





Introduction
Optometrists play critical peri-operative roles for patients undergoing ocular surgery, as some ocular pathologies are first diagnosed during routine eye examinations in primary care.1 In particular, optometrists help identify patients in need of surgery, educate patients about their conditions, guide patients toward making informed treatment decisions, and help facilitate access to surgical treatment.1 When providing patients with care and making appropriate referrals, a strong optometrist–ocular surgeon relationship is critical.1
Because surgical procedures impose mechanical trauma to and induce inflammation in affected tissues, topical corticosteroids play a central role in the management of inflammation and pain that may arise after ocular surgery.2 LOTEMAX® SM (loteprednol etabonate ophthalmic gel) 0.38% is a corticosteroid indicated for the treatment of postoperative inflammation and pain following ocular surgery.3 Distinct from prior entries in the LOTEMAX franchise, LOTEMAX® SM has a drug particle size reduced to the submicron (nanometer) range in diameter through application of SM Technology™, allowing for improved drug dissolution and more efficient ocular penetration.2 This, in turn, permits a reduction in drug concentration in the formulation (from 0.5% to 0.38%) and dosing frequency (from 4 times daily to 3 times daily), with possible implications for drug safety and patient adherence to the dosing regimen.2
In this roundtable discussion, 4 leading optometrists shared their perspectives on both the formulation features and the clinical performance of LOTEMAX® SM. The faculty also explored the broad utility of LOTEMAX® SM following diverse ocular surgeries, highlighting the central role of the optometrist in helping to ensure that a prescription for LOTEMAX® SM is properly pulled through at the pharmacy and not subjected to generic substitution.
Formulation Features of LOTEMAX® SM
Dr. Devries: LOTEMAX® SM represents an important advancement in the history of the LOTEMAX franchise, which has been anchored in its consistent use of the corticosteroid loteprednol etabonate (Figure 1).2 My experience with loteprednol etabonate has been largely favorable. It was very smart of Bausch + Lomb to retain this trusted corticosteroid while evolving and advancing the formulation in which it’s housed.


Dr. Hubbard: I’ve consistently prescribed loteprednol etabonate over the years, across its multiple formulations. It has been a trusted, reliable corticosteroid in my toolkit.
Dr. Devries: It’s important to recognize that while loteprednol etabonate hasn’t changed over the years, its delivery system has. I cannot overemphasize the importance of LOTEMAX® SM's method of delivery—its vehicle. As with LOTEMAX® GEL (loteprednol etabonate ophthalmic gel) 0.5%, the inclusion of polycarbophil in the formulation helps enhance widespread coverage and prolong exposure on the ocular surface to maximize absorption potential.4
Dr. Schweitzer: The defining attribute of LOTEMAX® SM is the submicron particle size of the corticosteroid. The submicron particles in LOTEMAX® SM have more surface area exposed to tears compared with the micron-sized particles in LOTEMAX® GEL, which drives more rapid drug dissolution of LOTEMAX® SM.4
Dr. Devries: I agree that drug dissolution is important, because drug dissolution has implications for drug pharmacokinetics and tissue penetration. In pharmacokinetic studies in rabbits, LOTEMAX® SM efficiently penetrated the ocular surface, with approximately 2-fold greater penetration to the aqueous humor than LOTEMAX® GEL (Figure 2).4 I find myself telling colleagues, “There’s a lot of complicated science that goes into the LOTEMAX® SM formulation, but the connection between dissolution and ocular penetration is actually simple and straightforward.”


Dr. Hubbard: What I appreciate about LOTEMAX® SM is that the product is moisturizing. LOTEMAX® SM is formulated with glycerin and propylene glycol, which are established moisturizing ingredients.3,4 LOTEMAX® SM also contains a low level of the preservative benzalkonium chloride—just 0.003%.3,4 Many of my patients undergoing ocular surgery have concomitant dry eye or other ocular surface disease, and these attributes of LOTEMAX® SM reinforce its appropriateness for this subgroup of patients.
Dr. Kislan: What’s particularly interesting about LOTEMAX® SM is the nonsettling nature of the formulation. There is no need to shake the LOTEMAX® SM bottle before administering the product, and the product shows good dose uniformity even without shaking, with a consistent amount of loteprednol etabonate delivered in each drop.4,5 In fact, in a head-to-head comparison of LOTEMAX® SM vs branded and generic forms of prednisolone acetate suspension 1%, unshaken LOTEMAX® SM showed consistent dose uniformity over time, whereas both forms of unshaken prednisolone acetate suspension 1% showed considerable dose variability.5 This gives me a degree of confidence in LOTEMAX® SM that I don’t have with branded or generic prednisolone acetate suspension 1%.
Dr. Devries: Thanks to the dose uniformity of LOTEMAX® SM, when a patient of mine receives a drop, I know exactly what’s in that drop. This is one fewer thing that my patients and I have to worry about.


