, and will present with different sizes of capillary non-perfusion. This table will help outline the difference between the three types:

This patient was diagnosed with ischemic BRVO with macular edema. The patient was young at 52 years of age. If a patient doesn’t fit the norm for vein occlusion (older, hypertensive, diabetic, hyperlipidemia), make sure to think of differential diagnosis. Blood work is important to order to rule out an infectious nature, and throw syphilis as mentioned in case #1 as a possible outlier.
In the last couple of years, literature advises to check homocysteine levels. Increased homocysteine promotes arteriosclerosis which leads to thrombosis. The etiology of vein occlusions is thrombosis. Patients with elevated homocysteine levels have a higher change of cerebral vascular problems, peripheral vascular disease, and 5x increased risk of stroke. This patient’s blood work showed normal results overall, besides homocysteine and cholesterol levels being elevated. If these levels are caught early, they can be easily treated with topical supplementation. For vein occlusions, it is important to evaluate for homocysteine levels in blood work.
This patient was managed with oral folic acid to normalize his homocysteine levels. He was also treated with 2 avastin injections over a three month period.
Case 3
Case 3
- 52 yo, BM comes in for a second opinion.
- POHx: Glaucoma (dx 2016)
- Medications: Latanoprost qhs OU, Cosopt bid OS, Brimonidine 0.15% tid OU
- Surgery: s/p laser procedure OS, 1 yr ago
- Tmax: unknown
- PMHx: situs inversus
- FOHx: glaucoma - brother
- BCVA: OD 20/20, OS 20/25
- Pupils: PERRLA, + RAPD OS grade 3
- IOP: 12 mmHg OU
- Pachymetry: 494 OD, 490 OS

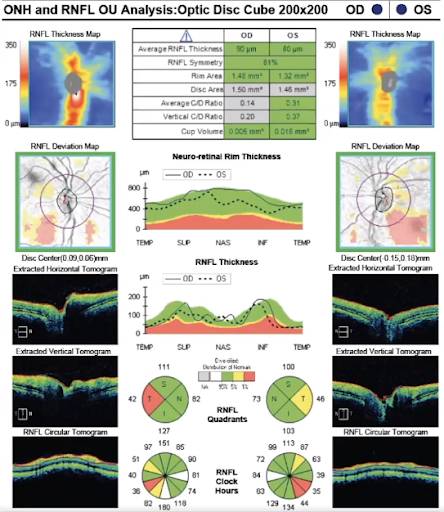
Figure 3.1: OCT RNFL - fairly symmetric RNFL within 10um. The temporal quadrants on each eye are flagged, but fairly symmetric. One of the ways to pick up whether a patient has situs inversus is to analyze their RNFL thickness. Note that the two peaks move a little nasal.

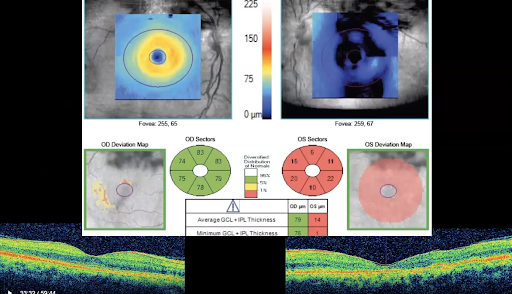
Figure 3.2: GCC analysis. There is a large difference between the eyes. Before thinking that the patient has such a severe dropout in OS, keep in mind the limitations of the scan. A ganglion cell analysis is looking at the internal limiting membrane and ganglion cells. The ILM is 50um, so if you notice numbers that fall below this value, it means that the segmentation is wrong. Note also the difference between the outer retinal layer of OD vs OS.

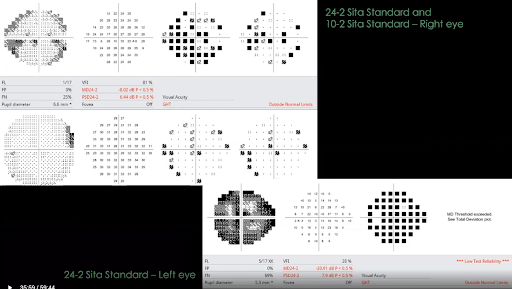
Figure 3.3: Visual field reports. A 24-2 and 10-2 were performed on OD due to a central depressed point. However, the fields were unreliable for both eyes.
Case 3 Discussion
This is not glaucoma due to many factors. There are abnormalities in different areas that do not coincide with glaucomatous damage. The patient is on 4 different medications, and has had some kind of retinal procedure. It is possible to start over with this patient’s medical treatment and see if changes occur due to glaucoma. If not, it opens the door to other options. We can go back over different scans done with this patient and dive a little deeper.

