



Diagnosing and managing retinal disease
Diagnosing and managing retinal disease can be extremely overwhelming due to the vast number of ophthalmic and systemic manifestations that can be seen within the retina. I try to think about four major areas when managing our patients in a retina clinic. The first thing that is extremely important when managing any retinal condition is to think about risk factors. It’s also really important to think about what technology can be helpful when I’m trying to diagnose, differentiate, and monitor a patient as well as deciding when to manage a patient and when to refer to or collaborate with an ophthalmologist.
Step 1: What are a patient’s risk factors?
Step 2: What technology will be most helpful?
Step 3: How can we preserve a patient’s vision?
Step 4: How important is it that we get them in to see someone for management and treatment right away?
How the medical model of optometry factors into retinal disease
Ultimately, the key to incorporating the medical model of optometry is to think about treating the whole patient, rather than just thinking about the eye. Often patients have many confounding issues, including systemic conditions they are managing and may be struggling with.
Things I consider include:
- Who else needs to get involved?
- How else can we make sure we’re taking comprehensive care of our patients?
- What systemic manifestations for systemic diseases a patient might have, including diabetes, hypertension, or anything inflammatory, as those are going to increase the risk for retinopathy.
Case specific considerations when managing retina patient:
History of Trauma
It’s important to ask patients if they've ever had any history of trauma—especially if you are looking for macular holes or peripheral retinal lesions in patients with degenerative myopia. Degenerative myopia is a huge risk factor for sight threatening retinopathy, especially with myopia on the rise.
Systemic medications that may affect the retina
It’s also really important to understand any systemic medications a patient is on, as many can affect the retina. As primary care optometrists, we can monitor them easily and check for retinopathy on regular visits. In many cases, this can save a patient’s vision.
Risk factors for common retinopathy in diabetic patients
Main risk factors for diabetic retinopathy are:
- Duration of diabetes
- Analysis of HbAIc over time
- Number and types of medications they are taking
HbAIc—When speaking with patients, I always ask what their HbAIc is. Generally, if a patient doesn’t know what their HbAIc is, they don’t have an understanding about controlling their blood sugar and may not know if it’s trending up or trending down. This puts them at a higher risk for retinopathy because I feel they don’t understand their condition as well as they should, and that is something I’m going to take into account when we are educating the patient and working with them about their condition. It’s also important to look at the HbAIc over time, so it’s helpful to document the HbAIc at each visit, to see if the patient is improving or not.
Medications—It’s also very important to understand the medications a diabetic is taking. If they are just taking one medication, they are probably a type II diabetic. For example, if their condition is well-controlled with Metformin, that patient is less likely to have retinopathy. On the other hand, if a type II diabetic is on three medications plus insulin you can assume right off the bat, that the patient is at a higher level of risk.
Risk factors for common retinopathy in macular degeneration patients
We know genetics play a huge role. It’s always important to talk to patients about their family history and if anyone suffered from blindness. Did they have injections for wet macular degeneration? Specific questions can be helpful in understanding what we expect to see in our patients, as different genetic mutations tend to present similarly. For example, if a patient’s mother had wet macular degeneration, that patient most likely has a gene that will lead to them having wet macular degeneration as well as needing injections.
Other risk factors include:
- Smoking
- Elevated BMI
What is the role of multimodal imaging in the management of retinal disease?
I cannot imagine diagnosing and managing retinal disease without integrated advanced diagnostic technology.
My top three are:
- Optical coherence tomography (OCT)—this is number one for diagnosing and managing a variety of retinal conditions.
- Widefield fundus photography with autofluorescence—this helps you see problems you might not otherwise notice.
- Data management system—this enables you to dynamically look at images over time to make sure you understand patterns and disease progression in order to make decisions based on images over time.
OCT analysis to diagnose retinal disease
OCT analysis can be extremely helpful at differentiating clinical findings. Often, we’ll look at a retina, and sometimes it’s hard to tell which layer of the retina is affected. When you can look at an OCT image, you can differentiate it, which can help you more accurately describe and diagnose a specific condition.
When I use OCT in my practice, the first thing that I will always do is plan the scan. Planning the scan involves thinking about the type of scan that will be useful, the location of the questionable lesion, and the pathology that you are evaluating or differentiating. Once you know where in the eye the pathology is, you have a better idea of what to look for on the OCT. For example, if you have a diabetic patient—especially a high-risk diabetic patient—you could be looking at moderate to severe nonproliferative diabetic retinopathy (NPDR) or even proliferative diabetic retinopathy (PDR). So it’s important to look at all the places where you might see change including:
- Macula—you might see signs of retinal ischemia or macular ischemia.
- Arcades— this is where the neovascularization is likely to result.
- Optic disc—this is where you might see neovascularization.
If you are planning your scan, and are thinking about this and can take it to the next level, especially if you have OCT Angiography (OCTA) in your practice.
In diabetic patients on OCTA, we’re going to expect neovascularization at the vitreoretinal interface and microaneurysms in the deep retina, because that’s where the capillary bed lies. When you are looking at OCTA images and evaluating en face views, those areas are going to be very helpful for detection of pathology and discerning your next steps. Similarly, if you have an AMD patient looking at the choriocapillaris,choroid and the avascular zone on OCTA are going to be money shots to detect choroidal neovascularization.
If you don’t have OCTA in your practice, you can still use the B-scans from your OCT scans to analyze the same area . For example, we know that retinal ischemia results in a thinning of the retina in areas of extensive ischemia. While OCTA can make it easier to visualize capillary dropout, you can always use what you know about the conditions themselves and what higher level imaging can show you to understand what your patient may be experiencing, even if you don’t have the more advanced technology at your fingertips.
Ultra widefield fundus imaging detects RPE and atrophy
Ultra widefield photography is not going to replace your retinal exam but it is an important supplement. It is very important that you do a thorough dilated exam using your binocular indirect ophthalmoscope (BIO)to get out to the periphery to look for small holes, tears, and thinning.. If you’re seeing lattice with some atrophic holes within it, it’s amazing to have a photo of that. I also love using fundus photography for patient education. Patients really love being able to see what we see. A photo really does provide 1,000 words.
To elevate your retinal examination, it’s also very important for your patients to look at fundus autofluorescence on your fundus photography if you have it. There are so many conditions where we can see stress in the RPE and the atrophy you might not actually pick up on your clinical exam. We refer to this as seeing the unseen, and it’s really helpful for patients with macular degeneration to see if the areas of the geographic atrophy are staying the same size or if they are increasing. If the borders are stressed, that might be an indicator that it’s going to grow over time.
How I use ZEISS FORUM to analyze progression over time
One of my other must haves is a Picture Archiving and Communication System (PACS) like the ZEISS FORUM for retinal management. The Retina Workplace in ZEISS FORUM enables you to pull up past visual field test results, OCT analyses, and fundus photos, all side-by-side. This gives you the opportunity to thoughtfully analyze the impact of what all these results mean for the patient over time to determine if a patient needs treatment, and if so, what kind of treatment would be optimal.
