


A 67 year old Indian female presented complaining of increasing difficulty reading at near, worsening during the past 2 years. Her previous examination was 3 years ago with an outside provider who had performed cataract surgery in both eyes. She reported that the cataract surgery significantly improved the vision but then her vision continued to worsen, although it was still considerably better than presurgical levels. She had been diagnosed with hypertension (last blood pressure 138/78 mmHg) and type 2 diabetes (last HbA1C 6.4%) 6 years prior. Both were well controlled with lisinopril and metformin, respectively.
Pertinent Findings
Entering distance acuities were 20/30 in the right eye and 20/25- in the left eye with an essentially plano prescription. Near acuities were similar: 20/30- in the right eye and 20/25-2 in the left eye with a +2.50 near add. External examination was unremarkable. Aside from healed corneal cataract incisions and the presence of clear and centered posterior chamber intraocular lenses in each eye, the anterior segment was unremarkable. Dilated fundus examination revealed mild foveal yellowing/pigmentary changes in each eye. A single druse was noted inferonasal to the fovea in the right eye.
OCT imaging of the macula was ordered to assess the pigmentary changes. Small inner retinal ovoid hypo-reflective spaces were noted in each fovea. The cavitations were more prominent on the temporal side of the fovea and were not associated with retinal thickening. Mild disruptions of the retinal pigment epithelium and ellipsoid zone corresponded to the pigmentary changes noted with funduscopy.

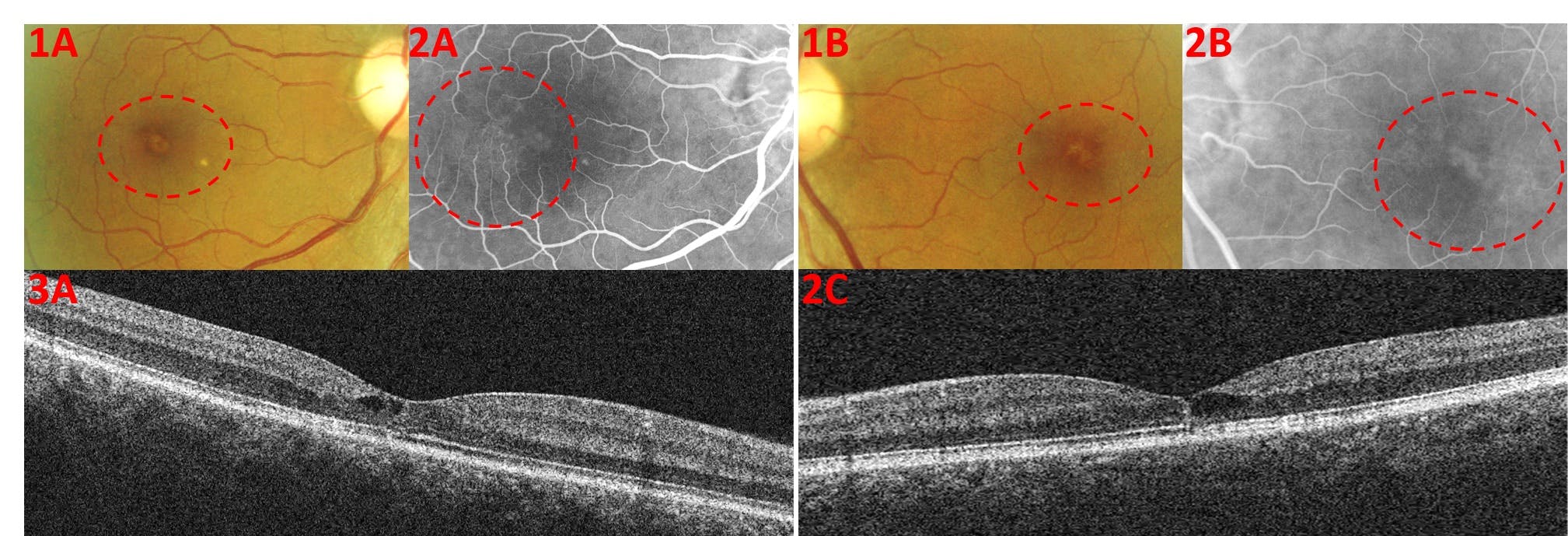
1A/1B: Fundus photographs of foveal RPE changes/pseudo-vitelliform lesion
2A/2B: Diffuse temporal hyperfluorescence noted on fundus autofluorescence reveals
3A/3B: OCT reveals inner retinal cavitations and mild ellipsoid zone/RPE disorganization
A fluorescein angiogram was performed to assess the retinal vasculature. Mild diffuse hyperfluorescence, mostly confined to the temporal macula, was noted in each eye. The retinal cystic-like cavitations, noted on OCT, did not show any fluorescein pooling with angiography.
