


WHAT YOU'LL LEARN
How to recognize the signs, symptoms, and pathophysiology of diabetic retinopathy
How to identify the progression of diabetic retinopathy through the use of the 4-2-1 rule
How to develop a treatment plan for diabetic retinopathy and optimize patient compliance
Introduction and Quiz
Introduction
Diabetic retinopathy is the leading cause of vision loss among adults in the U.S.3 Since diabetes is also among the leading causes of morbidity and mortality, primarily through an increased risk of developing cardiovascular disease, the stakes are high in protecting our patients’ ocular health and visual function.6
In this course, we will cover the background, treatment, management, and differential diagnoses of diabetic retinopathy through the lens of a patient case encountered by Dr. Robert Africano, OD, FAAO, a member of the National Vision Doctor of Optometry Network employed by North Carolina Primary Vision Care Associates.
Background
The earliest microvascular complications from type 1 and type 2 diabetes can occur in the retina. Prolonged periods of hyperglycemia results in basement membrane thickening, endothelial cell dropout and pericyte loss within the retinal microvasculature.7 Ischemia within the retina results in an upregulation of vascular endothelial growth factor (VEGF), which in turn triggers retinal neovascularization.7 It has been shown that approximately 1 in 3 diabetic patients will develop some form of retinopathy over their lifetime.2
According to the CDC’s National Diabetes Statistic Report 2020, over 34 million US adults have diabetes, 7 million of whom are undiagnosed. The number of Americans diagnosed with diabetes has almost tripled since 2000 with about 95% of cases being type 2. After considering another 1 in 3 adults also has prediabetes,7 we see that almost half of the US adult population is potentially at-risk for developing sight-threatening retinopathy over the course of their lifetime.
Unfortunately, many patients with prediabetes and T2DM may adopt the destructive mindset of having an irreversible genetic condition. While this may potentially be the case for patients with type 1 diabetes, a completely different story exists for patients with type 2 diabetes.
According to the American Optometric Association, optometrists in the U.S. diagnose type 2 diabetes (T2DM) in well over a quarter-million patients per year, based on their eye examination alone.1 Up to 24,000 new cases of diabetic retinopathy occur annually,4 with a 40% expected increase by 2050.5
Patient Case
Case History
A 33-year-old black male presented for a yearly diabetic evaluation and comprehensive examination. Pertinent systemic history positive for Type 1 diabetes for over 30 years, moderate control per patient. Last systemic primary care evaluation was approximately 4 months ago and revealed an HbA1c of 8.4%. This morning’s last blood sugar reading was 206.
The patient’s last eye exam was 18 months prior with another provider. Visual acuity was 20/20 OU, anterior segment findings were unremarkable, and fundus evaluation revealed moderate diabetic retinopathy OU. The patient was referred and scheduled for a retina consult secondary to the severity and location of the hemorrhaging. Evidence of macula/parafoveal hemorrhaging/exudate put the patient at risk of clinically significant macula edema if blood sugar management was not improved. The patient did not show any indication of diabetic refractive shifts over the past 3 years via our records.
The patient was noncompliant with further retinal evaluation. Further attempts to reach the patient for an in house 6-month follow-up and further retinal evaluation were unsuccessful.
Several months after we had initially wanted to follow up with him, the patient ended up returning on his own due to a new onset in visual symptoms, primarily in the right eye.
Chief complaint
The patient reported new onset reduced vision OD. The patient was unsure of the duration but believed it may have been worsening over the last several months. However, he reported stability over the past few weeks. After further probing, the patient reported the reduction in acuity may have potentially occurred 6+ months prior to the evaluation. The patient reported that the reduction in acuity was moderate and gradual.
Case Findings and Diagnosis
- BCVA: OD: 20/400-, OS: 20/30-1
- PH: NI OU
- Pupils: PERRL (-) APD OU
- Extraocular muscles: Smooth and Full
- Confrontation Fields: full to finger count OD, full to finger count OS
- IOP NCT: OD 14, OS 15
- Slit lamp examination of the anterior segment: Unremarkable OU, with no evidence of NVI. Angle was not evaluated for NVA via gonioscopy at this time.

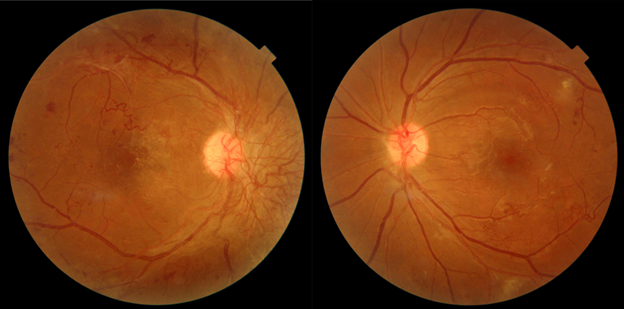
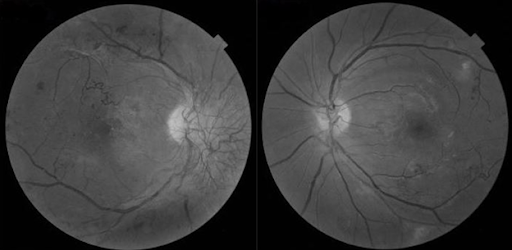
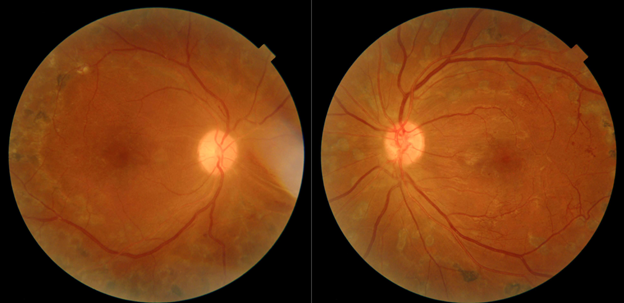
Dilated fundus examination at follow up: Scattered dot/blot hemorrhages OU, NVD OD>>OS; NVE OU with fibrotic changes OD with ERM.
Diagnosis
High risk proliferative diabetic retinopathy.
Treatment and Discussion
Treatment Plan
The patient was educated on the severity of his findings and risk to vision and ocular health. The patient was scheduled for an urgent retinal evaluation with expected panretinal photocoagulation (PRP) treatment OU and potential vitrectomy. Secondary to the patient’s history of noncompliance with follow-up care, the patient’s retinal exam was scheduled in office and risk of irreversible vision loss was repeatedly stressed.
The patient was seen the next day by a retinal specialist. Treatment options were discussed, including intravitreal anti-VEGF, panretinal photocoagulation, and vitrectomy. PRP was eventually performed at a later date.
The patient returned to our service for a 6-month follow-up and refraction. His vision remained stable OU, with little improvement OD. Pupil evaluation demonstrated a sluggish response OD post-PRP. The importance of further blood sugar control was stressed as well as full-time protective lens wear.