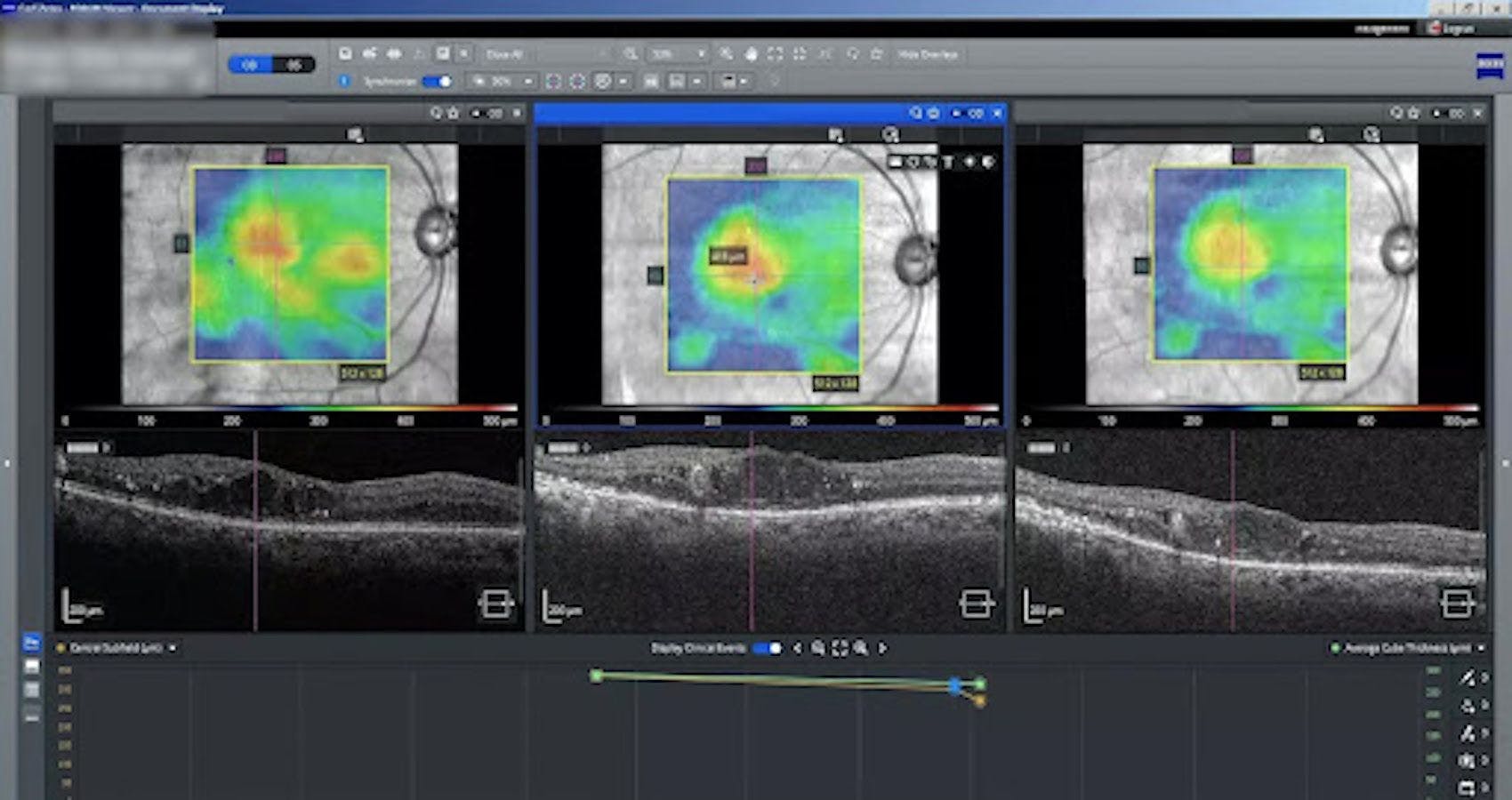
For these reasons, the ZEISS FORUM data management system is essential to determine if a patient needs treatment. One of my favorite aspects about Retina Workplace is that you can look at your cube scans, side-by-side, which are matched to location to the best ability of the device. As you scroll through a scan, you can literally be looking at three different OCT images at the same time, which is great for picking up subtle changes in the drusen and in retinal thickness. ZEISS FORUM has really made a difference in my ability to detect subtle changes over time.
B-scans can help visualize the vitreous
A final piece of equipment for retinal management which is a really nice-to-have is a B-scan, which enables you to visualize the vitreous for detachments. Looking for subtle tears can be extremely helpful, especially in the case of a proliferative diabetic patient who may have a vitreous hemorrhage. It can be challenging to examine the retina, so the ability of the B-scan to see if the retina is intact can help determine the urgency of the referral, because at the end of the day, that’s what really matters.
To refer or not to refer
The decision to monitor the disease or refer to an ophthalmologist can be one of the most overwhelming aspects of managing retinal disease. To simplify the process, I like to ask a few questions:
- What is the risk of functional vision loss based on this condition?
- Is the condition likely to progress, regress, or remain stable?
- Is the patient going to have likely progression, will that change be fast or slow?
The answer to the above questions can help determine whether or not to manage the patient yourself or refer to an ophthalmologist.
For example, if a patient comes in with peripheral vision loss and a macula-on retinal detachment, there is a very high risk of vision loss, likely progression, and potentially fast progression. Without a doubt, that’s going to be a fast referral. You will want to call your best friend retina specialist, asking them to get the patient into surgery as quickly as possible.
But let’s think about a more subtle case. If you have a patient present with acute central serous chorioretinopathy (CSCR), and it’s the first occurrence for this CSCR; the risk of vision loss is pretty low, and we expect this condition to regress on its own in about three months. In this case, I could monitor and manage that patient on my own because the overall risk of vision loss is low. I would monitor the patient monthly with OCT analysis and dynamic utilization of ZEISS FORUM’s Macular Thickness Analysis. If after three months the condition has not improved, then treatment is necessary and I would get my retina specialist involved.
Common clinical cases
Following are examples of common cases that primary optometrists will encounter in their practices. Here is a guide to give you some tips and tricks to make your life easier when you encounter these important patients in your practice.
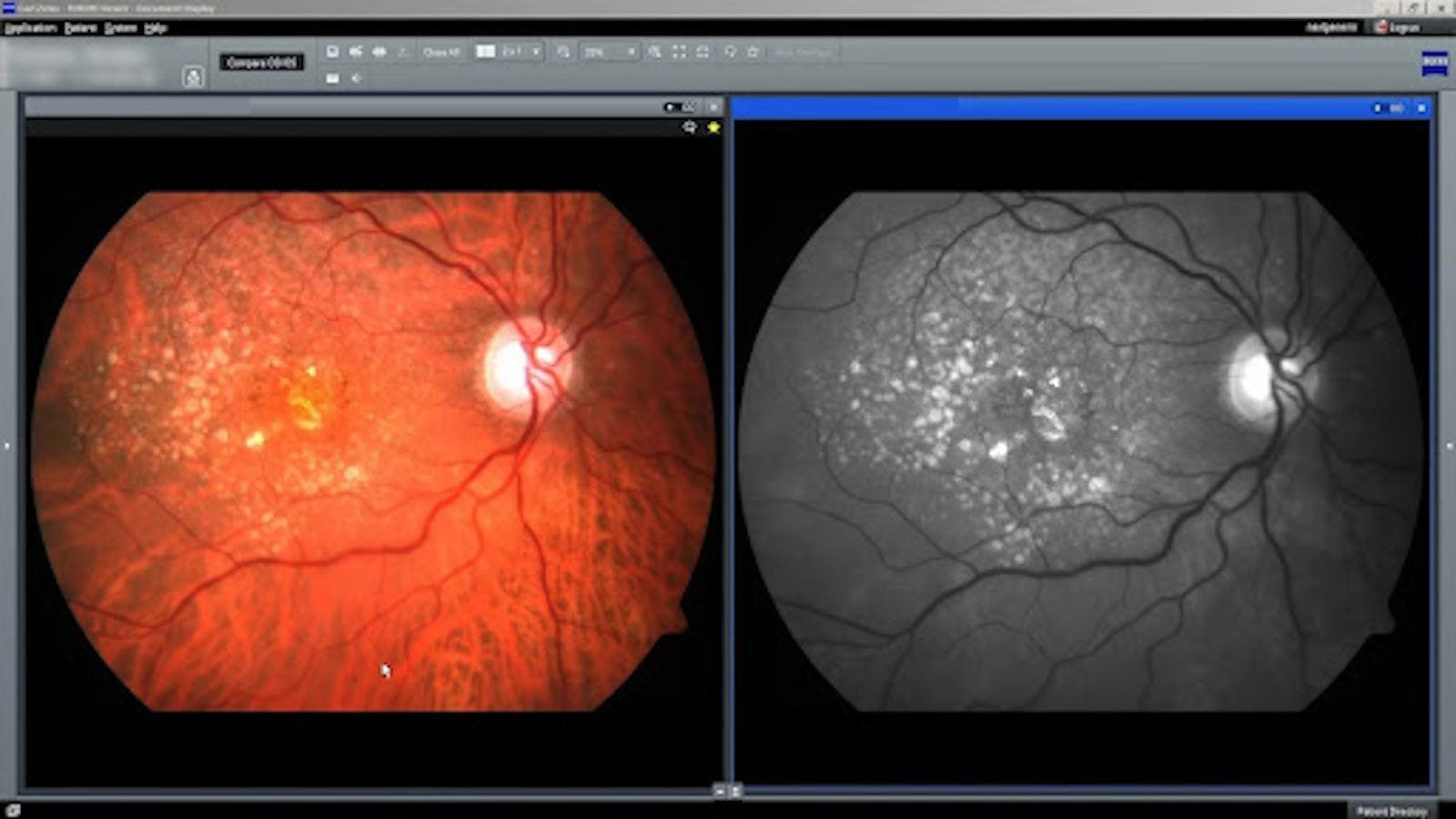
Case #1: Diabetic retinopathy
In this case we are looking at a patient's right eye to evaluate for diabetic retinopathy and diabetic macular edema.
