



Vital dyes, stains used in living cells, have become an indispensable tool in science and medicine. This article will explore the historical nature of vital dyes and their usage in eyecare, providing an overview of each dye used to diagnose and/or manage ocular disease, with a colorful downloadable cheat sheet.
Brief overview of dye staining
It is believed that Nicolás Monardes first described fluorescence in the sixteenth century when he noted the luminous qualities of a wood extract from the Lignum nephriticum tree.
With the emergence of the synthetic dye industry, Adolf von Bayer (of the Bayer aspirin fame) swiftly synthesized the first fluorescent dye, fluorescein, in 1871. Then, 9 years later, Paul Ehrlich used the fluorescent dye uranin (a sodium salt of fluorescein) to identify the aqueous humor pathway, marking the first time a fluorescent dye was used in animal physiology.1
Surgical procedures using vital dyes
There are numerous ocular surgical procedures that rely on vital dyes to stain targeted structures or tissues.
Angiography
Vital dyes are administered intravenously (IV) during angiography, as a diagnostic aid, illuminating the retinal vasculature and tissues.
Cataract surgery
Being able to differentiate certain structures is essential in cataract surgery, especially in difficult cases with low contrast, such as with white or traumatic cataracts. To assist the surgeon, dyes target the key features of the anterior capsule and the anterior vitreous.2
Chromovitrectomy
The use of vital dyes in the surgical treatment of vitreoretinal diseases is chromovitrectomy, with procedures that can include:3
- Anterior and posterior/pars plana vitrectomy
- Epiretinal membrane (ERM)/internal limiting membrane (ILM) peel
- Macular hole repair
- Retinal detachment repair
During chromovitrectomy, vital dyes enable surgeons to better visualize the semitransparent intraocular membranes. For vitreoretinal surgery specifically, targeted tissues, mainly the vitreous, ILM, and the ERM, can be highlighted by selective dyes.4
Glaucoma surgery
Staining in glaucoma surgery helps to:2
- Evaluate the patency and leakage of glaucoma filtering blebs
- Color pharmacologic agents, such as mitomycin C and 5-fluorouracil, for precise placement.
Download the Guide to Vital Dyes for Optometrists below!
📖
A Guide to Vital Dyes for Optometrists
Featuring detailed clinical images, this cheat sheet reviews the characteristics and indications of various vital dyes used in eyecare as well as clinical pearls for assessing patients with these dyes.
Topical dyes
Fluorescein sodium (NaFl) dye
Even though fluorescein was discovered and used in the late 1800s, it did not become popular until the inclusion of blue-violet-ultraviolet (UV) light-filtered illumination on slit lamps.
Fluorescein has since taken over as the most used ocular surface stain.2 This very fluorescent xanthene dye can be made into at least 50 different derivatives, with fluorescein sodium (NaFl) being the most extensively used in eyecare.
