


WHAT YOU'LL LEARN
Understand the pathophysiology of glaucoma
Know the options for glaucoma management
Learn what testing must be done to deliver a diagnosis
Know the guidelines for setting treatment goals
Tips for improving patient compliance
Introduction to glaucoma management
The glaucomas are a class of ocular disease characterized by progressive optic nerve degeneration with subsequent loss in retinal nerve fiber layer (RNFL) and retinal ganglion cells (RGCs). It is the leading cause of irreversible blindness worldwide, affecting over 60 million people. As primary eyecare providers on the front lines of ocular disease management, it is important for us to have an arsenal of management strategies at our disposal. By having a thorough understanding of glaucoma’s pathophysiology and various treatment options, we are able to provide better education and treatment options for our patients. In this course we will dive a bit deeper into addressing a patient’s risk factors and specifically tailoring their treatment plan.
At this time, there is no definitive cure for glaucoma; however, when caught early in the disease process, most practitioners are able to preserve their patients’ vision and quality of life. Currently, the reduction of intraocular pressure (IOP) is the only evidence-based treatment for glaucoma.
The primary care optometrist will likely encounter two common types of glaucoma, either primary open angle glaucoma (POAG), or normal tension glaucoma (NTG). More rare are cases of acute angle closure glaucoma (AACG) and neovascular glaucoma (NVG).
Pathophysiology
POAG pathogenesis is primarily thought to be caused from elevated eye pressure or ocular ischemia, while NTG pathogenesis is more likely attributed to ocular ischemia. Several causes of ocular ischemia are nocturnal hypotension, metabolic/ cardiovascular disease, and sleep apnea. For these reasons it is important to assess a patient’s vasculopathic risk factors and treat/educate accordingly. While some practitioners continue to refute the link between diabetes and glaucoma,2-14 the American Academy of Ophthalmology agrees that type 2 diabetes is a risk factor for POAG.1 Some commonly used POAG risk calculators are now even including diabetes into their calculations for risk of developing glaucoma.28

AACG occurs when patients with narrow anterior chamber angles (eg. hyperopes or advanced cataracts) have transient or permanent occlusion of the angle causing a rapid spike in IOP and subsequent irreversible optic nerve damage (over hours to days). It is best to refer patients with narrow angles for laser peripheral iridotomy and/or cataract surgery if you feel they are at risk for angle closure (to prevent an acute episode and permanent vision loss). Patients with untreated or recurring uveitis/iritis are also at risk for AACG due to the formation of anterior or posterior synechiae.
NVG occurs when the anterior chamber angle is partially or completely occluded from the abnormal formation of blood vessels within the angle (eg. vein occlusions or uncontrolled metabolic disease).
Glaucoma (POAG/NTG) is often a slow, painless, progressive disease that takes place over years to decades. However, some patients who experience acute angle closure or NVG (of any etiology) will often complain of severe ocular pain, increased pressure, photophobia, and hazy/cloudy vision.