Questions to ask yourself when evaluating diabetic retinopathy:
- What is the stage of the patient’s retinopathy?
- What are their risk factors?
- How well controlled is the systemic disease (how well can they control their HbAIc)?
- What is the likelihood of developing macular edema?
- If they have macular edema, is it affecting acuity? Does it require treatment?
- What is the risk of developing proliferative disease?
If they have proliferation, then how can that patient be treated and managed quickly?


Stage diabetic retinopathy and macular edema and look for risks of progression
- Fundus photography in a dilated fundus exam can be helpful for visualization following clinical examination. Small retinal hemorrhages can easily be overlooked during your retinal examination.
- Look for signs of previous treatment. This patient has a history of focal laser, and you can see scarring from that (two darkly pigmented spots inferior temporal the the macula). That gives us a sense that even if the patient may not remember having the treatment performed, he has a history of diabetic macular edema.
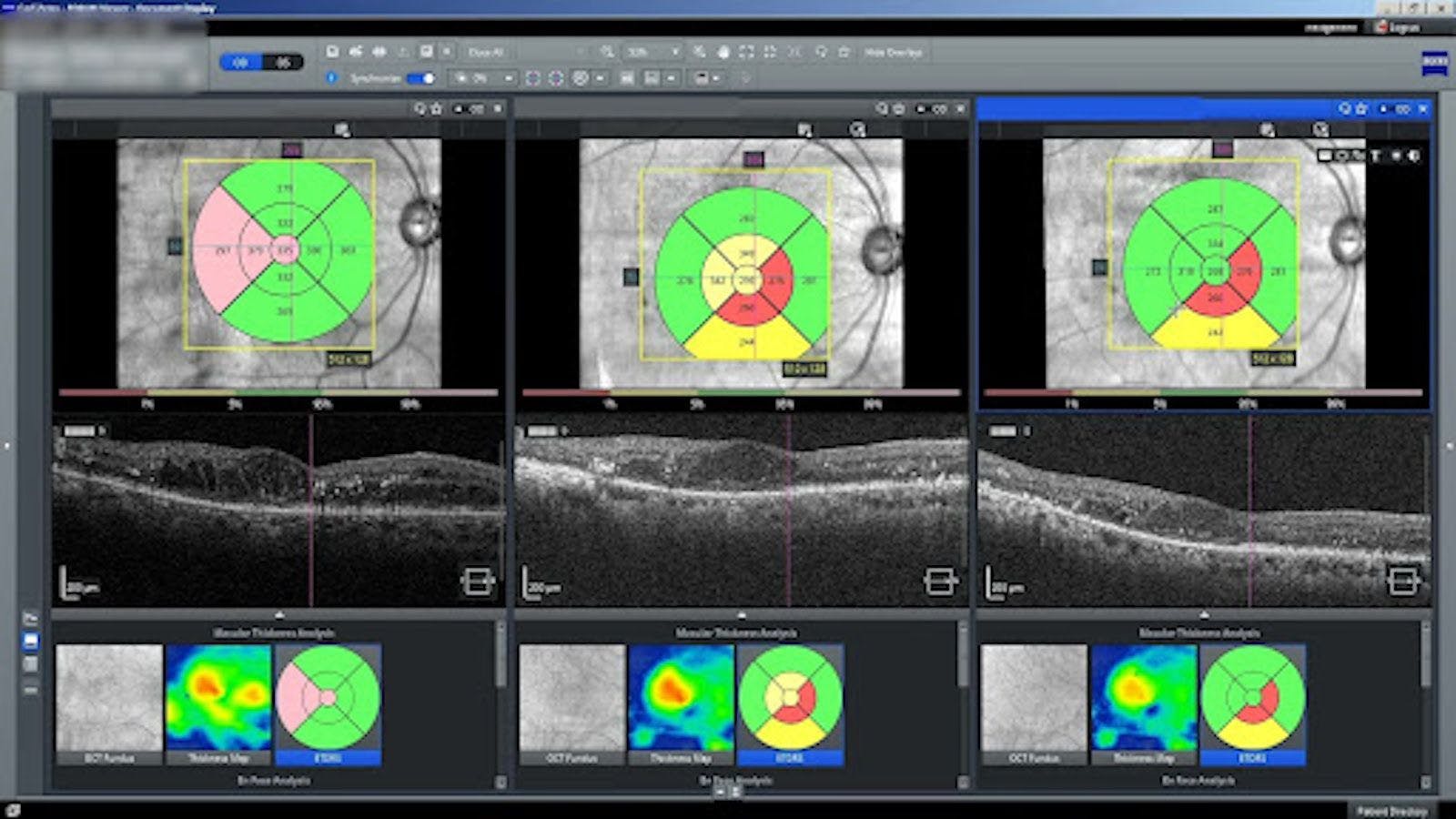
- Pay attention to the OCT images and utilize the ETDRS circles specifically while looking for the location of macular edema and thickening.
- OCTA can be helpful to identify risk of vision loss and progression of retinopathy (large areas of ischemia, early neovasculrization).