NaFl stains:5
- Healthy cells
- Damaged or dead cells
- Intracellular spaces
- Tear film
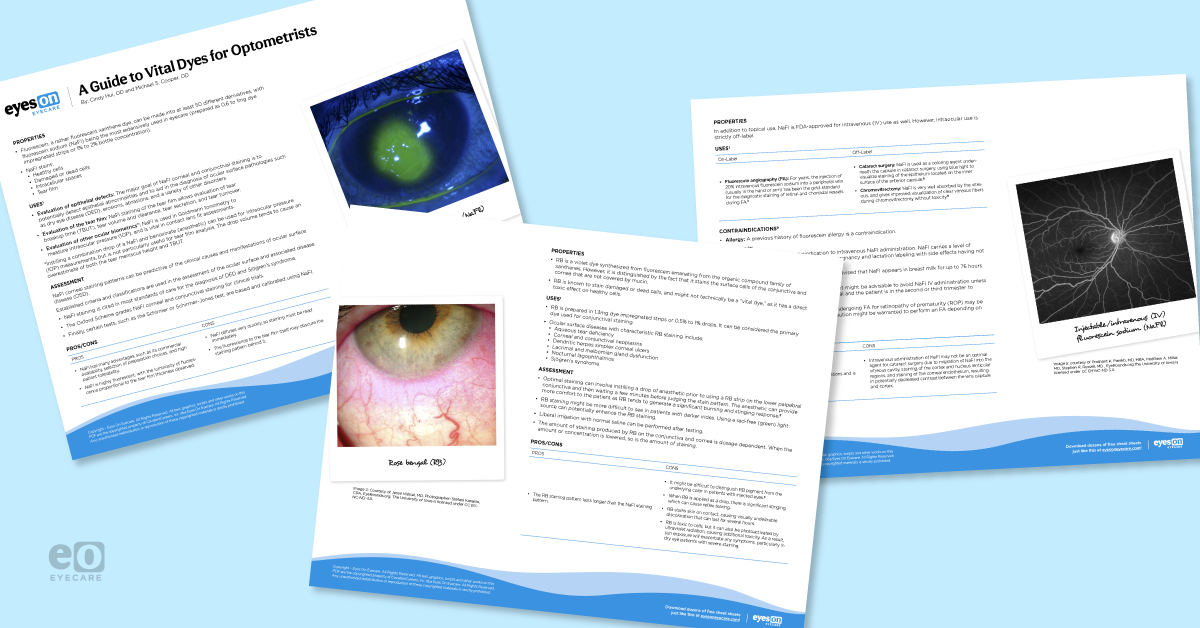
Figure 1 features a closeup of fluorescein sodium dye on a patient's eye to evaluate their ocular surface health.

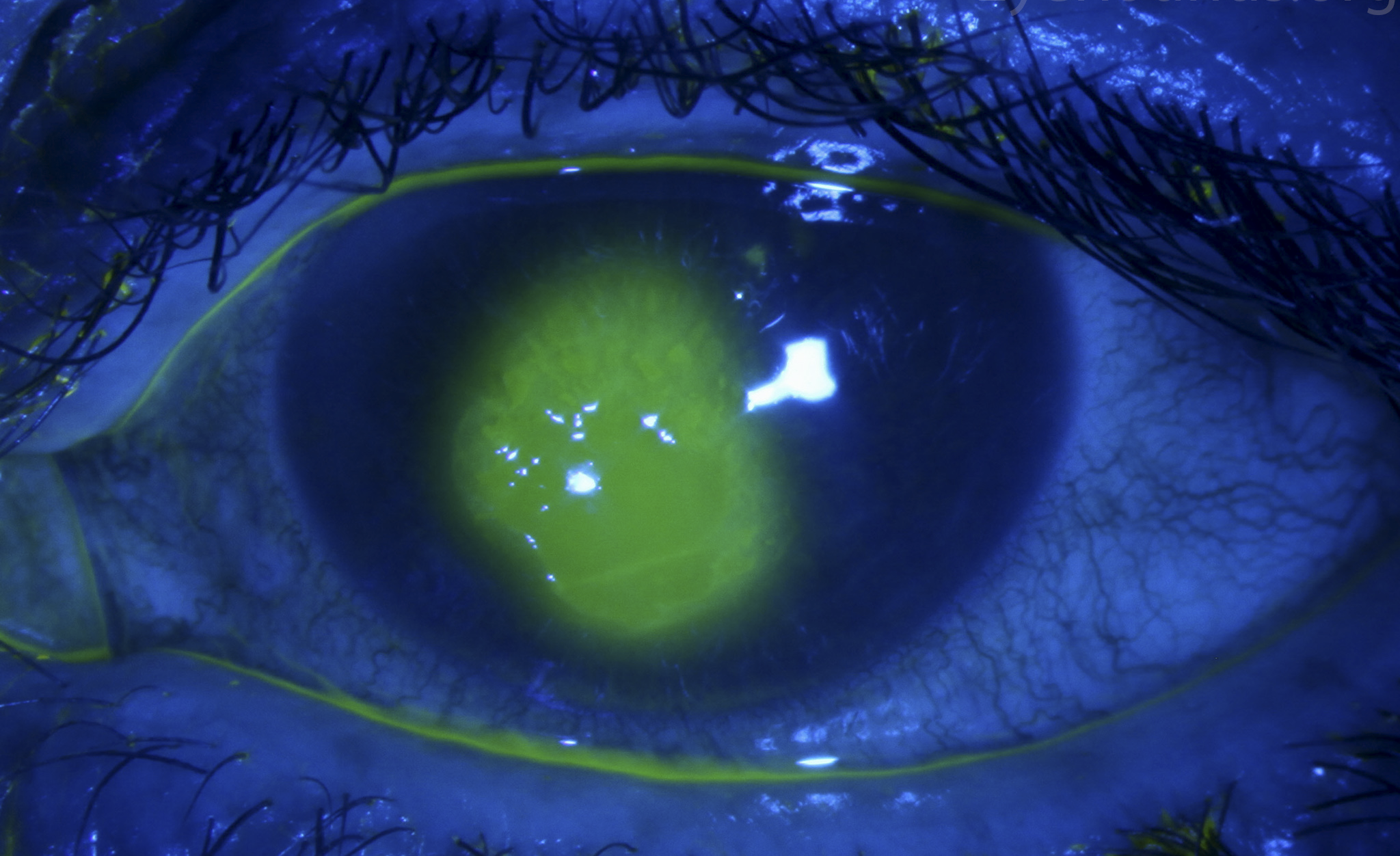
Figure 1: Courtesy of Jesse Vislisel, MD.
Uses for fluorescein sodium dye
Fluorescein sodium can be used to evaluate several conditions, including epithelial defects, tear film, and ocular biometrics.6
- Epithelial defects: The major goal of NaFl staining in the cornea and conjunctiva is to detect epithelial abnormalities and to aid in the diagnosis of ocular surface pathologies such as dry eye disease (DED), erosions, abrasions, and a variety of other disorders.
- Tear film: NaFl staining of the tear film allows evaluation of tear break-up time (TBUT), tear volume and clearance, tear secretion, and tear turnover.
- Ocular biometrics: NaFl is used in Goldmann tonometry to measure intraocular pressure (IOP), and is vital in contact lens fit assessments.
Assessment using fluorescein sodium dye
NaFl corneal staining patterns can be predictive of the clinical causes and manifestations. The Oxford Scheme grades corneal and conjunctival NaFl staining for clinical trials. Established criteria and classifications are used in the assessment of the ocular surface and disease.
For example, NaFl staining is cited in most standards for the diagnosis of dry eye disease (DED) and Sjögren’s syndrome. Finally, certain tests, such as the Schirmer or Schirmer-Jones test, are based on and calibrated using NaFl.7
Pros/cons of NaFl dye
- Pros: NaFl has many advantages, such as its commercial availability, selection of preparation choices, and high patient tolerability. In addition, NaFl is highly fluorescent, with the luminosity of fluorescence proportional to the tear film thickness observed.8
- Cons: One of the biggest drawbacks to NaFl is that it diffuses very quickly, so staining must be read immediately. Another downside is that the fluorescent tear film itself may obscure the staining pattern behind it.8
Rose bengal (RB) dye
Rose bengal (RB) was first used as a vital stain in 1919 by Kleefeld for the identification of corneal ulcers. Marx and Sjögren later used RB in their research, making RB the most commonly used stain between World War I and World War II.9
Though RB is also created from fluorescein, it is distinguished by the fact that it stains the surface cells of the conjunctiva and cornea that are not covered by mucin. RB stains dead or damaged cells, and might not technically be a “vital dye,” as it has a direct toxic effect on healthy cells.9
Figure 2 highlights rose bengal staining on a patient with Sjögren's syndrome.