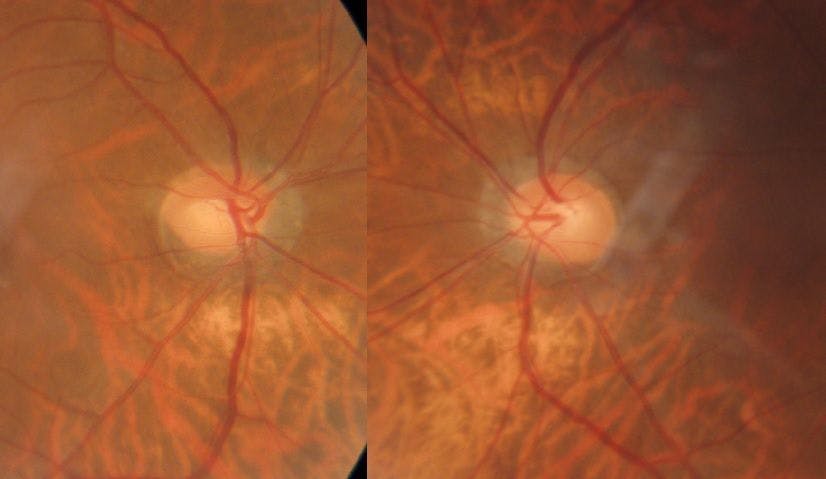
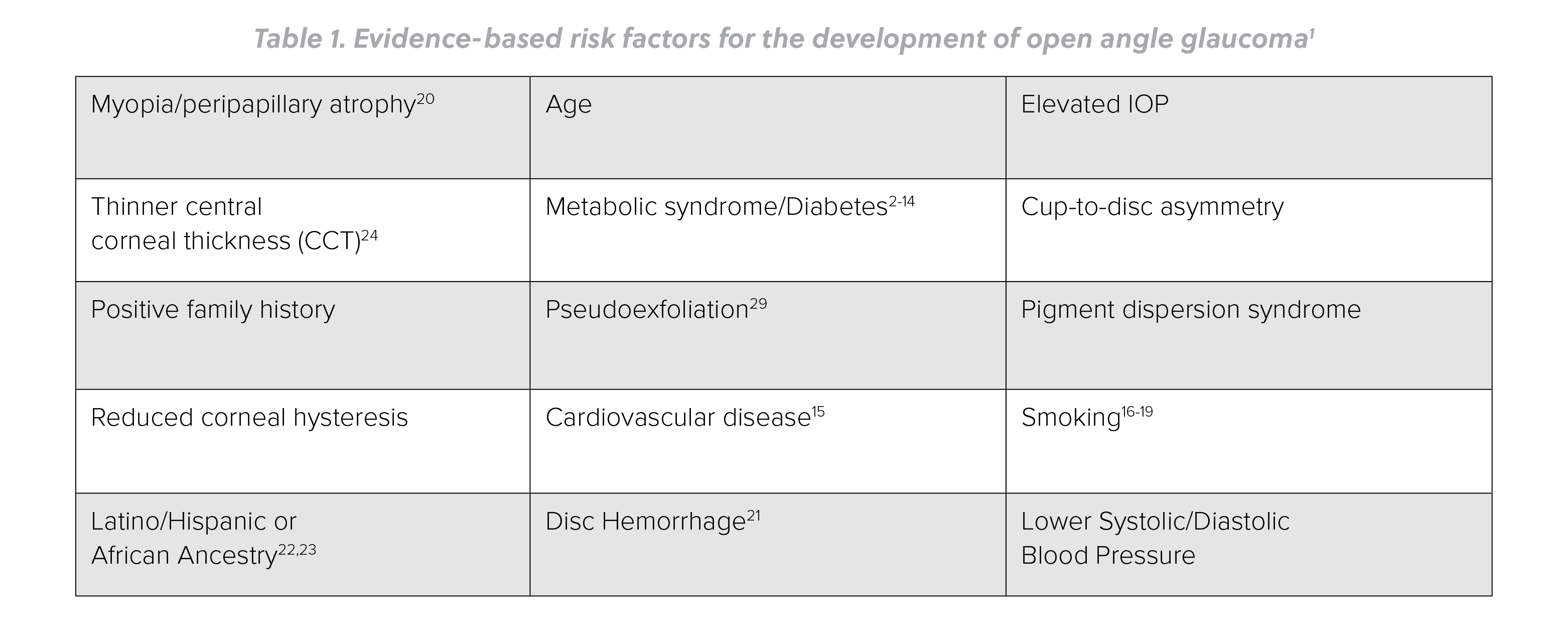
Figure 1: Peripapillary atrophy and high myopia are considered risk factors for developing glaucoma.20

Figure 2: Nerve fiber hemorrhages at the optic disc, aka “drance hemes” are also pathognomonic for glaucoma. These can predict areas of impending nerve fiber damage, subsequent erosion of the neuroretinal rim, and are also considered a strong risk factor for POAG progression.21
TIP: Take advantage each time you have your patient in your office to examine the disc for drance hemorrhages. If found, this will be a red flag of an area to watch more closely in the future for rim erosion, whether through thinning of the rim on clinical exam, wedge defects seen on fundus photography, RNFL thinning on OCT or eventually visual field loss.
Another emerging field in the research of glaucoma pathophysiology is investigating the relationship between intraocular pressure (IOP) and intracranial pressure (ICP). While first described in the early 1970s, this theory suggests that changes in ICP, relative to IOP, creates a difference in trans-lamina cribrosa pressure (leading to optic nerve cupping). In other words, if IOP is greater than the retrolaminar pressure (ICP), this pressure difference could result in glaucomatous optic neuropathy.25, 26 There is also an age related decline in ICP which may partially explain glaucoma being more prevalent in older populations.27
The relationship between IOP and ICP has also been of great interest as a means of explaining the phenomenon of optic disc swelling and elevated ICP in astronauts. This is referred to as spaceflight-associated neuro-ocular syndrome (SANS). Another example of optic nerve pathology related to intracranial pressure is that seen with cases of idiopathic intracranial hypertension (IIH).
Diagnosing glaucoma
Making a diagnosis
When deciding when to make a diagnosis of glaucoma or initiate treatment based on high risk, there are a number of factors to be accounted for.
- Nerve appearance, specifically vertically elongated cup-to-disc ratios are more suspicious of glaucoma. Now, a nerve can be vertically elongated (especially if the disc is also vertically oval in shape) without being glaucomatous. Examine for notches, early signs of thinning, bared vessels or drance hemorrhages for additional signs of glaucoma.
- A difference in vertical c/d of greater than 0.2 between right and left eye.
- Intraocular pressure.
- Central corneal thickness.
- Visual field results.
- RNFL OCT findings. If documented progression on repeated testing can be proven, your case is much stronger for the patient having glaucoma.
According to the Ocular Hypertension Treatment Study (OHTS), central corneal thickness (CCT) plays a significant role in determining a patient’s true IOP. According to OHTS, physiologically thinner corneas, typically those less than 545- 550 micrometers, are an independent risk factor for developing glaucoma.24

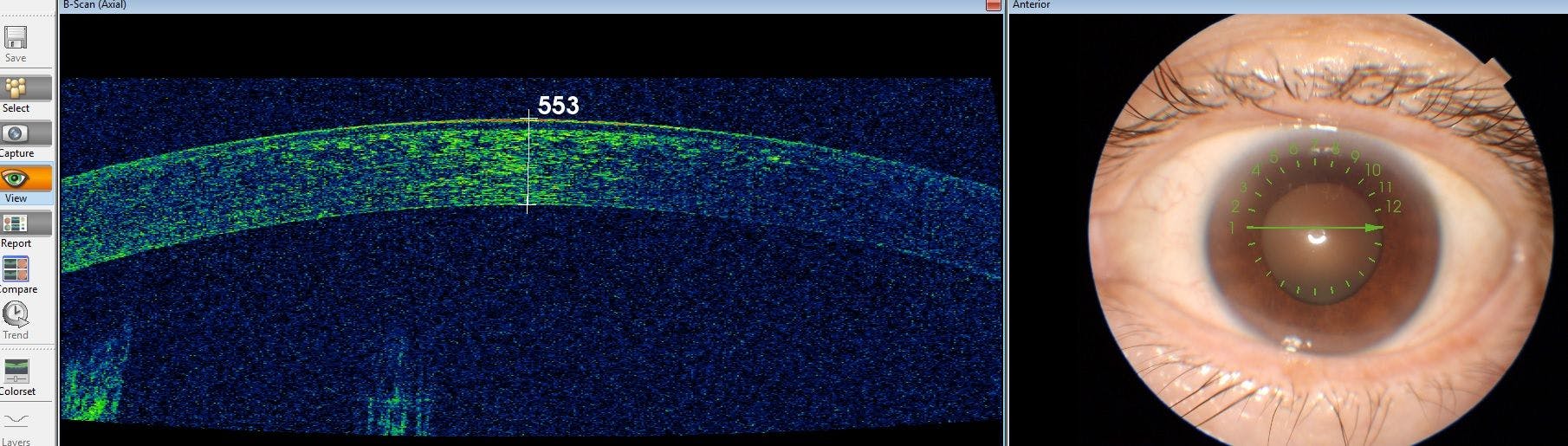
Figure 3: Most OCT machines today have an anterior segment feature, which allows the practitioner (or ophthalmic technician) to acquire non-invasive pachymetry readings via the drawing tool (billable procedure).