Diagnosis and Treatment
The main diagnosis considered in this case was macular telangiectasia type 2 due to the characteristic inner retinal cavitations noted on OCT. Because the patient was diabetic, diabetic macular edema was considered in the differential; however, unlike retinal cysts associated with diabetic macular edema, there was no noted retinal thickening, hemorrhaging, or hard exudates. The fluorescein angiogram confirmed the diagnosis when no significant angiographic signs outside the macula were noted. Other disorders such as branch/central retinal vein occlusions and age related macular degeneration were considered but ultimately ruled out due to the lack of corresponding clinical and imaging findings.
The patient was apprised of all findings and the slowly progressive nature of the disease was discussed in length. The patient was educated on the use of an Amsler grid to self-evaluate her vision and a four-month re-evaluation was scheduled.
Discussion: Macular telangiectasia type 2
Macular telangiectasia type 2 is a primary neurodegenerative maculopathy characterized by bilateral atrophy and subsequent vasculopathy most prominent in the temporal macula. The average age of diagnosis is 57 years old and even though the disease is slowly progressive, most patients will retain good vision in the 20/32-20/50 range.1 Due to the paracentral changes and resultant scotomas, reading ability seems to be affected out of proportion to visual acuity testing. The primary cause of macular telangiectasia type 2 is still unknown, but Muller cell dysfunction is considered to be an early pathological finding.
Early funduscopic changes include blunting of the foveal reflex, reduced retinal transparency (retinal graying), and blunted or right-angle venules. As the disease progresses, vascular telangiectasias, crystalline deposits, retinal pigment hyperplasia, and retinal atrophy will develop. Rarely, retinal neovascularization or foveal pseudo-vitelliform lesions may form. Before these clinical findings manifest, temporal diffuse fluorescein angiography hyper-fluorescence and temporal macular pigment loss may be noted. OCT imaging reveals distinctive inner retinal cavitations, outer retinal disorganization, and macular thinning (in nonproliferative cases). Aside from the loss of the foveal reflex, these findings are usually more prominent on the temporal side of the macula but often encompass the whole fovea as the disease progresses.
Though macular telangiectasia type 1 and 2 are similarly named and both possess macular telangiectatic vessels, they are quite different in their disease manifestations. Where macular telangiectasia type 2 presents with discrete bilateral macular neurodegeneration without exudation, macular telangiectasia type 1 most often presents unilaterally with aneurysmal changes, exudation, and retinal thickening. Type 1 disease, though frequently confined to the macula, can also be found further out within the posterior pole and rarely in the periphery. The strong male and unilateral predilection of this condition has led many to believe that macular telangiectasia type 1 may be a macular phenotype of Coats Disease.2
Macular telangiectasia type 3 was defined as a progressive bilateral macular occlusive disease which was sometimes associated with central nervous system vasculopathy. Due to its rarity and lack of telangiectatic vessels, macular telangiectasia type 3 was removed from the classification system by Yanuzzi et al.2