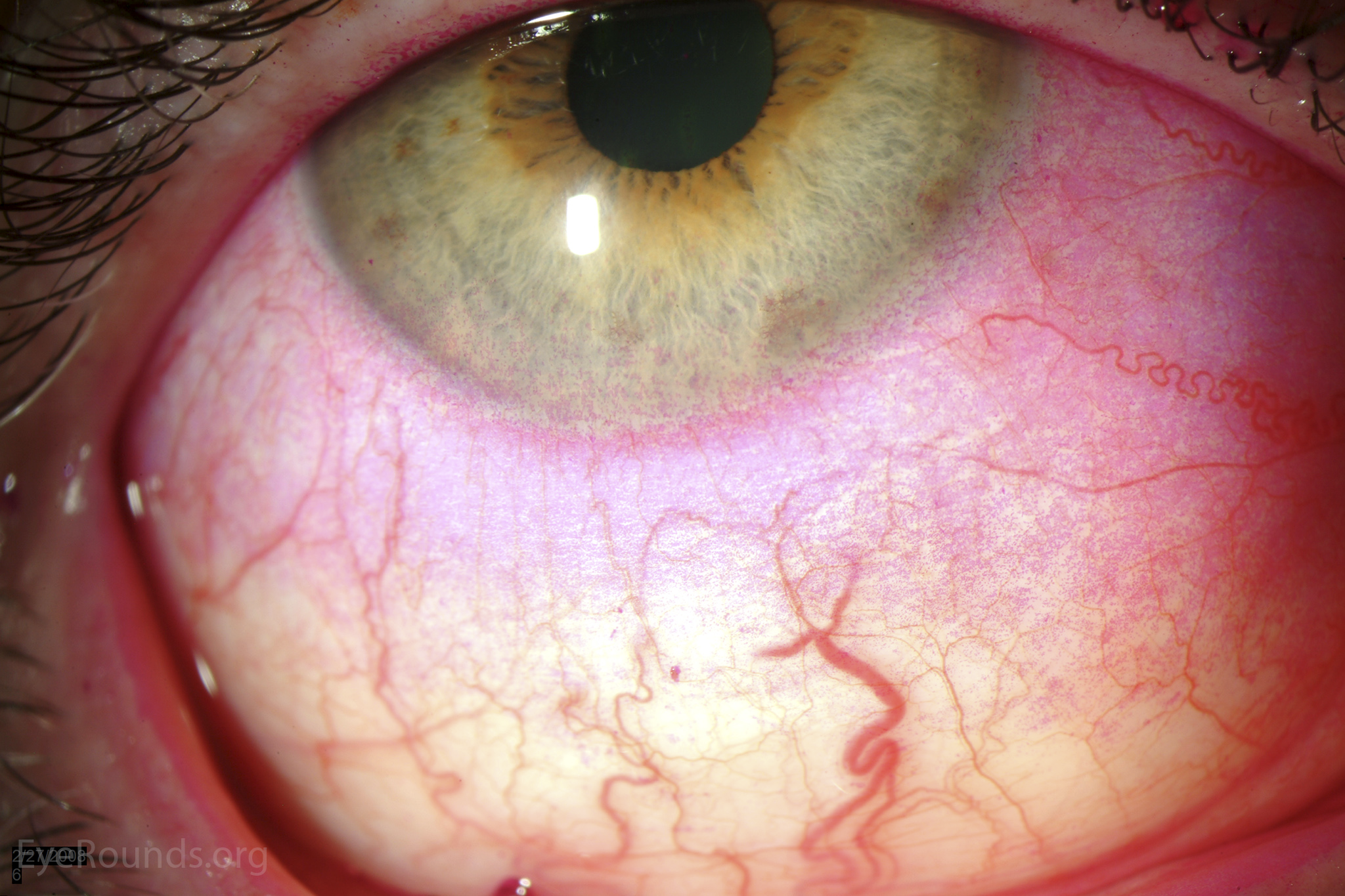
Figure 2: Courtesy of Jesse Vislisel, MD.
Uses for rose bengal dye
RB is the primary dye used for conjunctival staining.