It is also important to remember that POAG/NTG should never be diagnosed based on only one visual field test, one IOP measurement, or one OCT scan. Results from OHTS suggests performing three consecutive, reliable visual field tests prior to definitively saying a patient has glaucomatous field loss.
Careful assessment for pigment dispersion syndrome is also important when determining a patient’s overall risk for developing POAG. The presence of krukenberg spindles – excessive pigment on corneal endothelium, iris transillumination defects (best appreciated viewing undilated iris on retroillumination), and excessive pigment within the angle, noted on gonioscopy, all point to pigment dispersion syndrome and increased risk for elevated IOP.
The presence of pseudoexfoliation is another risk factor for elevated IOP and POAG development and is best assessed with a dilated pupil. Patients with pseudoexfoliation tend to have greater diurnal fluctuations in IOP.29
Patient ethnicity is another factor to consider when deciding to treat. Since the African American population tend to have larger vertical cup-to-disc ratios and thinner CCTs, they may benefit from earlier treatment of ocular HTN vs. patients of other ethnicities.24
Stereoscopic evaluation of the optic nerve head should be the foundation of the glaucoma work-up, since up to 40% of patients with “normal” IOP can have glaucomatous optic neuropathy. This can be VERY difficult to do with monocular, undilated views.

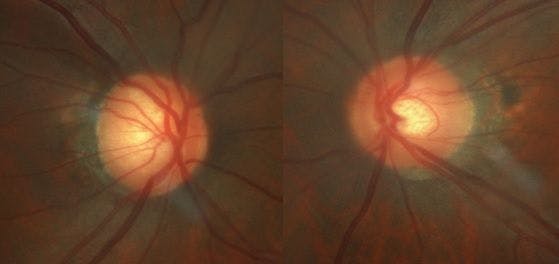
Figure 4: Sometimes shallow cupping can make the neuroretinal rim appear deceptively normal. Utilizing the slit lamp’s red-free filter during biomicroscopy can help practitioners better assess the patient’s rim tissue. Obtaining photos of the fundus/optic nerves can also be a useful tool, providing an alternate perspective. Remember that glaucoma produces the classic erosion/cupping of the rim tissue, while other etiology is usually responsible for pallor/atrophy of the optic disc. Only in advanced stages of POAG will practitioners appreciate a trace pallor of the neuroretinal rim. If disc pallor is present disproportionately to the amount of cupping, it is prudent to shift your work up for non-glaucomatous optic neuropathy, instead of POAG.
Glaucoma management and treatment
Treatment goals: what is “target IOP”?
While every practitioner may have a slightly different approach for glaucoma management, it is important to have one that is evidence-based while also realistic for your individual patient’s lifestyle. Since the reduction of IOP is the only proven treatment for glaucoma, it is important to have some type of criteria to use in determining your goal IOP for that particular patient.