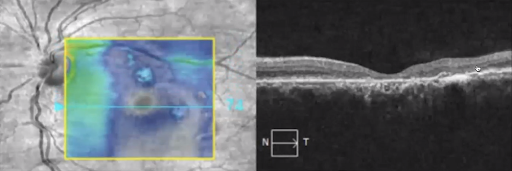
Figure 3.4: Fundus photo and OCT macula, OS. Note the outer pigment epithelial detachments and atrophy. (full scan of the OCT macula indicates more PED’s) .

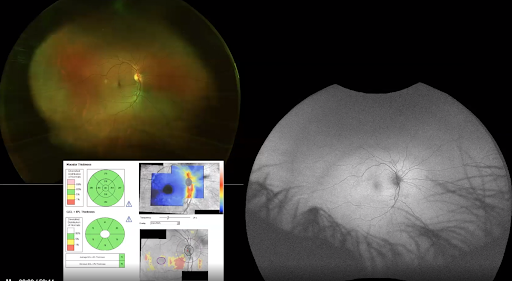
Figure 3.5: Fundus photo, OD. Note tilt of the optic nerve, and inferior vessels coming out on the nasal side.
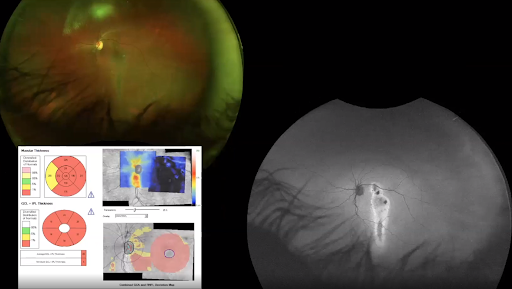
Figure 3.6: Fundus photo, OS. With fundus autofluorescence, the extent of damage on the macula is visibly highlighted.
This patient has chronic central serous chorioretinopathy. This correlates with the PED’s seen in the OCT macula. At some point in his life, he had large serous detachments. The descending drip occurs because gravity pulls the fluid down. The filtered image will show stressed areas as hyperfluorescence, and the darker spots as areas where the RPE is no longer functioning (Figure 3.6).
This patient still needs to be evaluated for glaucoma vs ocular hypertension. You can do a medication holiday and reevaluate periodically. This particular patient’s IOP went back up to 28 and 24, which is great to establish Tmax. Instead of having him on three different drops, we can start with one and periodically monitor pressure elevations.

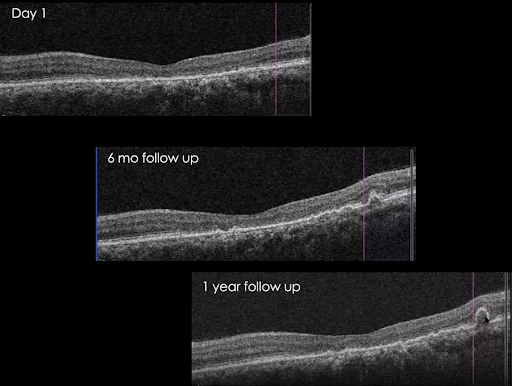
Figure 3.7: OCT slice, OS showing variation over time. Note how the disease changes with the PEDs even though there is no active serous detachment.

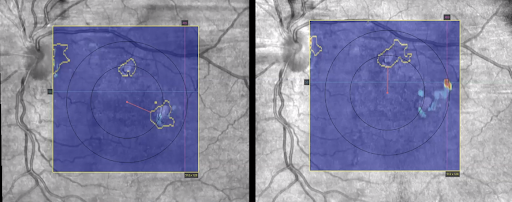
Figure 3.8: Advanced RPE analysis, OS. On the right image, the orange pigmented spot denotes the PED. The outlined spots in yellow indicate subretinal or choroidal illumination - areas of geographical atrophy. Recall that the patient had laser treatment in his OS, which points towards retinal laser instead of SLT that may have been thought of on initial discussion. This scan is great for AMD patients to monitor for changes in disease over time.
Central serous chorioretinopathy, “sick RPE syndrome”, is associated with increased permeability of the choroid resulting in PED and serous retinal detachments. This condition is mostly seen in Type A young males. OCT will show an increased choroidal thickness (normal average is 270um vs 405um seen in CSR).
Case 4
Case 4
- 52 yo, AF, diagnosed with POAG, moderate stage, OU for 14 years
- Medications: Cosopt bid OU, Brimonidine bid OD
- Tmax: 26, 24
- Pachymetry: 528 OD, 519 OS
- POHx: degenerative myopia OU, lattice degeneration OU, pigmented atrophic hole OD
- MHx: unremarkable
Note: there is a higher risk of glaucoma in degenerative myopic patients. It is also harder to examine their optic nerves and cupping because of the tilts.