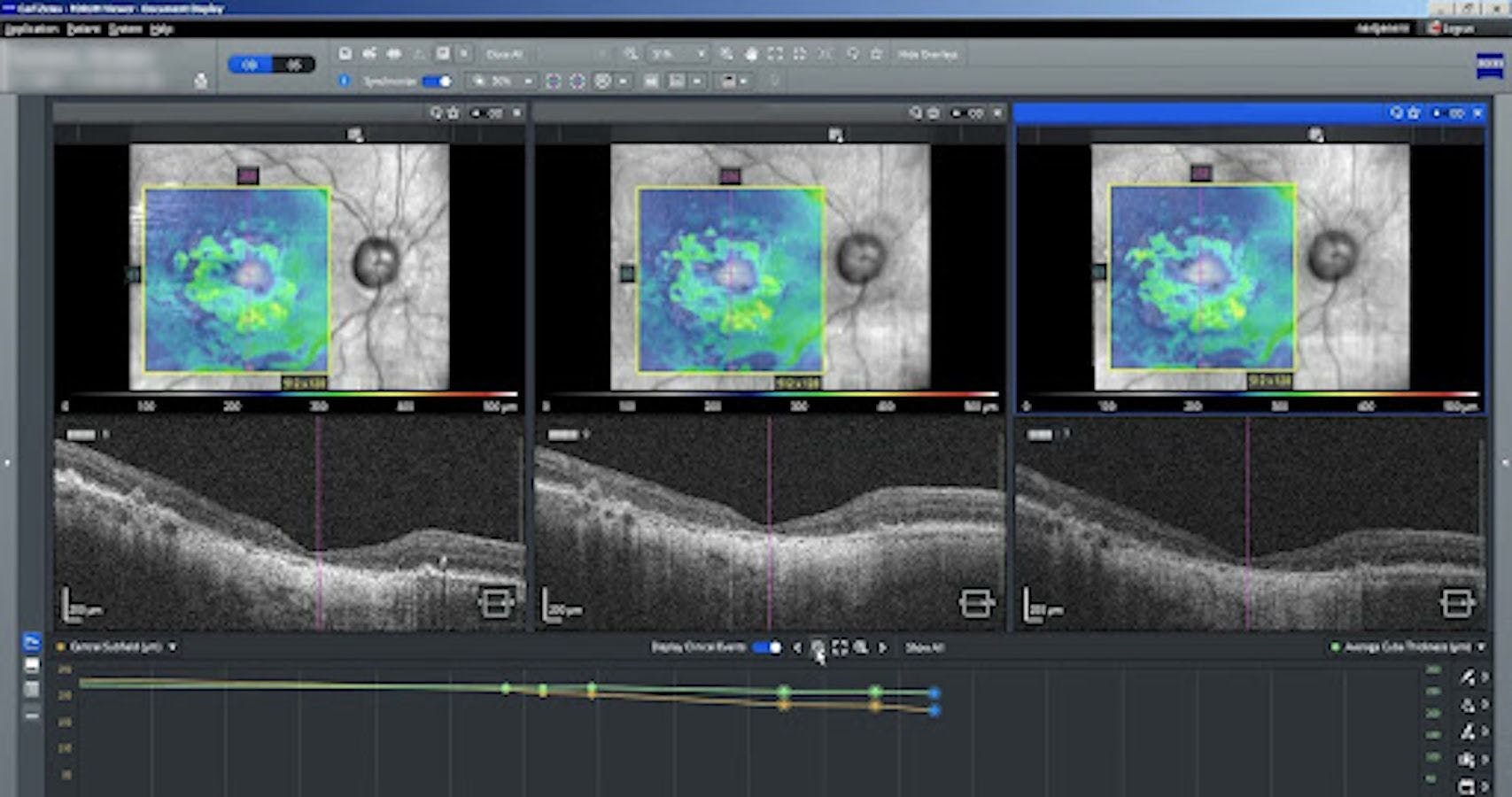
Utilize a data management tool like ZEISS FORUM to gain insight into treatment options
- Use the ZEISS FORUM for data management to analyze progression by scrolling through location matched images from multiple visits. This patient has macular edema, and the patient can see how the condition has changed over time.
- You can drop the ETDRS circle on top of the infrared fundus image to better assess diabetic macular edema. Looking at the center sub-circle,. if thickening in this area is present, the patient has center-involved macular edema and treatment with an anti-VEGF agent and potentially some focal laser are going to be warranted to improve and preserve the acuity.
- Pay attention to the patient’s best corrected visual acuity as well. We might see a mild thickening in the central ETDRS circle, but if the patient’s acuity is 20/20, that can be monitored closely by a primary care optometrist.
Resolution
In this case, the patient has significant intraretinal hemorrhages, a cotton wool spot and exudation noted on the clinical examination leading to a diagnosis of moderate non-proliferative diabetic retinopathy. We can see that the center subfield of the ETDRS circle is affected in the first and second visits leading to a diagnosis of center-involved diabetic macular edema. The center sub-field is not involved in the third visit showing non-center-involved diabetic macular edema The patient did not actually go through treatment as recommended as he was lost to follow-up. It was pure luck his edema resolved.
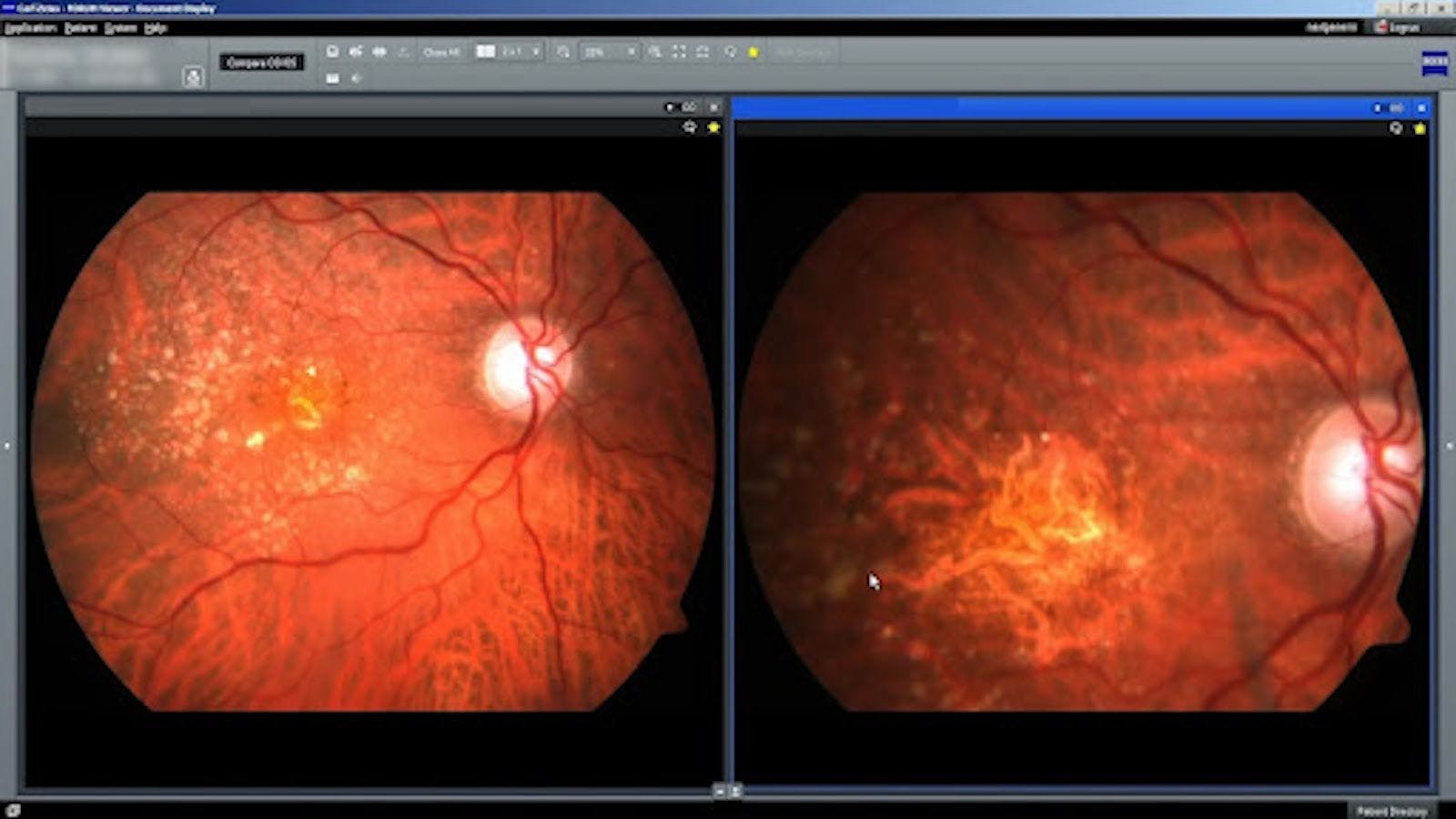
Case #2: Macular ischemia and proliferative diabetic retinopathy
In this case, we are looking at a patient’s left eye to examine for advanced diabetic changes.