Ocular surface diseases with characteristic RB staining include:6
- Aqueous tear deficiency
- Corneal and conjunctival neoplasms
- Dendritic herpes simplex corneal ulcers
- Lacrimal and meibomian gland dysfunction
- Nocturnal lagophthalmos
- Sjögren’s syndrome
Assessment using rose bengal dye
The best staining results are achieved by instilling a full drop of 0.5% of 1% RB, after a drop of anesthetic (optional), and then waiting a few minutes before judging the stain pattern.6,8
The amount of staining produced by RB on the conjunctiva and cornea is dosage-dependent. When the amount or concentration is lowered, so does the amount of staining. Also, RB staining might be more difficult to see in patients with darker irises.
Using a red-free (green) light source can enhance the RB staining.8 Liberal irrigation with normal saline can be performed after testing.
Pros/cons of rose bengal dye
- Pros: The RB staining pattern lasts longer than the NaFl staining pattern.8
- Cons:
- When RB is applied as a drop, there is significant stinging, which causes reflex tearing.
- It might be difficult to distinguish RB pigment from the underlying color in patients with injected eyes.6
- RB stains skin on contact, causing visually undesirable discoloration that can last for several hours.
- More importantly, RB is toxic to cells and can also be photoactivated by ultraviolet radiation, causing additional toxicity. As a result, sun exposure will exacerbate any symptoms, particularly in dry eye patients with severe staining.8
Lissamine green dye
Lissamine green (LG) is a synthetically produced organic dye that is traditionally used in food additives and cosmetics. LG was first presented as a vital stain by Morgens Norn in 1973 for staining the cornea and conjunctiva.10
LG’s staining profile is practically equivalent to RB, but LG is less toxic and, as a result, less irritating to the ocular surface and patients.11