Some practitioners (including glaucoma specialists) will simply say, “I want to achieve an eye pressure that stops the progression of glaucoma.” Others will have a predefined formula, such as “30% reduction from the maximum IOP reading or average of multiple readings.” The name of the game in treating glaucoma is to prevent visual field degradation while also preserving quality of life. Having a goal for the patient’s treated IOP is important and helps the practitioner assess whether or not the current treatment strategy is effective or if it needs to be altered.


Figure 5: In order to establish a target IOP for the patient, it's best to obtain at least three or four untreated IOP readings, preferably with Goldmann tonometry. For patients who strain to comfortably position themselves in our slit lamp, practitioners may obtain more accurate IOP readings from handheld tonometers such as the Perkins model.
While “normal” IOP can range from 10mmHg to 21mmHg,30,31 the higher a patient’s baseline IOP usually equates to a greater risk of glaucoma development. Practitioners must also take into consideration a patient’s CCT in order to truly assess IOP.30,31
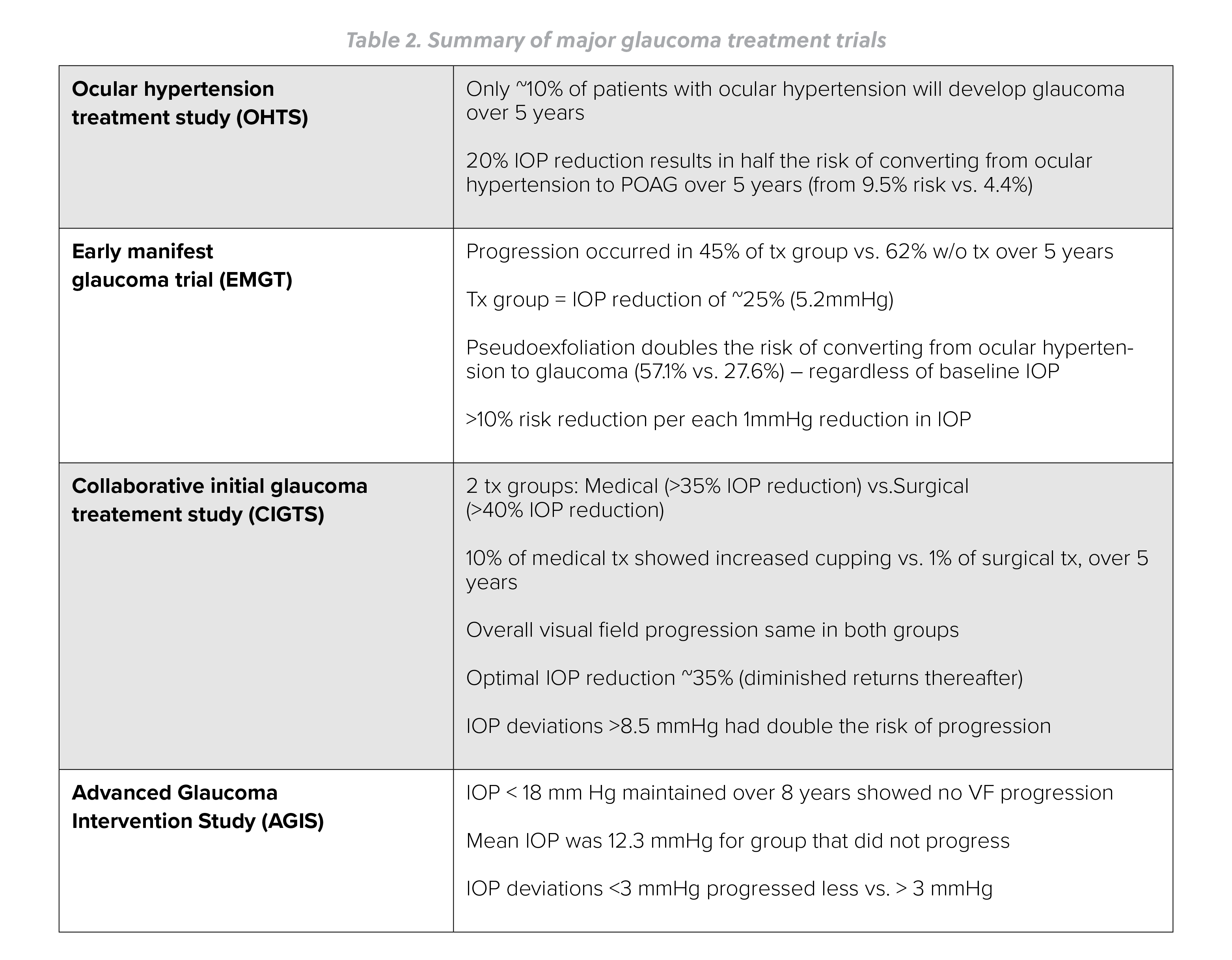
There is no definitive study that says reducing a patient’s IOP by X% is guaranteed to eliminate all risk of progression. There is, however, a multitude of clinical pearls we can take away from the major glaucoma treatment trials.
Preferred practice guidelines from the American Academy of Ophthalmology state that a target IOP reduction of 20% from baseline is recommended for glaucoma suspects.1 The American Optometric Association recommends a 30% to 50% reduction of pre-treatment IOP for managing glaucoma, depending on the patient’s stage/severity and rate of progression.32

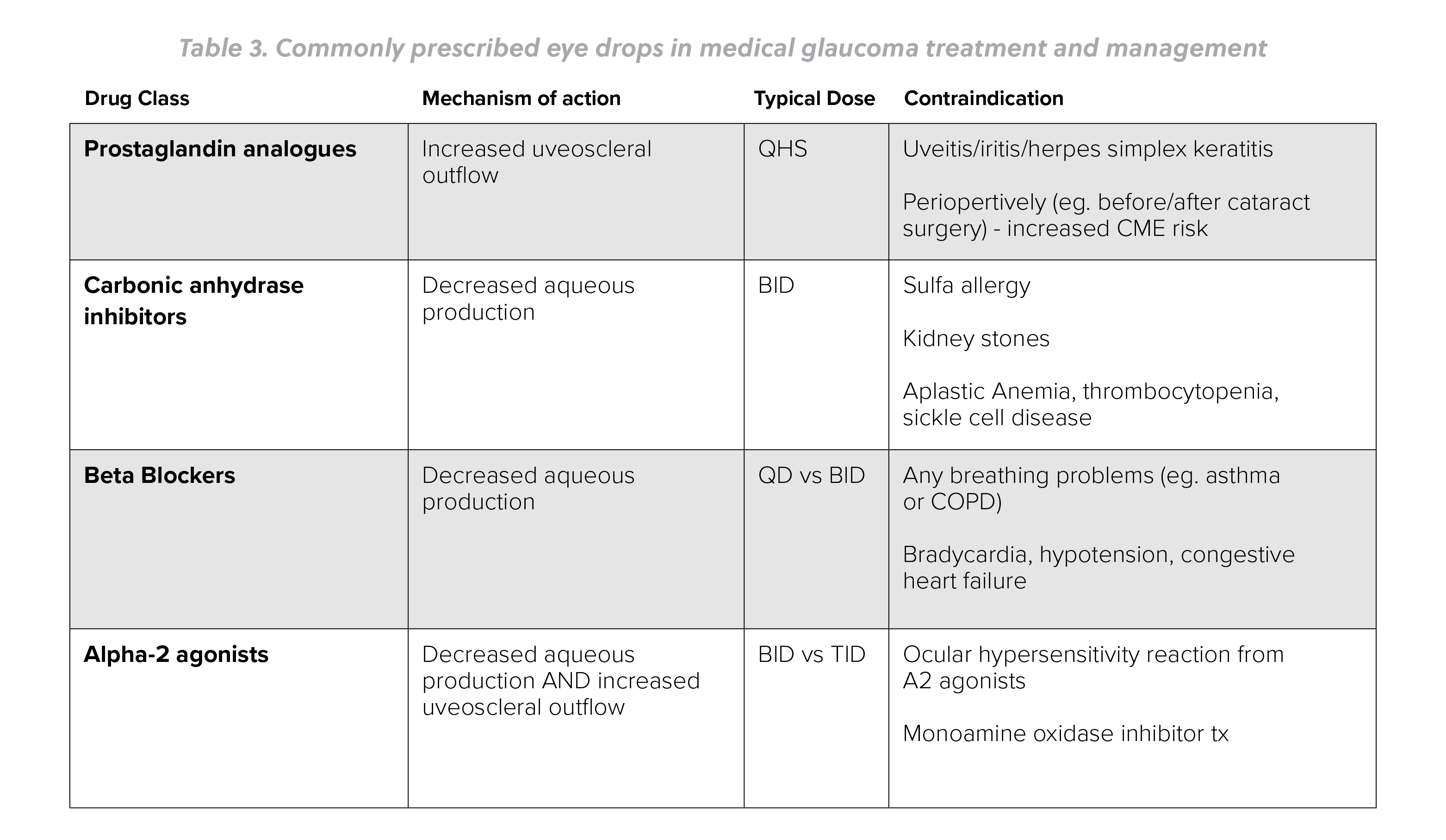
Prostaglandin analogues have been shown to reduce IOP by 28-33%, while beta blockers and carbonic anhydrase inhibitors have a slightly smaller IOP lowering effect of just 15-20%.31

Unfortunately, despite significant IOP reduction, some glaucoma patients will progress while other untreated patients will not.31
Assessing our patient’s other comorbidities and systemic diseases is also important with our glaucoma management plan. Addressing metabolic dysfunction, cardiovascular disease, and smoking cessation can all help restore ocular perfusion and potentially improve treatment outcomes. Referring patients to primary care, behavioral health, and/or nutritionists can also help foster a multidisciplinary approach in the management of glaucoma.