Imaging diagnostics to identify diabetic retinopathy
- OCT macular thickness analysis and B-scan images will reveal areas of macular edema
- The OCTA analysis can be very helpful for highlighting microaneurysms, macular and retinal ischemia, intraretinal microvascular abnormalities, and retinal and optic disc neovascularization
- Fundus photography can he helpful for identifying peripheral hemorrhages related to diabetic retinopathy
- Fluorescein angiography can be helpful in diabetics if you are just not sure what you are seeing (IRMA vs neovascularization) and don’t have access to OCTA.
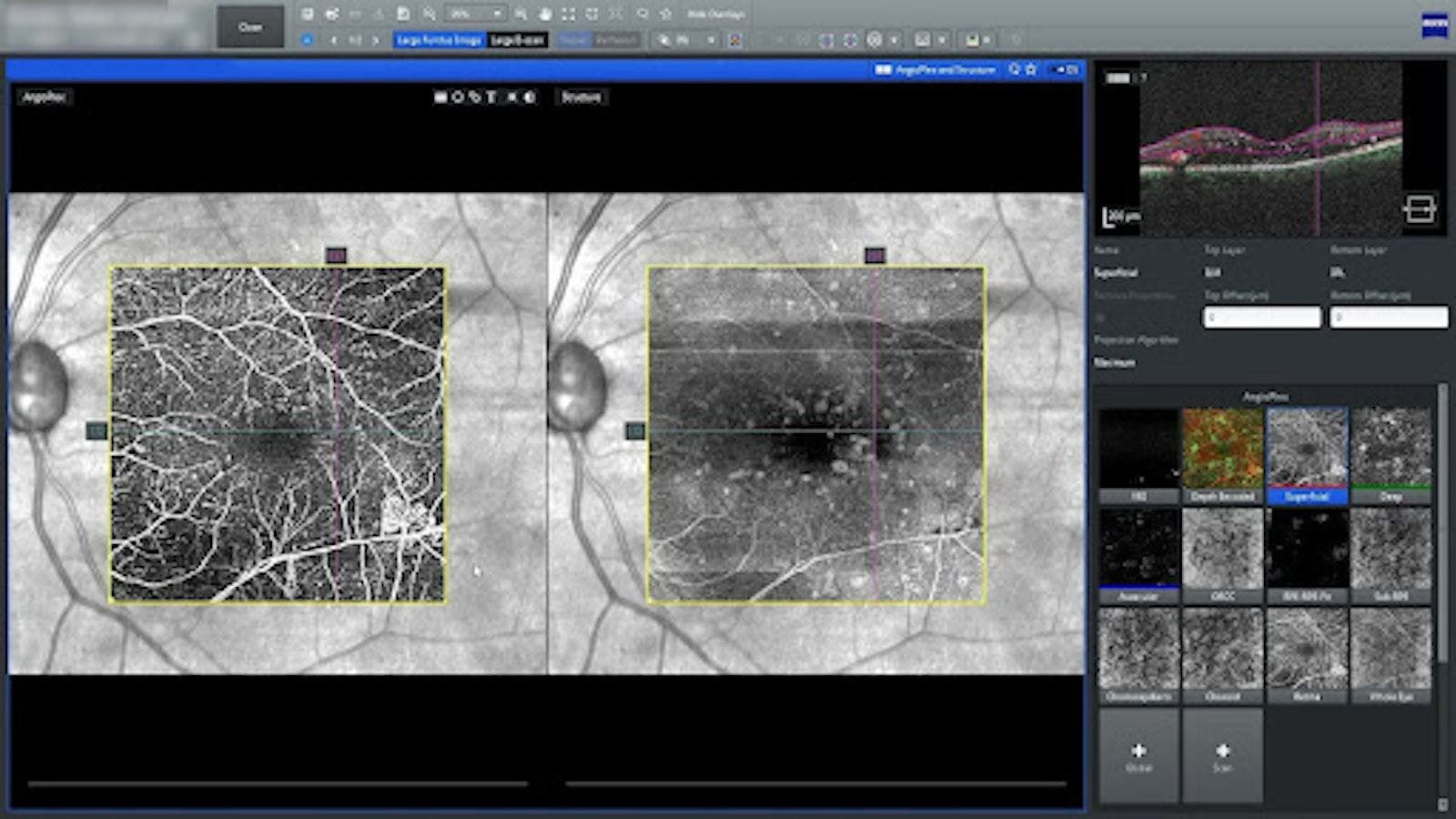
Identification of macular ischemia
One of the best places to look for macular ischemia on OCTA is in the superficial or the deep retinal segmentation. The foveal avascular zone should be about a third of the disc diameter in normal eyes and appears as a dark circle. This area irregularly expands when macular ischemia is present and can correspond to changes in acuity. In this clinical case, it has widened out, indicating mild macular ischemia.

