In this talk, Leslie O’Dell OD, FAAO discusses EYSUVIS™ and its revolutionary ability to treat dry eye flares. Dr. O’Dell, the Clinical Director of Medical Optometry America, is speaking on behalf of Kala Pharmaceuticals to spread the word—short-term treatment can now be poised as a first-line prescription choice as part of your dry eye treatment arsenal.
What is EYSUVIS™?
EYSUVIS™(loteprednol etabonate ophthalmic suspension) 0.25%, is the first and only FDA-approved corticosteroid specifically developed for the short-term treatment (up to two weeks) of the signs and symptoms of dry eye disease (DED). It is powered by AMPPLIFY®, Kala’s novel mucopenetrating drug delivery technology with two proprietary attributes: (i) a nanoparticle size below 500 nm and (ii) a mucus-penetrating surface coating to facilitate the penetration of the mucus barrier.1-4
Dry Eye Disease
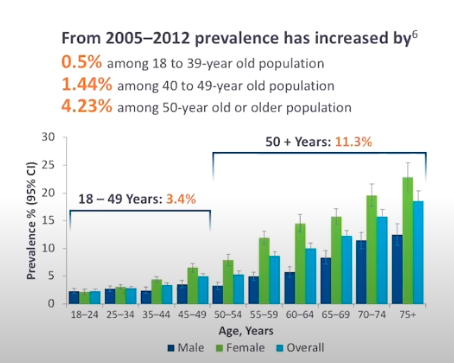
Nearly 38 million Americans have symptoms consistent with dry eye disease, but only 17.2 million are diagnosed.5-7 Common risk factors include female gender, being postmenopausal, and in many cases age, but DED is becoming increasingly prevalent in younger age groups.
Now that screen time is at an all-time high, we are seeing the incidence of DED rising amongst all age groups.
It is well understood that DED is chronic in nature; however, it does not necessarily mean that all patients suffer from continuous symptoms. DED must be treated for its root cause and not just the symptoms. Inflammation leads to an unstable tear film, loss of homeostasis, ocular surface stress, and a breakdown of tissues eventually leading to ocular surface damage.9,10 This risk for irreversible tissue damage is why it’s important to be proactive in diagnosing and treating the root cause.
Signs and symptoms of dry eye include redness and conjunctival hyperemia, ocular surface staining, discomfort, blurry vision, and fluctuating vision. Patients may overlook or suffer through these potential symptoms, and simply dismiss with the assumption “that’s just how it is.”
Many patients might only seek treatment during episodic flares, which are a common feature of many chronic inflammatory and autoimmune diseases such as asthma, Sjögren’s syndrome, and rheumatoid arthritis.11
DED can lead to decreased workplace productivity—affecting it by as much as 30%. Additionally, it has been shown to make it 2-3x more difficult to perform daily tasks.12,13
Dry Eye Flares
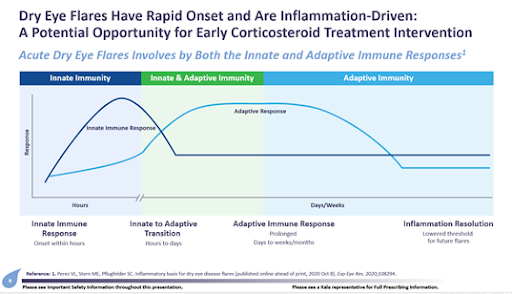
Dry Eye Flares are inflammation-driven and have a rapid onset. Patients will often experience acute flares due to innate and adaptive immune responses. The innate response has a rapid onset within a few hours of exposure which can trigger inflammation on the ocular surface. The transition to the adaptive immune response can occur hours to days after a threat to the ocular surface with an elegant ability to possess an immunological memory of previous exposure to certain pathogens.14
If the adaptive response were to go unchecked though, the bar can be raised which could ramp up T-cell mediated activity; thereby, setting up a longer and more severe exacerbation lasting from days to weeks. Subsequently, with each new inflammatory episode, the immune system has already been primed with a lower threshold for future dry eye flares facilitating an increase in patient symptomatology such as redness, irritation, fluctuating vision, pain, or itching.