Patients who you suspect may have NTG should have their blood pressure checked in-office. Practitioners working in multidisciplinary settings can also review the EHR for vital signs/BP taken at other encounters. It is important to assess a patient’s risk for nocturnal hypotension. To your surprise, your NTG patient may be on three or four blood pressure medications, some of which are taken in the evening. Some of these patients may achieve adequate blood pressure with less medication or an alternative dosing schedule. It is important to communicate with the patient’s PCP and explain your concern for mitigating risk of pathological nocturnal hypotension, and subsequent glaucoma progression.
Imaging for glaucoma management
Visual field (VF) testing & optical coherence tomography (OCT)
In the initial stages of monitoring patients who you suspect may have glaucoma, obtaining a 24-2 Humphrey VF and OCT scan of the optic nerve/RNFL is a great place to start. If the practitioner is concerned for any paracentral defects involving fixation (eg. compromised ganglion cell count on macular OCT), it is prudent to also perform a 10-2 VF. While most glaucoma patients will initially lose peripheral vision (eg. nasal steps, arcuate scotomas) some patients may actually lose central vision first (eg. paracentral, centrocecal scotoma) due to RNFL loss in the macular vulnerability zone.33 Since 50% of all retinal ganglion cells are within the central eight degrees of fixation, the 10-2 VF is more sensitive at detecting glaucomatous defects involving fixation. The 24-2 VF spaces test points six degrees apart, while 10-2 VF testing spaces points only two degrees apart.

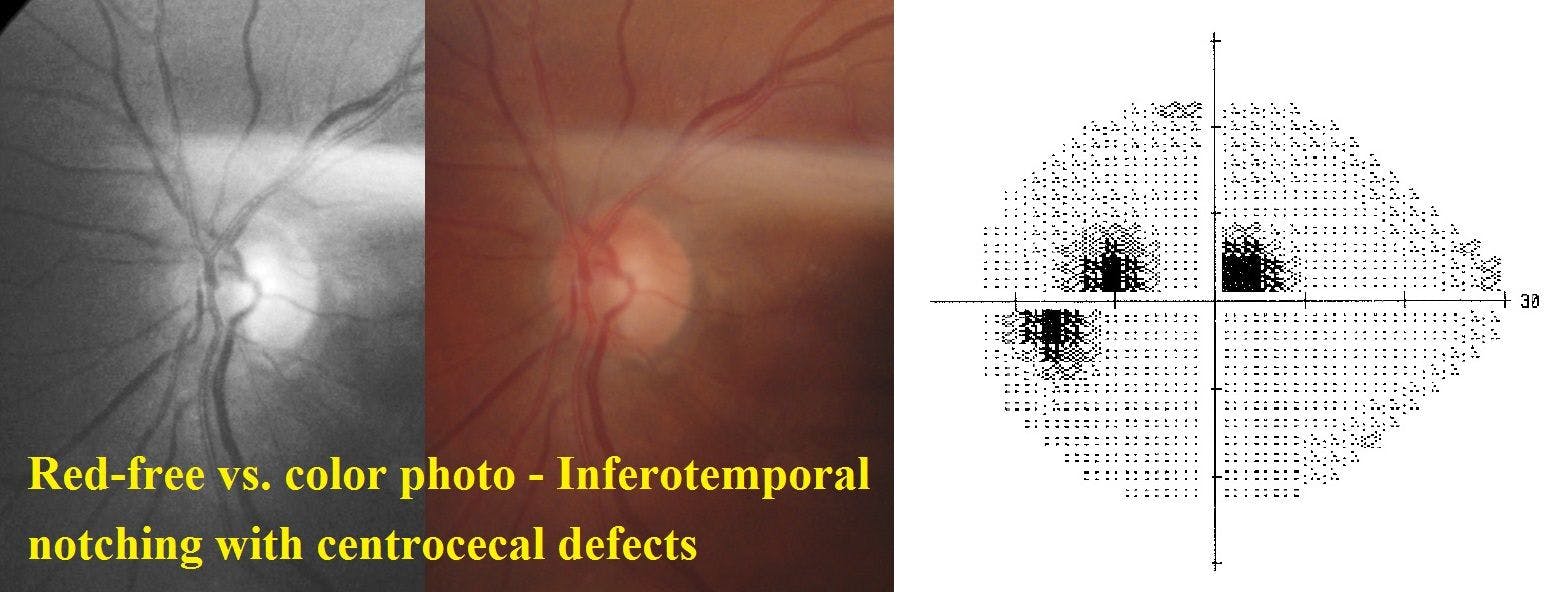
Figure 6: With frank notching or erosion of the neuroretinal rim, patients will present with corresponding visual field defects that mirror the glaucomatous optic neuropathy. Assessing the ganglion cell count on macular OCT scan can also be a useful tool when assessing a glaucoma risk, or determining the presence or progression of central visual field defects. The inferotemporal portion of the ganglion cell layer within the macula is referred to as the macular vulnerability zone33—correlating with superior centrocecal defects as shown above.