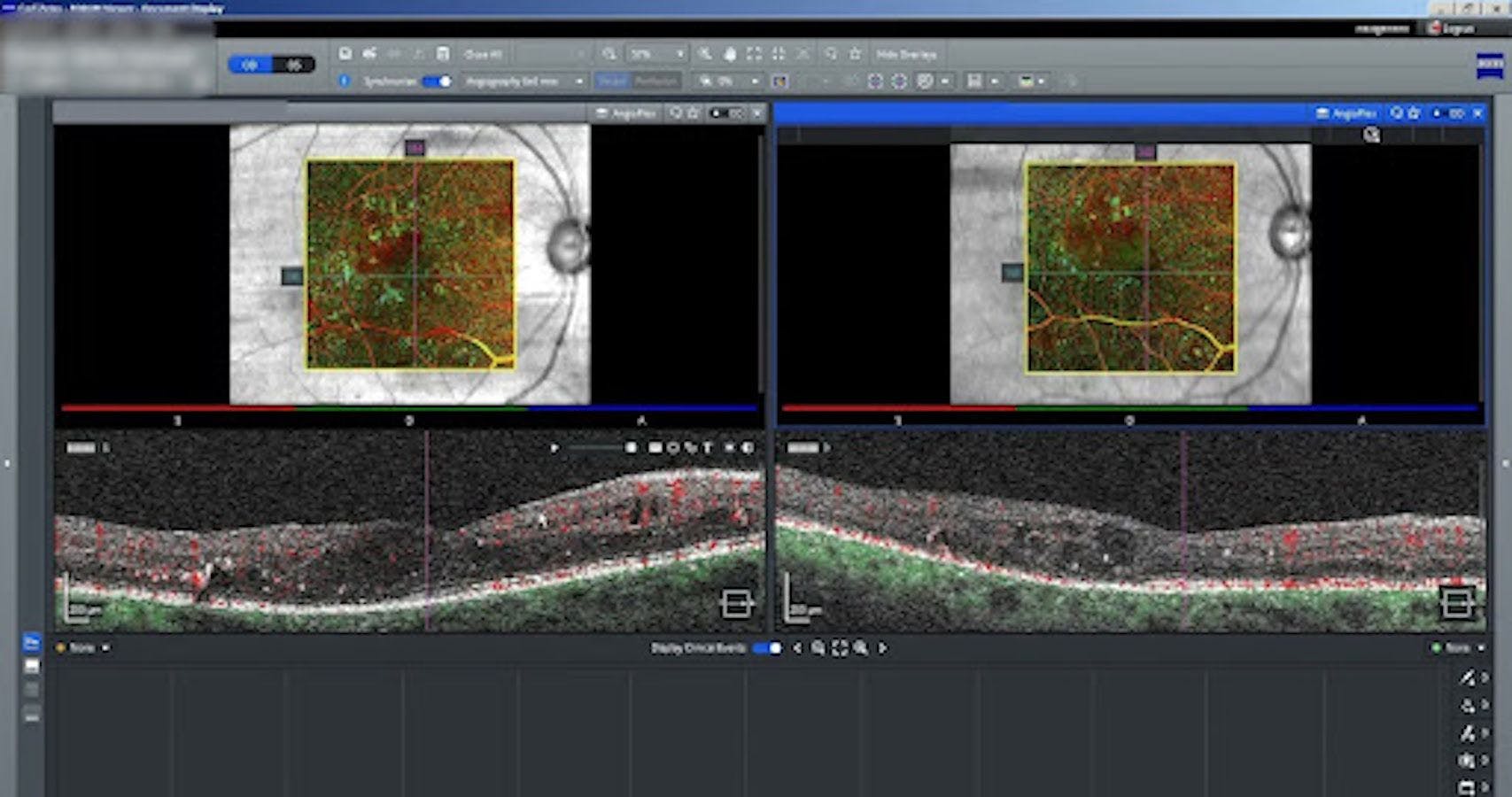
Identification of retinal and optic disc neovascularization
Using OCTA, retinal and optic disc neovascularization can be seen via the en face vitreoretinal interface segmentation. In this clinical case, you can see a flat area of neovascularization on the OCTA inferior temporal to the fovea. This is something that could easily be confused on a clinical exam as intraretinal microvascular abnormalities (IRMAs).
Resolution
In this case, it is appropriate for the patient’s acuity to be slightly less than 20/20 due to the macular ischemia. The presence of an early retinal neovascular net in the left eye raises the risk level for this patient and requires collaboration with ophthalmology. If the neovascular net was not present, the patient would still pose a moderate-high risk of progression due to the ischemia but could be monitored at a close interval for further progression.
Case #3: Macular degeneration
In this case, we are looking at a longstanding patient who has advanced macular degeneration without neovascularization. There are areas of geographic atrophy, where the choroid is clearly visible and areas of large drusen surrounding.
Family history is important when examining macular degeneration patients
- Ask about family history as genetics are incredibly important in macular degeneration cases. Genetic variances dictate the type of retinopathy you expect to see on the clinical exam and tend to have similar progression to other family members.
Utilize OCT analysis and fundus photography to differentiate and diagnose
- From a clinical perspective, macular degeneration is a posterior pole disease, so it’s important to pay close attention to the macula. OCT and OCTAare helpful to monitor retinal drusen, geographic atrophy, and detect choroidal neovascularization. These images can be compared over time to detect subtle changes that could have been missed on a clinical exam.
- Fundus photography will be very important for differentiating, diagnosing, and documenting. They are also helpful in monitoring over time and patient education.
Questions to ask when looking at images in macular degeneration patients
- Do they just have drusen?
- Do they have atrophy?
- Do they have neovascularization?
- Is there progression from previous exams?
In this case, using fundus photography, you can see that the area of geographic atrophy vastly increased over the four-year span between the two different photos. Red-free and fundus autofluorescence images (not shown) can be helpful as that can help you identify where the geographic atrophy is and see the drusen with a slightly different perspective.
OCT is an important tool to monitor drusenoid and atrophic changes and to see early evidence of neovascularization. The Macular Thickness Analysis in ZEISS FORUM data management software can help you assess the macular thickness over time, by analyzing multiple images at once.
By adding images from multiple visits, you can get a sense if you have change for the patient. In this case, you can see that the patient has a significant amount of drusen in the outer retina. You can also identify areas of choroidal atrophy, and the geographic atrophy that are increasing over time. This progression of the geographic atrophy is easily noted by enhanced illumination down into the choroid because of the absence of the overlying retinal pigment epithelial (RPE). Using these imaging techniques, it’s easy to see that the area of atrophy area is increasing over time.
Unfortunately, this patient’s acuity went from 20/60 in the first visit to 20/400 currently. Generally with macular degeneration as you see an increase in the amount of atrophy, the amount of drusen will decrease. This can be easily evaluated by utilizing ZEISS FORUM’s Advanced RPE Analysis. This analysis provides visualization and quantification of two different measurements that are important in non-exudative Macular Degeneration:
- RPE elevation within either a 3mm or 5mm circle, this corresponds to retinal drusen. This is shown as on the overlay in light blue.
Sub-RPE illumination, this corresponds to areas where the RPE is missing indicating geographic atrophy. The border of these areas is highlighted on the overlay with a while line.
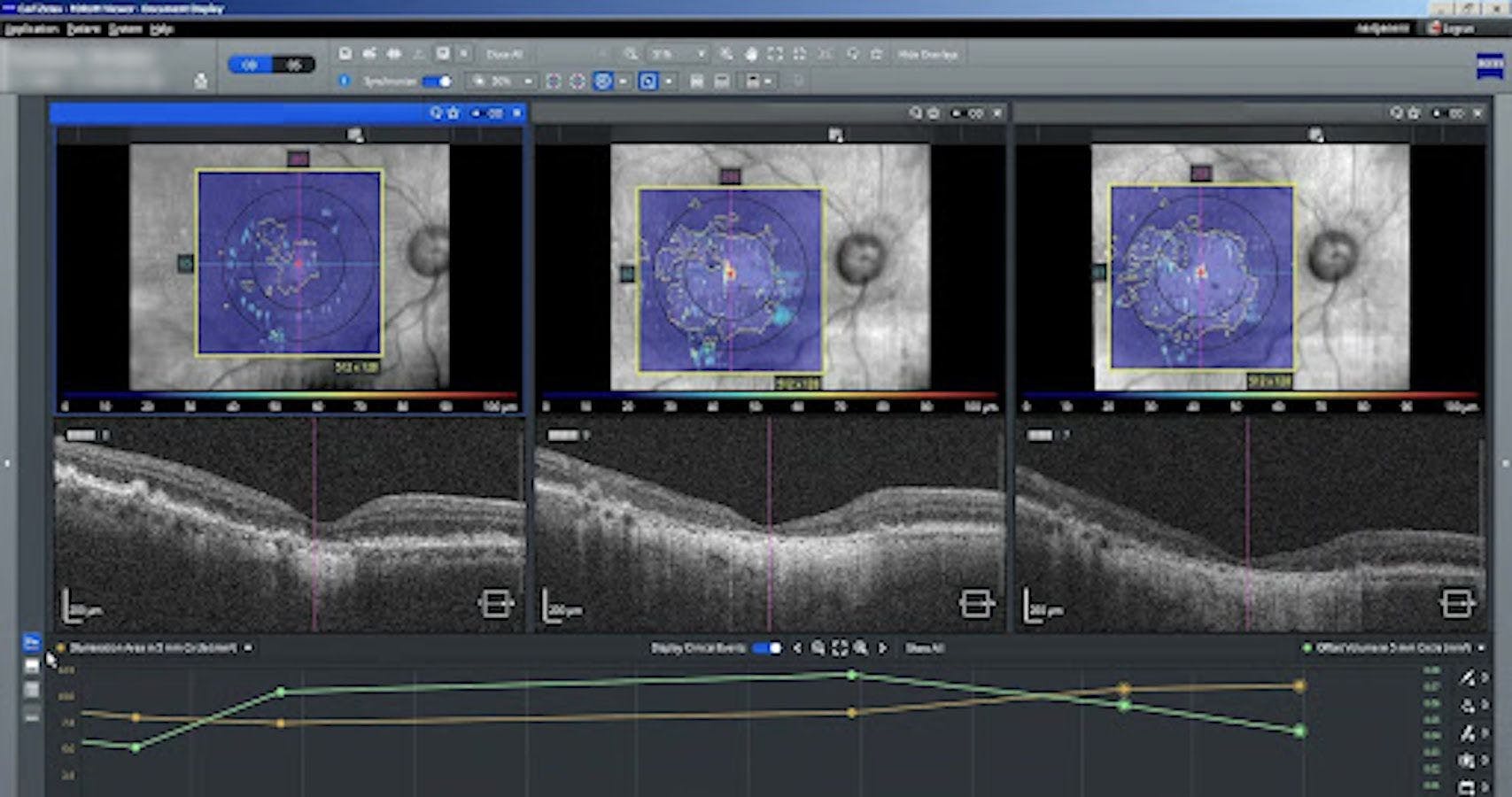
I recommend using the RPE elevation overlay as a guide to help identify areas of drusen when you are reviewing OCT scans. This can save time so that you are not having to dig fully through OCT images themselves to look for these small outer retinal changes. Areas of geographic atrophy (sub-RPE illumination) are encircled in the overlay. This visualization and the associated area measurements can be very helpful for detecting progression of geographic atrophy.