The characteristics of Dry Eye Flares15,16 include:
- Rapid onset inflammation
- Occurs in response to a variety of triggers
- Can’t be managed with chronic medications the patient is already taking
- With or without maintenance therapy, dry eye patients experience flares and want rapid relief
- Happens multiple times a year
These flares are when the patient notices the most discomfort, but the underlying condition is still at play. It’s important to speak with the patient about their experience and when they are having flares since it could be up to 4-6 times per year.17-19
Asking stepwise patient-friendly questions can be helpful to uncover those suffering from dry eye flares;
- Do you ever experience a dry eye flare, which are periods of time where your dry symptoms may get worse or even feel like your dry eye symptoms are like a “roller coaster”?
- Can you remember back in the last few months if you had dry eye flare(s) which may have lasted a few days to a couple of weeks?
- Could you pinpoint what your symptoms felt like or eyes looked like to me?
- Have you noticed any particular triggers that may cause a dry eye flare? (i.e., screen time, contact lens use, allergies, systemic medications, dry/cool air)
- Would a quick-acting relief short-term medication to treat your dry eye flares and underlying causes of disease be of interest to you?
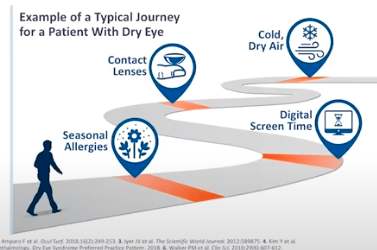
Dry eye is a journey
And just like any journey or road trip, it has speed bumps. These “speed bumps,” also known as episodic flares, are due to seasonal allergies, digital screen time, contact lenses, and cold or dry air.20-22
Most patients are not discussing dry eye flares with their ECPs. Many are just using artificial tears during these flares to help with symptom relief, but are doing nothing to stop the inflammation.
In fact, 91% of patients using approved dry eye products still experience flares.19 Because of this, patients on a chronic daily medication will often have issues with compliance. Patients look for immediate symptom relief, and a slower-acting medication that could take several weeks to months to provide symptom relief can discourage them from continuing with therapy.
45% of dry eye patients experience primarily flares and not constant symptoms. 80% of patients discontinue chronic medications after just 4 months.19,23
About EYSUVIS™
EYSUVIS’ AMPPLIFY® Drug Delivery technology uses mucus-penetrating particles to maximize effectiveness. Historically, mucus acts as a natural barrier to topical ophthalmic drug delivery. Because the ocular surface is constantly exposed to the environment, it makes sense for our eyes to have built-in defensive protection.1 But this can limit the penetration of drugs to target ocular tissue.
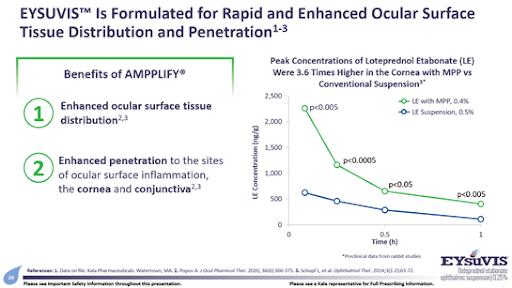
Since it can be difficult for medications to be absorbed by the ocular surface, EYSUVIS™ was designed with AMPPLIFY® novel drug delivery technology to have extremely small molecules (~300 nm) and a proprietary surface coating. These mucus penetrating nanoparticles allow the molecules to rapidly slip past mucins in the tear film to avoid adhesion thereby allowing for enhanced ocular surface tissue distribution and penetration (absorption) in order to get where it needs to be, specifically the cornea and conjunctiva.1-3
Formulated with AMPPLIFY®, EYSUVIS™ boasts better penetrative absorption, due to the smaller molecules allowing for a higher concentration of loteprednol etabonateto be absorbed even with less medication used.
EYSUVIS™ has the same contraindications as other corticosteroids. Prescribers should use caution when treating patients with existing viral, bacterial, or fungal infections. There is a very small risk of IOP elevation similar to vehicle, and 5% of patients experienced instillation site pain, so just be sure to monitor your patients as they undergo treatment.24
Patient care
EYSUVIS™ is a great solution for many patients. Its creation was hallmarked by the largest clinical development program in dry eye to date.3 Dry eye disease patients who suffer episodically from dry eye flares and use artificial tears on a regular basis may benefit from EYSUVIS™ as a first-line prescription choice. Other appropriate patients could be those undergoing eye surgery (i.e., cataract or refractive surgery) who also experience dry eye flares, chronic dry eye patients who use long-term medication experiencing breakthrough symptoms, or induction therapy for those individuals who might be placed on long-term maintenance therapy.