During the initial glaucoma workup, it is not uncommon to conduct three or more 24-2 VF tests over the course of 12 months.
Patients who struggle with formal VF testing may benefit from repeated explanations of the test, hearing a repeated dialogue during the test—“you’re doing great, don’t move your eyes or head,” or even alternating testing spot size, such as increasing to size five vs. size three default. Increasing spot size can also be beneficial in monitoring patients with more advanced glaucoma. To avoid fatigue and improve testing reliability, practitioners can also alternate which eye is tested first, especially if you’re initially only concerned about one eye. Due to spectacle mag and distortion of the visual field, patients with high refractive error (+/- 7.00 diopters) maybe perform better with a contact lens during the test.
When you’ve repeated numerous VFs and continue to obtain unreliable results, it may be time to switch to relying on objective testing in your glaucoma management plan. This primarily includes serial IOP readings and OCT scans, as well as pachymetry and gonioscopy.

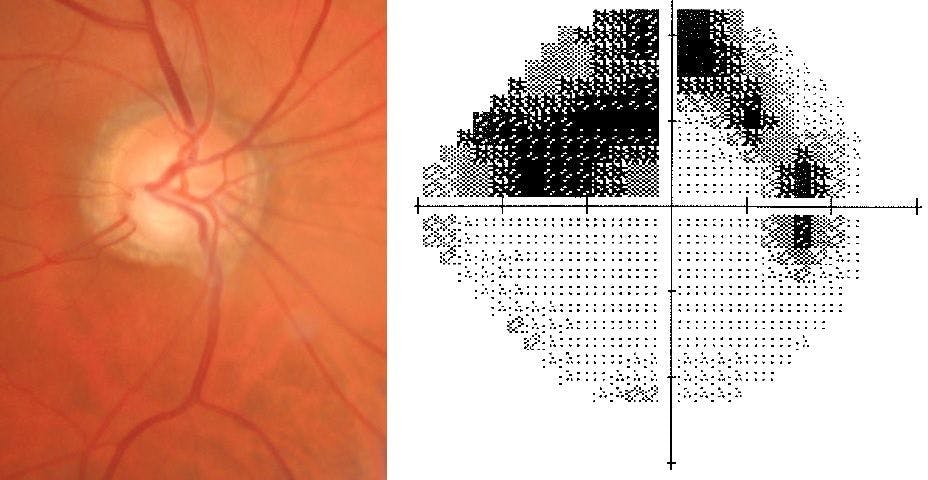
Figure 7: Inferior notching with corresponding classic superior arcuate defect shown on 24-2 visual field testing. Given this visual field defect involves fixation, periodic 10-2 visual fields will also be obtained to better assess progression. Remember that glaucomatous VF defects will always respect the horizontal meridian, while non-glaucomatous optic neuropathy typically respects the vertical meridian.


Fig 8. Performing gonioscopy is also important as part of the diagnosis of primary open angle glaucoma. Sure, the angle may look wide open on a Van Herick assessment, but performing gonioscopy allows the practitioner to detect an angle abnormalities such as angle recession or neovascularization, as well as determine level of pigmentation. More pigment present in the angle can improve outcomes of SLT laser treatment.
Tips to improve compliance
Patient communication
Sometimes holding patients accountable for taking their glaucoma drops can improve compliance. This can be done simply by making a spreadsheet/grid with your office’s header at the top, and includes the names, dates, and times of all drops prescribed (similar to a journal).
Collaborating with spouses, caretakers, or other family members can also be a useful way to maintain compliance with topical glaucoma treatment.
Right off the bat, if patients flat out tell you they’re not interested in committing to using eye drops on a routine basis, or you suspect there will be poor compliance, a referral to ophthalmology is your best bet. Optometrists can explain other treatment options to the patient and opt for referral to have the patient undergo selective laser trabeculoplasty (SLT) or even MIGS if the patient will be undergoing cataract surgery. Cataract surgery alone can also drop intraocular pressure by several points, even putting the patient within your target IOP range.
Minimizing the treatment burden for the patient is key to successful outcomes. Unfortunately, most patients will not be compliant with taking three or more eye drops on a daily basis. For this reason, most practitioners will always start with a prostaglandin analogue (generic version ok) dosed just once in the evening. Sometimes patients will ask if a specific time is really important, and most ODs will agree simply one drop in each eye “in the evening” will suffice. Whether it’s before or after dinner, walking the dog, or watching their favorite television show is really up to the patient. Also, the difference in therapeutic IOP reduction with prostaglandins is somewhere around 1mm Hg when taken in the am vs. pm, therefore taking them ANY TIME of day is more efficacious than poor compliance in the evening as typically directed.