Discussion
Our patient reported moderate blood sugar control with elevated yet stable blood work. However, the patient’s lengthy duration of disease significantly increased his risk of developing sight-threatening retinopathy. The initial management plan for our patient was to closely monitor his level of retinopathy. The goal was to identify progression from moderate to severe diabetic retinopathy, via the 4-2-1 rule. When proliferative retinopathy is observed, prophylactic PRP is almost always performed in an attempt to reduce the patient’s risk of permanent vision loss. Unfortunately for our patient, he returned to our service presenting with high-risk PDR which was responsible for his vision loss OD.
It is imperative that when retinopathy is observed in patients with a long duration of diabetes (especially poorly controlled disease), they are followed more closely. If a patient’s severity progresses from moderate to severe by meeting the 4-2-1 rule, we must decide to monitor the patient far more closely or refer to ophthalmology for prophylactic treatment.
The 4-2-1 rule is used to classify severe nonproliferative diabetic retinopathy and is defined as severe retinal hemorrhages in all 4 quadrants of the posterior pole, significant venous beading in 2 or more quadrants, and/or moderate intraretinal microvascular abnormalities (IRMA) in 1 or more quadrants. Once patients progress to severe NPDR, we must strongly consider initiating retinal consultation, due to the likelihood of necessary treatment. Approximately half of all patients with severe nonproliferative retinopathy will further progress to proliferative status within 12 months.8,9 The ETDRS study demonstrated a statistically significant reduction in severe vision loss in eyes receiving early laser treatment. PRP is considered standard first-line treatment in the majority of cases for proliferative retinopathy.
Our patient is young, presented with moderate blood sugar control, and had only a history of moderate diabetic retinopathy at his initial exam with us. Yet his extensive duration of disease and poor follow-up compliance resulted in a loss of vision. As thus, the patient’s presenting with high-risk characteristics should be monitored appropriately to reduce the risk of vision loss, especially if extensive duration of disease is present.
It is essential that we educate our diabetic patients on ocular risk and follow-up compliance in an attempt to reduce the risk of vision loss that was seen in this case. The care provided did prevent further vision loss OS, however continued vigilance and blood sugar control is always necessary in managing the diabetic patient (regardless of type 1 vs. type 2).
Conclusion and References
Conclusion
It is the responsibility of primary eye care providers to help patients prevent long-term diabetic ocular complications. As integral members of the healthcare team, optometrists encounter a growing number of patients presenting with uncontrolled/undiagnosed metabolic disease such as type 2 diabetes. It is crucial to our patients’ ocular health that we understand how to assess, follow and co-manage patients with diabetic retinal changes, regardless of severity. By engaging with patients and discussing their health and risks of permanent vision loss, optometrists are able to have a more meaningful impact on our patients’ systemic health, ocular health, and lives.
References
- “21st-Century Optometric Care for the 21st-Century Pandemic.” American Optometric Association, 2018, www.aoa.org/news/clinical-eye-care/21st-century-optometric-care
- Lee, Ryan, et al. “Epidemiology of Diabetic Retinopathy, Diabetic Macular Edema and Related Vision Loss.” Eye and Vision (London, England), BioMed Central, 30 Sept. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4657234/
- “Watch Out for Diabetic Retinopathy.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 5 Nov. 2018, www.cdc.gov/features/diabetic-retinopathy/index.html
- “Economic Studies|Vision Health Initiative (VHI).” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 11 Apr. 2017, www.cdc.gov/visionhealth/projects/economic_studies.htm
- “Diabetic Retinopathy Data and Statistics.” National Eye Institute, U.S. Department of Health and Human Services, 2019, www.nei.nih.gov/learn-about-eye-health/resources-for-health-educators/eye-health-data-and-statistics/diabetic-retinopathy-data-and-statistics
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for Disease Control and Prevention, US. Dept of Health and Human Services (2017)
- Moreno, A., and M. Lozano, et al. “Diabetic Retinopathy.” Nutricion Hospitalaria, 2013, www.nutricionhospitalaria.com/pdf/6714.pdf
- Early Treatment Diabetic Retinopathy Study Research Group. Early photocoagulation for diabetic retinopathy: ETDRS report number 9. Ophthalmology. 1991;98:766-85
- Steven Ferrucci, OD. “Diabetic Retinopathy by the Numbers.” Review of Optometry, 15 June 2016, www.reviewofoptometry.com/article/diabetic-retinopathy-by-the-numbers#footnotes