It’s important to consider your patient’s needs both when prescribing and also when explaining this medication to them. Remember that most patients are looking for immediate relief that is well-tolerated to minimize side effects. Since EYSUVIS™ is fast-acting and formulated to address the short-term needs of DED patients who may experience dry eye flares. Providing proper educational cues to the patient on why it is imperative to treat these episodic flares will help
combat noncompliance. Furthermore, it is essential to treat early and aggressively when DED patients experience flares to dampen the potential for future episodic exacerbations.
Meeting the Carpe Diem moment
Take a moment to consider the impact of your patients' dry eye speed bumps or triggers—what are lifestyle and environmental factors that may be contributing to dry eye? How much time do they spend on the computer or on digital devices? Do they go outdoors often? Do they use cosmetics or contact lenses? Being aware of these factors will all help when communicating with your patients and ensuring that their needs are met.
Until now, a medication specifically to treat dry eye flares has been an unmet need for many DED patients, and EYSUVIS™ fills this niche. As the first and only FDA-approved corticosteroid to treat dry eye, it is sure to be a useful asset in any dry eye treatment plan.
References:
- Popov A. J Ocul Pharmcol Ther. 2020; 36(6): 366-375.
- Schopf L, et al. Ophthalmol Ther. 2014;3(1-2): 63-72.
- Data on file. Kala Pharmaceuticals: Watertown, MA.
- Ensign LM, Schneider C, Suk JS, et al. Adv Mat. 2012;24(28): 3887-3894.
- Paulsen AJ et al. Am J Ophthalmol. 2014;157:799-806.
- Howden LM and Meyer JA. 2010 Census Briefs. 2011. http://www.census.gov.
- Market Scope. 2019 Dry Eye Products Market Report.
- Bron AJ, de Paiva CS, Chauhan SK, et al. Ocul Surf. 2017;15:438-510.
- Dana R, Bradley JL, Guerin A, et al. Am J Ophthalmol. 2019;202:47-54.
- Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276-283.
- Rosenblum MD et al. J Clin Invest. 2015;125(6):2228-2233. doi:10.1172/JCI78088.
- Nichols KK et al. IOVS 2016; 57(6) 2975-2982.
- Miljanović B, Dana R, Sullivan DA, Schaumberg DA. Am J Ophthalmol. 2007;143(3):409-415.
- Perez VL, Stern ME, Pflugfelder SC. Inflammatory basis for dry eye disease flares. Exp Eye Res. 2020;108294.
- ASCRS EyeWorld. https://www.eyeworld.org/download/file/fid/453. Published May 2019. Accessed Sept 1, 2020.
- American Academy of Ophthalmology Corneal/External Disease Panel. Preferred Practice Pattern Guidelines. Dry Eye Syndrome. San Francisco, CA: American Academy of Ophthalmology; 2018. Available at: www.aao.org/ppp.
- Brazzell RK, Zickl L, Farrelly J, et al. Prevalence and characteristics of dry eye flares: a patient questionnaire survey. Presented at: AAO 2019: Oct 12-15, 2019; San Francisco, CA.
- Brazzell RK, Zickl L, Farrelly J, et al. Prevalence and characteristics of symptomatic dry eye flares: results from patient questionnaire surveys. Poster presented at: AAOPT 2019: Oct 23-27, 2019; Orlando, FL.
- 2020 Study of Dry Eye Sufferers. Conducted by Multi-sponsors Surveys, Inc.
- American Academy of Ophthalmology. Dry Eye Syndrome Preferred Practice Pattern. 2018.
- Walker PM et al. Clin Sci. 2010;29(6):607-612.
- Tesόn M et al. Investig Ophthalmol Vis Sci. 2013;54(3):2093-2099.
- NPA Market Dynamics IQVIA data, June 2018-June 2019, as reported in October 2019, Restasis (N=24,340) and Xiidra (N=13,037).
- Korenfeld et al. Safety of KPI-121 Ophthalmic Suspension 0.25% in Patients With Dry Eye Disease. Cornea. 2020. doi: 10.1097/ICO.0000000000002452.