Dr. Kislan: I prioritize patient comfort. If my patients find their drops irritating or uncomfortable, they’re less likely to adhere to treatment. There are many factors that contribute to the comfort of eye drops, but the important thing to remember about LOTEMAX® SM (loteprednol etabonate ophthalmic gel) 0.38% is that in the Phase 3 trials, over 3 in 4 patients receiving LOTEMAX® SM reported no drop discomfort, and no patients receiving LOTEMAX® SM reported blurred vision.6 My patients consistently report that they find LOTEMAX® SM comfortable and want to continue using it as prescribed.
Dr. Schweitzer: In my view, minimizing the risk of blurred vision is the key to maximizing patient satisfaction. Blurred vision is the most common complaint I hear from my patients who are receiving prescription drops for any reason, but I haven’t heard this complaint from any of my patients receiving LOTEMAX® SM.

Clinical Performance of LOTEMAX® SM
Dr. Devries: The efficacy results observed in the Phase 3 trials of LOTEMAX® SM underscore the clinical importance of ocular corticosteroids for the management of postoperative inflammation and pain. In these trials, significantly more patients had zero anterior chamber cells and Grade 0 (no) pain at Day 8 with LOTEMAX® SM than with vehicle (Figure 3).3,6 The absence of anterior chamber cells, in particular, is reassuring to eye care professionals because it helps establish that a patient’s postoperative inflammation is under control.


Dr. Schweitzer: When looking at the proportions of patients achieving zero anterior chamber cells, it’s important to recognize that an absence of anterior chamber cells is a rather stringent endpoint. In my experience, just about any motivated investigator can find an inflammatory cell in a patient’s anterior chamber if they look hard enough. This makes the anterior chamber cell outcomes with LOTEMAX® SM seem that much more impressive to me.
Dr. Kislan: What I find particularly exciting about the trial data for LOTEMAX® SM is that clinically meaningful results were obtained quickly, with statistically significant improvements in the coprimary endpoints obtained at postoperative Day 8.3,6 In real-world, practical terms, results like these mean that many of my patients can be cleared of their postoperative inflammation and pain quickly, and may require less follow-up care. This, in turn, can help improve the efficiency of my practice and increases the volume of patients I can treat.
Dr. Devries: I echo the importance of practice efficiency. Ineffective treatments result in wasted time for both me and my patients, which has a real-world cost that can negatively impact an optometry practice. Utilization of effective medications like LOTEMAX® SM can help mitigate this concern.
Dr. Hubbard: While I agree the efficacy data in support of LOTEMAX® SM are impressive, I’m also impressed by the safety outcomes. There were no treatment-emergent adverse drug reactions that occurred in more than 1% of patients in clinical trials.3,6 In addition, only 1 out of 369 patients receiving LOTEMAX® SM experienced significant intraocular pressure (IOP) elevations of ≥10 mmHg, which was comparable to the IOP elevations seen with vehicle.6 These outcomes are highly relevant to me as an optometrist because in my experience 30%-40% of patients are steroid responders and I have to remain vigilant about possible IOP spikes. In my real-world experience, I rarely see IOP spikes with LOTEMAX® SM, which is consistent with the clinical trial findings. The recommended guidance for LOTEMAX® SM is that if the product is to be used for 10 days or longer, IOP should be monitored.3