Resolution
In this case, using Advanced RPE analysis it’s easy to visualize that the patient has had significant progression of his geographic atrophy over the years corresponding with a large decrease in visual acuity. The patient has not had any evidence of choroidal neovascularization throughout the years so the change in acuity is attributed to advanced dry macular degeneration with central geographic atrophy.
Typical Exam Flow for a Patient With Degenerative Myopia
In order to visualize a typical exam flow when managing patients with retinal, I’d like to walk through an example of a patient with degenerative myopia, as this is a very prevalent condition. We’re seeing many more degenerative myopes, and it’s important to know how to care for these patients as a primary care optometrist.
The first step is to think about risk factors. For degenerative myopic patients, it’s important to think about family history. To begin, I might ask my patient the following questions, starting with family history:
History questions to ask:
- Who else in the family had myopia? Did they have one myopic parent or two?
- How high of a myope were the family members?
- Did their parents have any history of retinal tears or retinal detachments? Did anyone else in the family?
- Have they ever experienced any trauma to their eyes?
- What are the patient’s symptoms? Do they have any flashes of light or floating spots in their vision?
It’s also important to determine the axial length when dealing with myopes. The higher the axial length, the greater the risk of a patient having long term vision loss from their degenerative myopia. This test can be performed with biometry, specifically the ZEISS IOLMaster. If the axial length is over 26, that patient is at a much higher risk of developing sight-threatening myopic degenerative issues later in life.
Most effective clinical exam steps for degenerative myopia patients
Next, it’s important to understand the best corrected visual acuity by performing a refraction. I believe it’s imperative when taking care of any of our patients who have retinopathy or are a retinopathy suspect, because we want to understand what change in vision is coming from the retina as well as what’s coming from the cornea and lens versus refractive error. A good refraction is always step one in managing any retina patient.
Then, it’s essential to perform a dilated fundus examination. It’s important to get a good dilation in order to examine the periphery, because degenerative myopes are going to potentially have issues in the peripheral retinal as well as in the posterior poles. We can look at that thoroughly with a binocular indirect examination.
Which equipment can give you the most information about degenerative myopes?
After we look at the patient, if there is something unusual in the retina, we will want to document that or use diagnostic imaging to better assess and monitor the patient over time. In this case, widefield fundus photography can be very useful when documenting a peripheral retinal lesion you found. It’s also helpful to utilize fundus photography to document any posterior pole findings.
Degenerative myopes tend to have large staphylomas which can lead to retinal thinning, choroidal thinning, and increase the risk of neovascularization. If any of this pathology is clinically seen in high myopes, OCT analysis can provide incredible insight into the extent of the damage the patient has due to the thinning and other retinal issues potentially occurring. OCT is also helpful to view those different changes and analyze change over time.
Another great utilization for OCT is to visualize myopic macular schisis. Luckily in most cases, patients do not experience any impact to their vision. Myopia macular schisis is something that can be monitored by primary care optometrists because there’s typically no treatment other than a vitrectomy—which is not typically warranted because of the risks associated with that procedure.
How to use OCT images for degenerative myopia patients
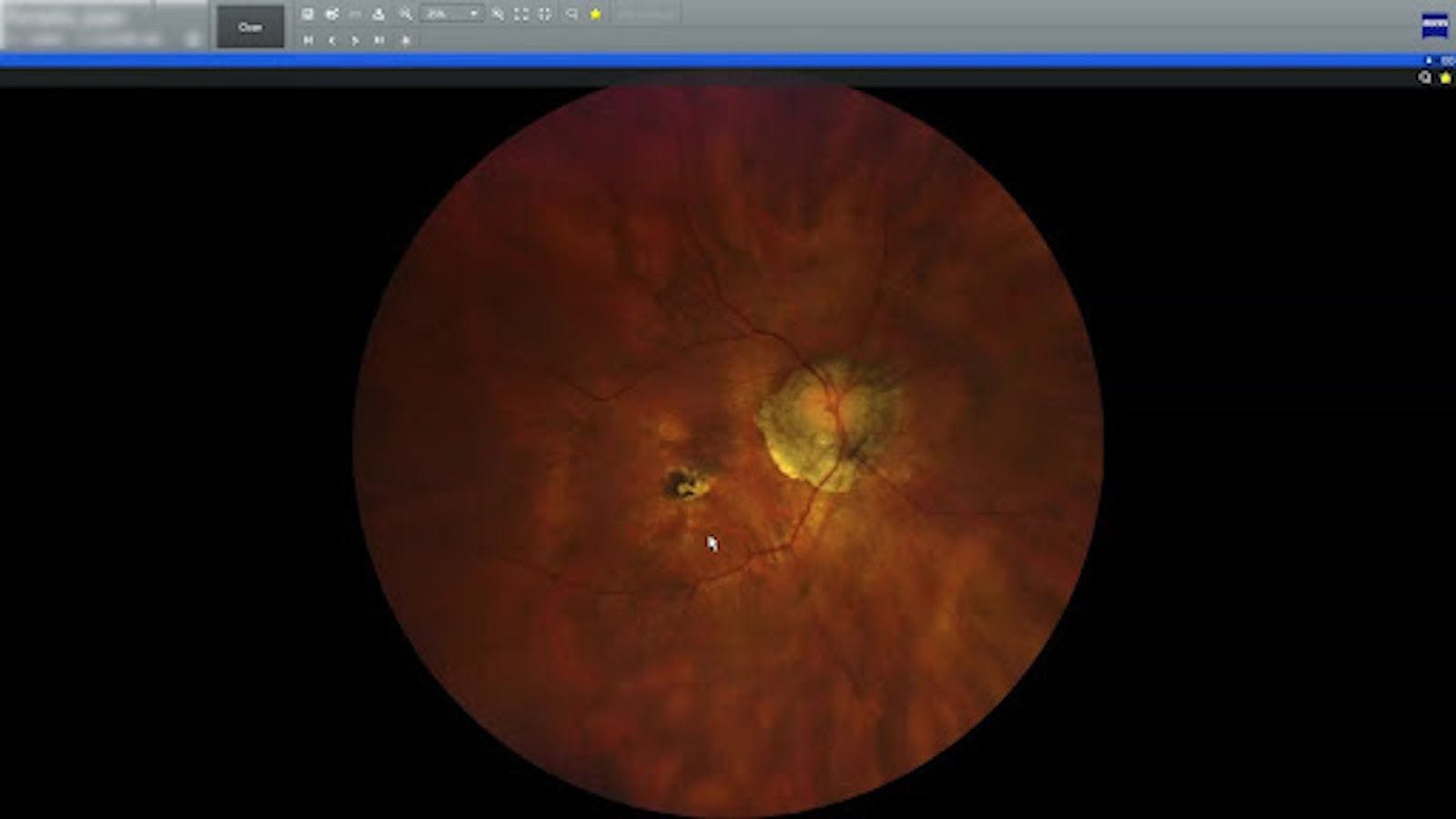
In the example above, you can see a very prominent scleral crescent, which is typical of degenerative myopic patients. You will notice some temporal dragging of the vasculature due to the elongation of the eye and the staphyloma within the back of the eye. You will also notice a Fuchs spot and some nearby choroidal atrophy.. Fuchs spots are very important because you get a sense that the patient had a past history of choroidal neovascularization. We can consider this retina to be ischemic. In this case, OCT can help you visualize the atrophy, ischemia, and old CNVM a bit more clearly.