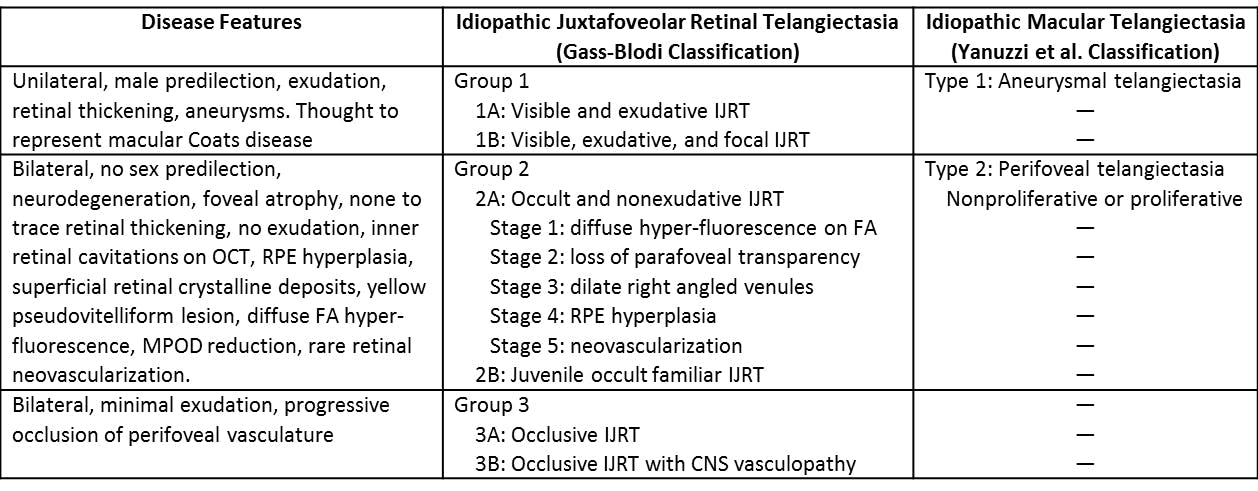
- IJRT: idiopathic juxtafoveolar retinal telangiectasia
- OCT: optical coherence tomography
- RPE: retinal pigment epithelium
- FA: fluorescein angiogram
- MPOD: macular pigment optical density
- — Denotes removed classification
Unfortunately, there is no accepted treatment for the nonproliferative form of macular telangiectasia type 2. Since macular pigment optical density was noted to be reduced in these patients, a pilot study of carotid supplementation was completed.4 This small study showed possible stabilization of vision and improvement of retinal architecture as denoted by OCT. Another treatment paradigm for macular telangiectasia type 2 hopes to harness the neuroprotective effect of ciliary neurotrophic factor. Chew et al. demonstrated that delivery of ciliary neurotrophic factor delivered into the vitreous cavity via a surgical implant can significantly slow down neurodegeneration and vision loss.5 Due to the slow course of macular telangiectasia type 2, additional longer studies will need to be carried out before this treatment can be widely used. The proliferative form of macular telangiectasia type 2 is treated like exudative age related macular degeneration, with various anti-VEGF therapies or photodynamic therapy.
Macular telangiectasia type 2 is a difficult disease to diagnose clinically, especially in its earlier stages. Checking for characteristic OCT findings and ruling out common conditions such as age related macular degeneration and diabetic macular edema can help establish the correct diagnosis. Though there is no accepted treatment for the nonproliferative form of macular telangiectasia type 2, patients must be counseled on self-assessing their vision to prevent profound vision loss from the treatable, proliferative form.
In a Nutshell
- Macular telangiectasia type 2 is a bilateral neurodegenerative condition characterized by telangiectatic vessels, loss of retinal transparency, superficial retinal crystals, RPE hyperplasia, and rarely retinal neovascularization most prominent on the temporal half of the macula
- OCT findings have characteristic inner retinal cavitations without exudation or retinal thickening
- Most patients retain good visual acuity, but reading ability may be affected more than distance visual acuity would suggest
- There is no treatment for the nonproliferative form. The proliferative form can be treated with intravitreal injections, laser photocoagulation, or photodynamic therapy
References
- Clemons, Traci E., et al. "Baseline characteristics of participants in the natural history study of macular telangiectasia (MacTel) MacTel Project Report No. 2." Ophthalmic epidemiology 17.1 (2010): 66-73.
- Yannuzzi, Lawrence A., et al. "Idiopathic macular telangiectasia." Archives of ophthalmology 124.4 (2006): 450-460.
- Gass, J. Donald M., and Barbara A. Blodi. "Idiopathic juxtafoveolar retinal telangiectasis: update of classification and follow-up study." Ophthalmology 100.10 (1993): 1536-1546.
- Tan, Anna CS, Chandrakumar Balaratnasingam, and Lawrence A. Yannuzzi. "Treatment of macular telangiectasia type 2 with carotenoid supplements containing meso-zeaxanthin: a pilot study." Ophthalmic Surgery, Lasers and Imaging Retina 47.6 (2016): 528-535.
- Chew, Emily Y., et al. "Effect of ciliary neurotrophic factor on retinal neurodegeneration in patients with macular telangiectasia type 2: a randomized clinical trial." Ophthalmology 126.4 (2019): 540-549.