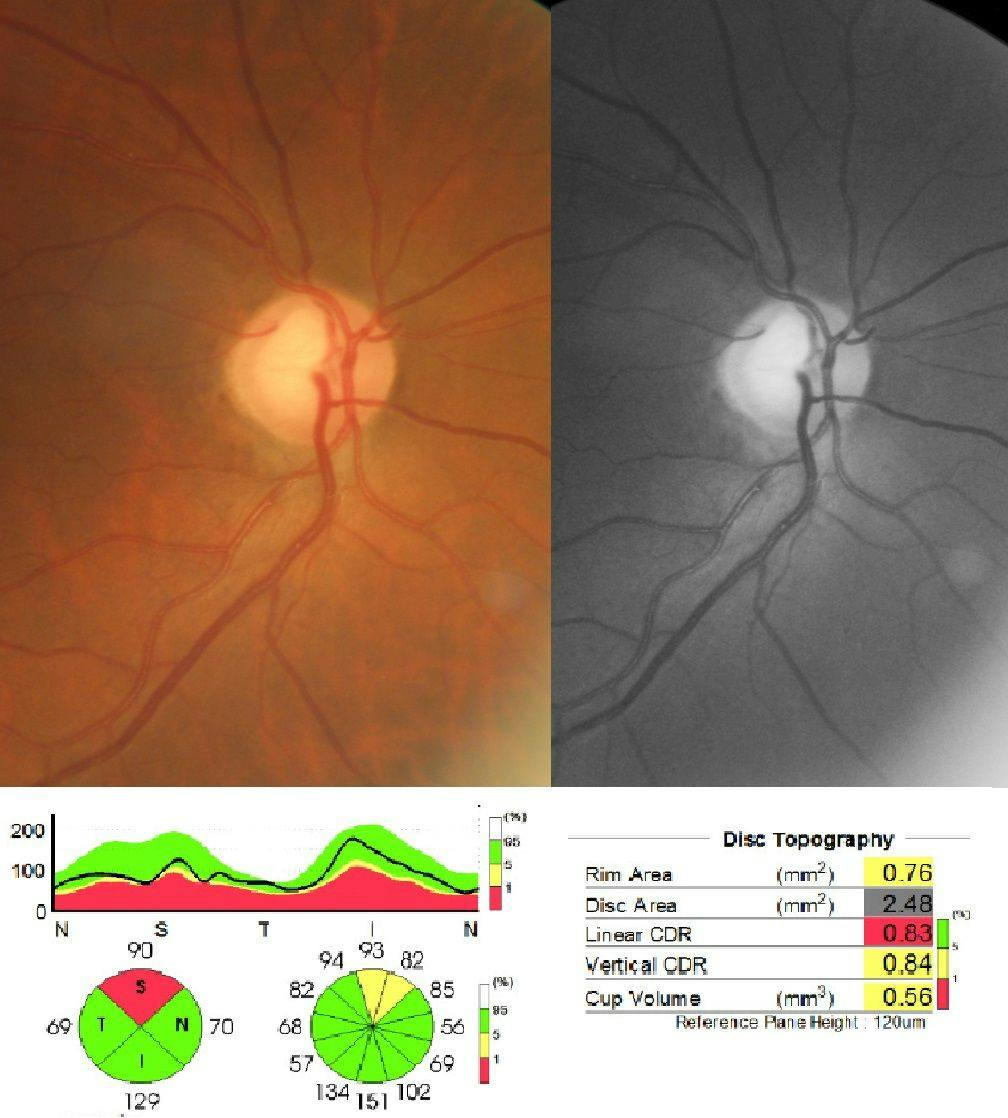
Fig 9. Primary open angle glaucoma of the right eye, with superotemp RNFL wedge defect and correlating RNFL thinning on OCT. Interpret OCT test results in context with the visual field and your stereoscopic assessment of the patient’s optic nerve. Never diagnose glaucoma solely on the OCT scan alone (e.g., “red disease”). The reference ranges of the OCT do not scale across all patient races/demographics, and therefore must be factored into the larger clinical picture.
Conclusion
Summary
Overall, treating glaucoma can be a challenging but rewarding experience for both the practitioner and patient. Offering to manage and treat glaucoma can also be an excellent practice builder. It is important to have the full clinical picture before making a definitive diagnosis. While IOP reduction is currently the only evidence-based treatment for glaucoma, it is important to assess your patient’s other systemic risk factors and comorbidities. With a thorough work up and systematic approach, your patients with POAG or at risk for developing glaucoma will greatly benefit from your expertise as their primary eye care provider.
References
- “Primary Open-Angle Glaucoma Suspect PPP - 2015.” American Academy of Ophthalmology, 30 May 2018, www.aao.org/preferred-practice-pattern/primary open-angle-glaucoma-suspect-ppp-2015
- Kass, M. A., Zimmerman, T. J., Alton, E., Lemon, L., & Becker, B. (1978). Intraocular Pressure and Glaucoma in the Zuni Indians. Archives of Ophthalmology, 96(12), 2212-2213. doi:10.1001/archopht.1978.03910060514008
- Wild, S. H., Roglic, G., Green, A., Sicree, R., & King, H. (2004). Global Prevalence of Diabetes: Estimates for the Year 2000 and Projections for 2030: Response to Rathman and Giani. Diabetes Care, 27(10), 2569-2570. doi:10.2337 diacare.27.10.2569-a
- Zhao, Di, Juhee Cho, Myung Kim, and David Friedman. “Diabetes, Glucose Metabolism, and Glaucoma: The 2005-2008 National Health and Nutrition Examination Survey.” PLoS One Open Access Journal. PLoS One, 13 Nov. 2014. Web. 28 Feb. 2016
- Chopra, Vikas, MD, Rohit Varma, MD, MPH, Brian A. Francis, MD, and Et Al. “Type 2 Diabetes Mellitus and the Risk of Open-angle Glaucoma the Los Angeles Latino Eye Study.” American Academy of Ophthalmology Journal (2007): 227-32. Amerian Academy of Ophthalmology, 22 Aug. 2007. Web. 28 Feb. 2016
- Zhou M, Wang W, Huang W, Zhang X. Diabetes Mellitus as a Risk Factor for Open-Angle Glaucoma: A Systematic Review and Meta-Analysis. Vavvas D, ed. PLoS ONE. 2014;9(8):e102972. doi:10.1371/journal.pone.0102972
- Newman-Casey PA, Talwar N, Nan B, Musch DC, Stein JD. The Relationship Between Components of Metabolic Syndrome and Open-Angle Glaucoma Ophthalmology. 2011;118(7):1318-1326. doi:10.1016/j.ophtha.2010.11.022
- Sato, Tsuyoshi, and Sayon Roy. “IOVS | Effect of High Glucose on Fibronectin Expression and Cell Proliferation in Trabecular Meshwork Cells.” IOVS | Effect of High Glucose on Fibronectin Expression and Cell Proliferation in Trabecular Meshwork Cells. Investigative Ophthalmology and Vision Science, 5 May 2001. Web. 02 Mar. 2016
- Lopes de Faria JM, Russ H, Costa VP. Retinal nerve fibre layer loss in patients with type 1 diabetes mellitus without retinopathy. The British Journal of Ophthalmology. 2002;86(7):725-728.