Figure 3 demonstrates lissamine green staining on a patient with keratoconjunctivitis sicca.
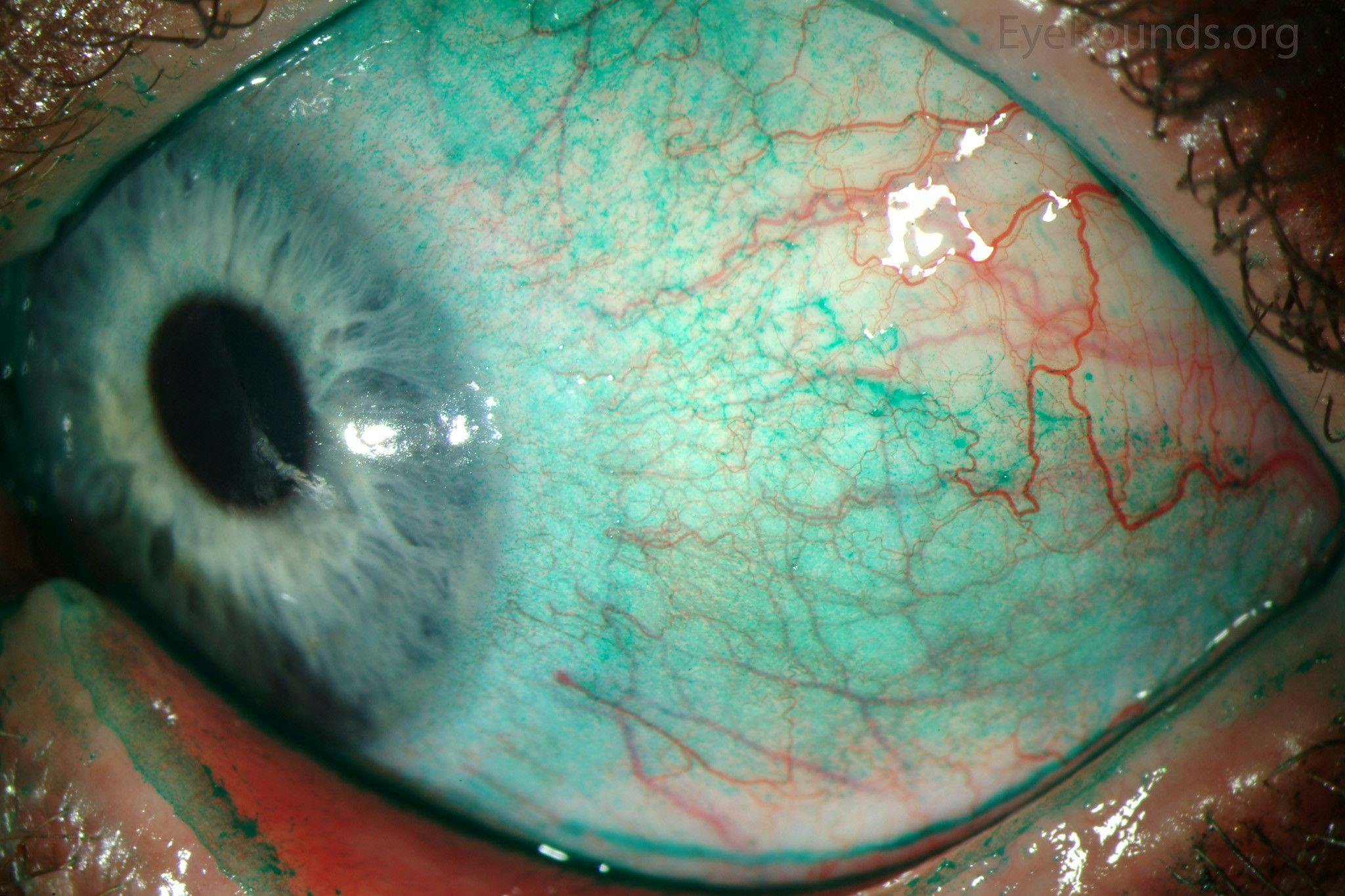
Figure 3: Courtesy of Jesse Vislisel, MD.
Uses for lissamine green dye
Like RB, LG is the primary dye of choice for conjunctival staining. The indications for LG staining are identical to those for RB staining.11
Assessment using lissamine green dye
As with RB, LG staining is dose-dependent. Similar to RB, it may be difficult to see the LG staining pattern in darker irises, and a red filter can help with visualization.
The conjunctival staining will appear black against a red background.8 LG should not sting, so there is no need to limit the dose amount, a full drop should be instilled to maximize the staining.11
Pros/cons of lissamine green dye
- Pros: Compared with RB, LG is nontoxic and is better tolerated by patients, thus making it a superior dye for the evaluation of the conjunctiva.11
- Cons: Some studies have shown that LG strips may not provide enough concentration to highlight conjunctival staining. Liquid LG (bottled) does deliver acceptable concentrations, however due to formulary rules, this preparation is not available in the US.7
Combination of fluorescein sodium (NaFl) and lissamine green (LG) dye
Employing a variety of dyes at the same time can reduce chair time while achieving comprehensive ocular surface staining. In the past, NaFl was combined with RB, but newer protocols combine NaFl with LG due to its similar staining pattern to RB, with better patient comfort.12
Mixing the two stains together does not change or cancel any of their respective effects; the staining properties of NaFl and LG should remain unchanged.12
Figure 4 features a closeup of fluorescein sodium and lissamine green staining on a patient with superior limbic keratoconjunctivitis.