Dr. Devries: Some of our optometry colleagues have reasonable concerns about corticosteroid-induced IOP elevation. What I tell them is that in the clinical trials, over 99% of LOTEMAX® SM–treated patients did not experience IOP elevations of ≥10 mmHg.6 This outcome is very striking when expressed in percentage terms.
LOTEMAX® SM Following A Variety of Ocular Surgeries
Dr. Hubbard: All ocular surgeries cause tissue damage, which in turn can cause ocular inflammation and pain. Some of my patients have difficulty understanding this idea, but an analogy can be helpful. I explain that ocular surgery is like a spark, inflammation is like a fire, and a corticosteroid like
LOTEMAX® SM is like the water that can help extinguish the fire.
LOTEMAX® SM is like the water that can help extinguish the fire.
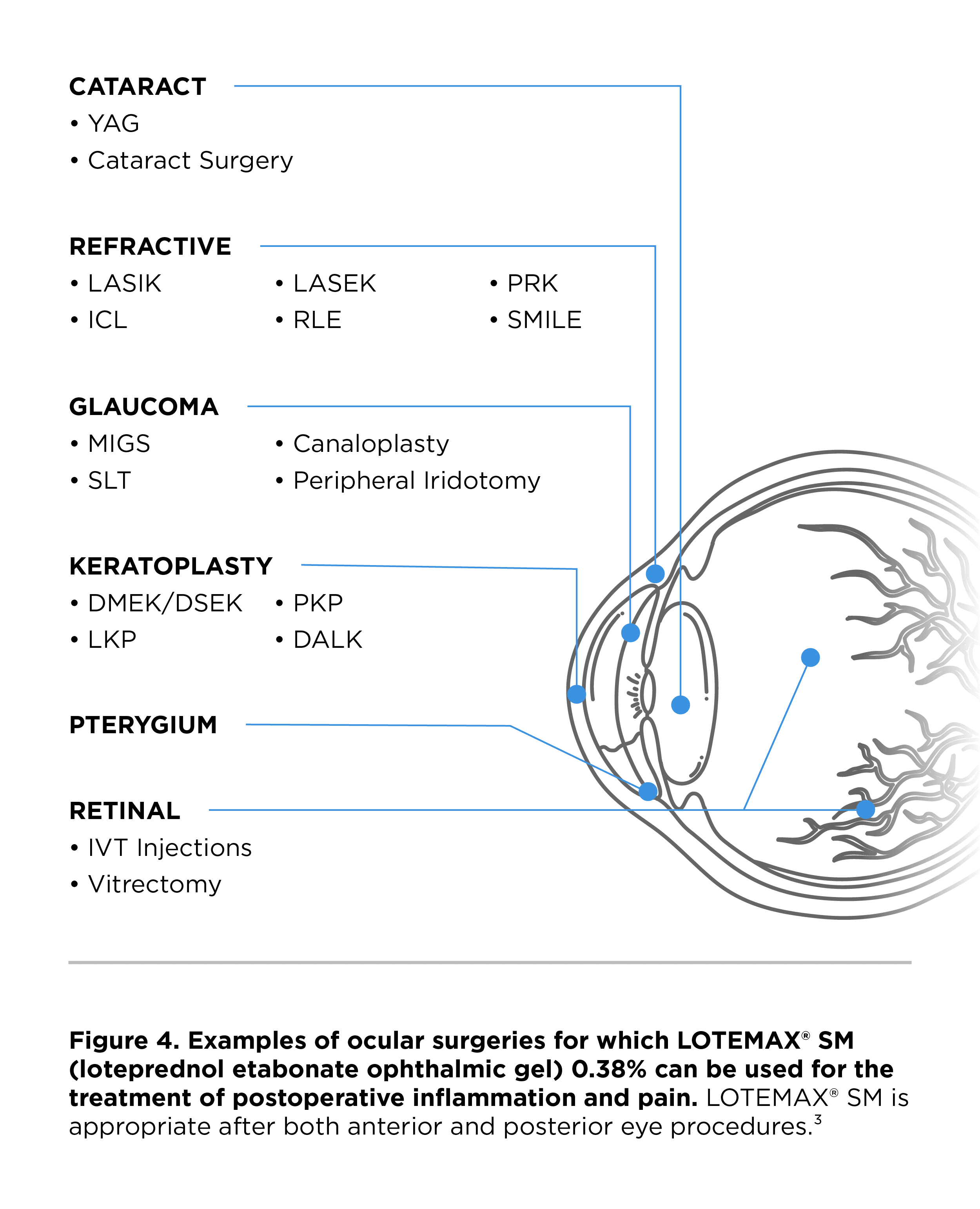
Dr. Kislan: My practice performs a wide array of ocular surgeries, and it’s remarkable that LOTEMAX® SM is appropriate for use after any of them (Figure 4).3 That said, we tend to recommend LOTEMAX® SM to patients receiving specialty intraocular lenses following cataract surgery, as we believe those patients benefit most from a potent corticosteroid. My retina colleagues also like to use LOTEMAX® SM following posterior eye procedures.