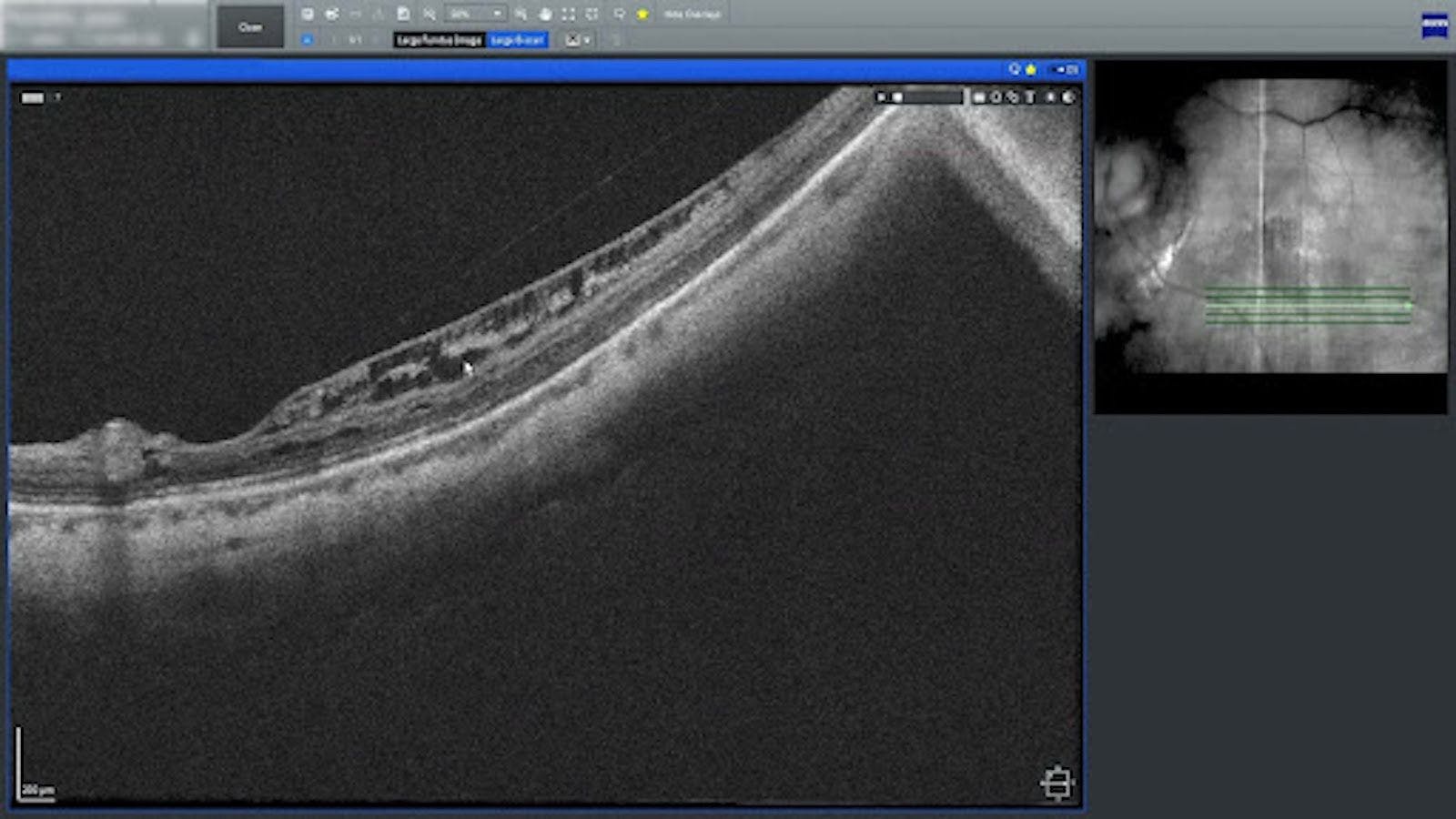
Another retinal finding that is important is myopic macular schisis. In this case, we can see a splitting of the layers within the inner retina. Fortunately, this doesn’t lead to much vision change, and you can’t even see it in your clinical exam. It’s only able to be seen with OCT analysis, which demonstrates the power of this technology. Some patients will have some flashes of light with this condition because the vitreous does pull on the retina, which can lead to some flashes, so some patients may become symptomatic when they have myopic macular schisis.
What are the risks of vision loss and the likely rate of progression in degenerative myopes?
The next step is to determine how quickly this condition is going to change. And if it’s going to change, is it going to be fast or slow? If you have a degenerative myopia patient with a retinal detachment that obviously has a very high risk of long term vision loss, that patient should be referred immediately to a specialist.
But if you have a degenerative myope with a macular hole and it’s a recent onset, then this is something that if managed quickly and correctly, can have a better visual outcome. This patient should also be referred, but it’s not necessarily an urgent referral to an ophthalmologist. In the case of a myopic macular schisis, that can be monitored by a primary care optometrist as visual impact is generally low.
Decisions you need to make when managing degenerative myopia patients
If you have a low risk of vision change, a low risk of a condition progressing, and if it does progress, the progression rate is slow, then that is a patient who can be monitored on a three to six-month basis, depending on how close to the macula the condition is and what the impact is on best corrected acuity. Really, at the end of the day, our job is to make sure we control our patients and make sure we manage the risks to protect them from long term vision change.
If we think about this, the best way for degenerative myopes is to avoid vision loss is to prevent degenerative myopia completely. This means that we are rigorous about managing myopia early on to slow myopic progression.
Summary
Due to the vast quantity of ocular and systemic conditions that can affect the retina, managing patients with retinal disease can be overwhelming. Multimodal imaging and advanced imaging assessment tools are extremely helpful to make managing these retinal conditions more manageable for medical optometrists. By evaluating risk factors, understanding disease prognosis and risk, and combining advanced imaging analysis, we can make decisions to help preserve the vision of our patients and enhance collaboration for advanced care.