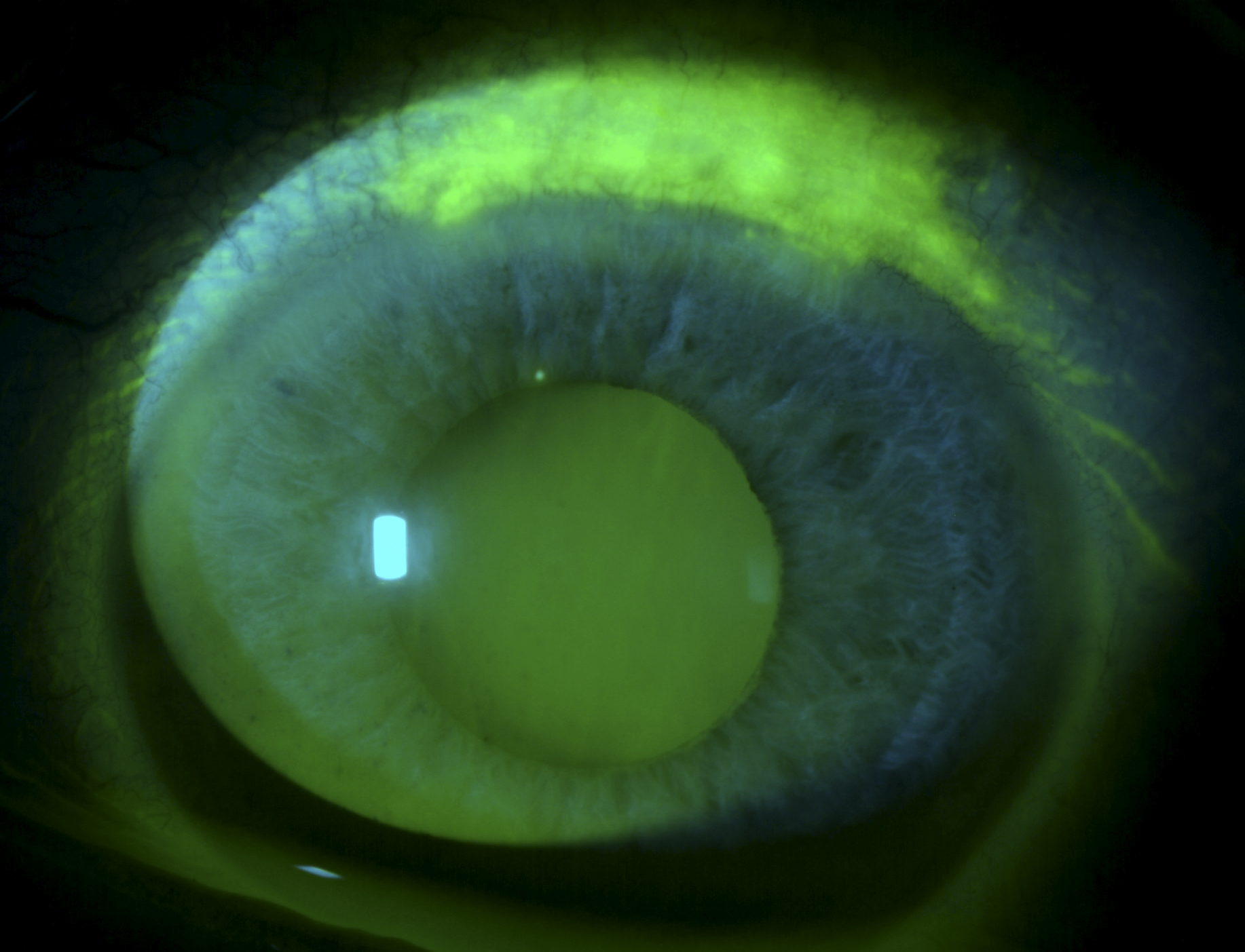
Figure 4: Courtesy of Jesse Vislisel, MD.
Uses of NaFL and LG dye
While there is some overlap, NaFl and LG stain distinct cells and areas of the ocular surface. NaFl is better for judging tear film stability and the cornea, with LG being better for conjunctival staining.
Assessment using NaFl and LG dye
Lissamine green staining of the conjunctiva has a distinct brightness and vividness that is absent from fluorescein or rose bengal staining. This characteristic seems to make it easier to visualize small staining defects.
Some studies recommend a mix of 2% NaFl and 1% LG, while others recommend 1% NaFl and 1% LG.3 Switching between the cobalt blue filter and white light will be necessary.7
Pros/cons of NaFl and LG dye
- Pros: Combining NaFl and LG simultaneously allows comprehensive staining of the entire ocular surface for uninterrupted evaluation, and increases clinician efficiency.
- Cons: The clinician will need to shift back and forth between white light and the cobalt filter during the examination, adjusting the magnification as necessary to appreciate tiny areas within the larger region. The switching process might seem more cumbersome to some.
Injectable/IV-administered dyes
Fluorescein sodium (NaFl) dye
In addition to topical use, NaFl is FDA-approved for IV use as well. However, intraocular use is strictly off-label.4
Figure 5 shows fluorescein angiography imaging, which utilizes injectable/IV-administered fluorescein sodium, of a patient with sickle cell retinopathy.