Dr. Schweitzer: My practice manages a large volume of patients undergoing glaucoma surgery. These tend to be patients who are experienced with IOP-lowering drops and are fearful of losing their vision. The last thing I want to do is complicate their treatment experience by introducing a corticosteroid drop that might cause blurred vision or induce IOP spikes. I find LOTEMAX® SM very helpful for managing postoperative inflammation and pain in patients who need a corticosteroid option with a low risk of IOP elevation.
Dr. Kislan: I tell my surgical colleagues that every extra minute of ocular surgery may translate into greater potential for postoperative inflammation. I emphasize the importance of using a corticosteroid drop that can address postoperative inflammation regardless of what type of ocular surgery caused it.
Dr. Devries: On occasion, optometrists are hesitant to talk to their surgical colleagues. The reasons for this vary—a few optometrists find surgeons intimidating, while others do not wish to encroach onto surgeons’ clinical territory—but the conversation needs to happen regardless. In fact, I’ve heard some surgeons say, “A steroid is a steroid; they’re all the same.” I believe this misconception is caused by the fact that not all surgeons are able to actively participate in their patients’ postoperative recovery. It becomes the responsibility of the optometrist to communicate the bigger clinical picture to the surgeon, focusing on the attributes of different postoperative corticosteroids and the rationale for corticosteroid selection.
Dr. Kislan: Overcoming hesitation and building a strong optometrist–ocular surgeon relationship are critical for optimizing patient outcomes. I’ve worked with the same surgeon for 25 years, and we have an outstanding relationship. He tells me that I make his day better because I try to ensure that any patients I refer to him have a healthy ocular surface. He is usually aligned with my corticosteroid recommendations because he knows I have the patient’s best interests in mind.
Dr. Hubbard: Optometrists bring a unique perspective to the surgical conversation. I always ask my surgical colleagues if I can help take the ocular corticosteroid decision off their plate. If they are amenable to my input, I’ll consistently recommend LOTEMAX® SM for appropriate patients.
The Optometrist's Role in Prescription Pull-Through of LOTEMAX® SM
Dr. Hubbard: One of the most onerous challenges we encounter as optometrists is generic substitution at the pharmacy. LOTEMAX® SM is my preferred ocular corticosteroid—in fact, it’s the only one I like to use. For this reason, it’s critical that my patients receive their medication as prescribed and that the medication isn’t swapped by the pharmacy.
Dr. Schweitzer: In my experience, the main drivers of generic substitution are drug cost and access. My commercially insured patients usually have little difficulty receiving LOTEMAX® SM as prescribed. However, my Medicare patients are more challenging in terms of achieving successful prescription pull-through. I have to work especially hard on behalf of my Medicare patients.
Dr. Kislan: Drug cost and access are my main challenges as well. My colleagues are constantly learning about all the new drugs entering the market and the importance of ensuring that our patients receive the medications they need. It’s our responsibility to make sure that happens.
Dr. Hubbard: That is why I like to direct my patients to specialty pharmacies. I find that they’ll do the legwork needed to get the appropriately prescribed drug to the patient who needs it. Specialty pharmacies have distinguished themselves as organizations tirelessly working on behalf of both doctors and patients. I am very impressed by them.
Dr. Devries: Our office staff play such an important logistical and administrative role in managing prescriptions, so we have to educate them about the importance of prescription pull-through. I tell them, “I wouldn’t be able to do what I do without your help.” However, without proper education, staff may underestimate just how widespread a phenomenon generic substitution actually is. Research has identified considerable variation in generic substitution policies across the United States,7 although there is a paucity of data on ocular corticosteroid substitution trends more specifically.
Dr. Hubbard: I agree that our office staff need to feel like they have ownership over the prescription process. Understanding the pharmaceutical science and clinical reasoning that inform our prescribing decisions is essential— not just for our LOTEMAX® SM patients, but for all our ophthalmic patients.
INDICATION
LOTEMAX® SM (loteprednol etabonate ophthalmic gel) 0.38% is a corticosteroid indicated for the treatment of post-operative inflammation and pain following ocular surgery.
IMPORTANT SAFETY INFORMATION
• LOTEMAX® SM, as with other ophthalmic corticosteroids, is contraindicated in most viral diseases of the cornea and conjunctiva including epithelial herpes simplex keratitis (dendritic keratitis), vaccinia, and varicella, and also in mycobacterial infection of the eye and fungal diseases of ocular structures.
• Prolonged use of corticosteroids may result in glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision. Steroids should be used with caution in the presence of glaucoma. If LOTEMAX® SM is used for 10 days or longer, IOP should be monitored.
• Use of corticosteroids may result in posterior subcapsular cataract formation.
• The use of steroids after cataract surgery may delay healing and increase the incidence of bleb formation. In those with diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical steroids. The initial prescription and renewal of the medication order should be made by a physician only after examination of the patient with the aid of magnification such as slit lamp biomicroscopy and, where appropriate, fluorescein staining.
• Prolonged use of corticosteroids may suppress the host response and thus increase the hazard of secondary ocular infections. In acute purulent conditions, steroids may mask infection or enhance existing infections.
• Employment of a corticosteroid medication in the treatment of patients with a history of herpes simplex requires great caution. Use of ocular steroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex).
• Fungal infections of the cornea are particularly prone to develop coincidentally with long-term local steroid application. Fungus invasion must be considered in any persistent corneal ulceration where a steroid has been used or is in use. Fungal cultures should be taken when appropriate.
• Contact lenses should not be worn when the eyes are inflamed.
• There were no treatment-emergent adverse drug reactions that occurred in more than 1% of subjects in the three times daily group compared to vehicle.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088.
Please see additional Important Safety Information throughout and full Prescribing Information here.