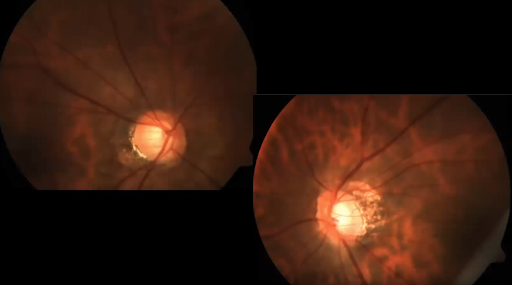
Figure 4.1: Optic nerve photos. Note the oblique/tilted insertion, and PPA. The cups look fairly symmetric.

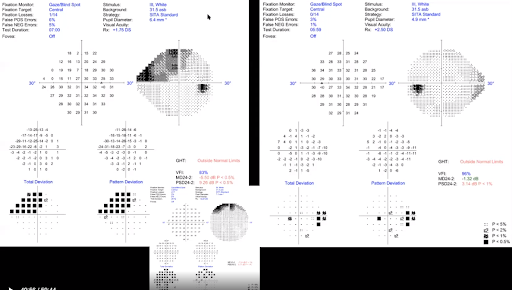
Figure 4.2: Visual fields. Top left: superior defect in OD (not as dense compared to the BRVO in Case 2). Bottom: 10-2 also indicates a superior defect., which classifies it as a severe stage. Right: OS, peripheral visual field defect inferior and superior nasal.

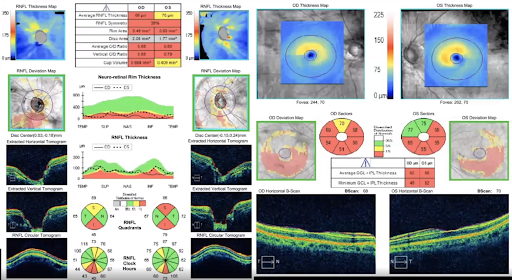
Figure 4.3: OCT and ganglion cell analysis. There is symmetry in reduction of the RNFL thickness OU that points more towards glaucoma. There is asymmetry in cupping as seen on the RNFL thickness map, but remember that the insertion is not the same for this degenerative myope.
Note: The normal database for OCT scans goes up to -6.00D. This patient has a refractive error of -10.00D. So the red indicators just means that the patient does not fit the normative database.

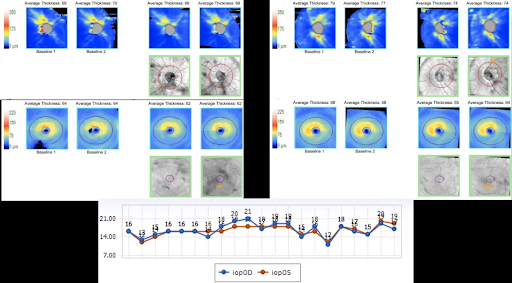
Figure 4.4: Comparative scans over a ten year span. The top images are nerve fiber layer thickness, and bottom shows the ganglion cell analysis.
Case 4 Discussion
Figure 4.4 shows lack of change over the course of 10 years. This patient did have elevated eye pressure, but it could just be ocular hypertension. Let’s analyze her defects a little further:

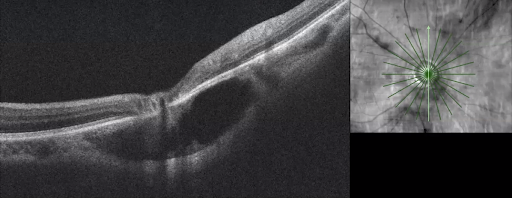
Figure 4.5: Fundus autofluorescence, OD with radial raster. Note the large cavitation right below the optic nerve head.

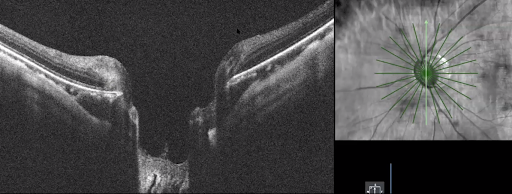
Figure 4.6: Fundus autofluorescence, OS. There is a superior and inferior cavitation present.
This condition is called peripapillary choroidal cavitation. Looking back at figure 4.3, the right eye tomogram in the middle picks up the cavitation. The OCT images also show a vast inferior thinning of the right eye corresponding with the large cavitation. In the left eye, there were also signs of superior and inferior nasal steps that correspond with the smaller cavitations (figure 4.2).
Peripapillary choroidal cavitation is generally found in high myopes (average -9.00D, 27.36mm axial length). In 60% of cases, there will be a yellow-orange peripapillary lesion. About 70% of patients present with glaucomatous appearing visual field losses. Glaucoma is a progressive optic neuropathy. Cavitations are not. It is important to monitor these patients and see if there is any progression in her IOP, visual field, OCT scans etc.
Conclusion
Conclusion
There are countless glaucoma masqueraders, but with advanced imaging and diagnostics many of these mimics can be distinguished and diagnosed accordingly. It’s absolutely crucial to supplement diagnostic imaging with comprehensive patient history for accurate diagnosis and appropriate treatment—key elements in delivering excellent patient care.