- Lonneville, Yıldız H., şengül C. özdek, Merih önol, &idot;lhan Yetkin, Gökhan Gürelik, and Berati Hasanreisoğlu. “The Effect of Blood Glucose Regulation on Retinal Nerve Fiber Layer Thickness in Diabetic Patients.” Ophthalmologica 217.5 (2003): 347-50. Web. 2 Mar. 2016.
- Barber, A. J., E. Lieth, S. A. Khin, D. A. Antonetti, A. G. Buchanan, and T. W. Gardner. “Neural Apoptosis in the Retina during Experimental and Human Diabetes. Early Onset and Effect of Insulin.” Journal of Clinical Investigation J. Clin. Invest. 102.4 (1998): 783-91. Web. 2 Mar. 2016.
- Kim, Y H, et al. “High Intraocular Pressure Is Associated with Cardiometabolic Risk Factors in South Korean Men: Korean National Health and Nutrition Examination Survey, 2008-2010.” Eye (London, England)., U.S. National Library of Medicine, June 2014, www.ncbi.nlm.nih.gov/pubmed/24603415
- Son J, Koh H, Son J. The association between intraocular pressure and different combination of metabolic syndrome components. BMC Ophthalmol. 2016;16:76. Published 2016 Jun 6. doi:10.1186/s12886-016-0263-8
- Kanamori, A., Nakamura, M., Mukuno, H., Maeda, H., & Negi, A. (2004). Diabetes has an additive effect on neural apoptosis in rat retina with chronically elevated intraocular pressure. Current Eye Research, 28(1), 47-54. doi:10.1076 ceyr.28.1.47.23487
- Chan, T C, et al. “Risk Factors for Rapid Glaucoma Disease Progression.” American Journal of Ophthalmology., U.S. National Library of Medicine, Aug. 2017, www.ncbi.nlm.nih.gov/pubmed/28624324
- Jain, V, et al. “The Association between Cigarette Smoking and Primary Open Angle Glaucoma: a Systematic Review.” International Ophthalmology., U.S. National Library of Medicine, Feb. 2017, www.ncbi.nlm.nih.gov/pubmed/27138591
- Bonovas, S, et al. “Epidemiological Association between Cigarette Smoking and Primary Open-Angle Glaucoma: a Meta-Analysis.” Public Health., U.S. National Library of Medicine, June 2004, www.ncbi.nlm.nih.gov/pubmed/15121434
- Kamble, Ganesh, et al. “Intraocular Pressure Changes in Smokers and Nonsmokers -.” International Journal of Medical Science and Public Health, 1 Jan. 1970, www.scopemed.org/?mno=211540
- Lee, A J, et al. “Does Smoking Affect Intraocular Pressure? Findings from the Blue Mountains Eye Study.” Journal of Glaucoma., U.S. National Library of Medicine, June 2003, www.ncbi.nlm.nih.gov/pubmed/12782837
- Jonas, Jost. “Clinical Implications of Peripapillary Atrophy in Glaucoma.” Current Opinion in Ophthalmology, Ovid Technologies, Inc, 2005, insights.ovid com/pubmed?pmid=15744137
- Chan, T C, et al. “Risk Factors for Rapid Glaucoma Disease Progression.” American Journal of Ophthalmology., U.S. National Library of Medicine, Aug. 2017, www.ncbi.nlm.nih.gov/pubmed/28624324
- Kass MA, Gordon MO, Gao F, et al. Delaying treatment of ocular hypertension: the Ocular Hypertension Treatment Study. Arch Ophthalmol. 2010;128(3):276-28
- Higginbotham EJ, Gordon MO, Beiser JA, et al. The Ocular Hypertension Treatment Study: topical medication delays or prevents primary open-angle glaucoma in African American individuals. Arch Ophthalmol. 2004;122(6):813-820
- Bryn Mawr Communications, and Michael A. Kass. “The Ocular Hypertension Treatment Study.” Glaucoma Today, 2011, glaucomatoday.com/2011/06/the ocular-hypertension-treatment-study/
- Jóhannesson, Gauti, et al. “Intracranial and Intraocular Pressure at the Lamina Cribrosa: Gradient Effects.” Current Neurology and Neuroscience Reports, Springer US, 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5897485/
- Wostyn, P, et al. “Intracranial Pressure and Glaucoma: Is There a New Therapeutic Perspective on the Horizon?” Medical Hypotheses., U.S. National Library of Medicine, Sept. 2018, www.ncbi.nlm.nih.gov/pubmed/30037625
- Fleischman, David, et al. “Cerebrospinal Fluid Pressure Decreases with Older Age.” PLOS ONE, Public Library of Science, 26 Dec. 2012, journals.plos.org plosone/article?id=10.1371%2Fjournal.pone.0052664
- “Ocular Hypertension to Glaucoma Risk Calculator.” Ocular Hypertension to Glaucoma Risk Calculator, oil.wilmer.jhu.edu/risk/
- Konstas, A G, et al. “Diurnal Intraocular Pressure in Untreated Exfoliation and Primary Open-Angle Glaucoma.” Archives of Ophthalmology (Chicago, Ill. : 1960)., U.S. National Library of Medicine, Feb. 1997, www.ncbi.nlm.nih.gov pubmed/9046252
- “2018 Ophthalmic Drug Guide.” Review of Optometry, Review of Optometry, 2018, www.reviewofoptometry.com/publications/2018-ophthalmic-drug-guide
- “New Perspectives on Target Intraocular Pressure.” Survey of Ophthalmology, Elsevier, 8 Apr. 2014, www.sciencedirect.com/science/article/pii S0039625714000769?via%3Dihub
- “AOA Optometric Clinical Practice Guidelines.” American Optometric Association, www.aoa.org/optometrists/tools-and-resources/clinical-care publications/clinical-practice-guidelines
- Blumberg, D M, et al. “Association Between Undetected 10-2 Visual Field Damage and Vision-Related Quality of Life in Patients With Glaucoma.” JAMA Ophthalmology., U.S. National Library of Medicine, 1 July 2017, www.ncbi.nlm nih.gov/pubmed/28542692