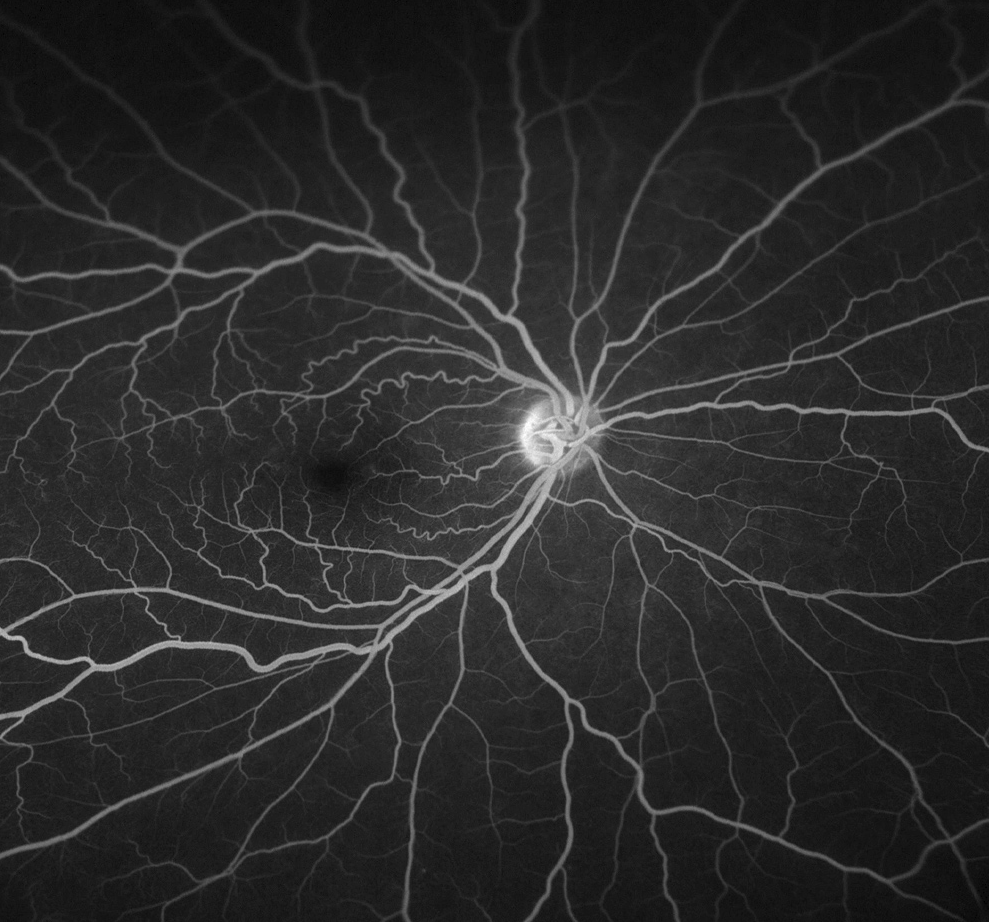
Figure 5: Courtesy of Parekh et al.
Uses for injectable NaFl dye
- Angiography: For years, the injection of intravenous fluorescein sodium has been the gold standard for the diagnostic staining of retinal and choroidal vessels during fluorescein angiography (FA).4
- Cataract surgery: NaFl is used as a coloring agent underneath the capsule in cataract surgery, using blue light to visualize staining of the epithelium located on the inner surface of the anterior capsule.2
- Chromovitrectomy: NaFl is very well absorbed by the vitreous, and gives improved visualization of clear vitreous fibers during chromovitrectomy without toxicity.
Note: Highlighted procedures indicate off-label use.2
Pros/cons of injectable NaFl dye
- Pros: NaFl is available in multiple commercial formulations and is very economical.
- Cons: NaFl may not be an optimal agent for cataract surgery due to the migration of NaFl into the vitreous cavity, staining of the cortex and nucleus lenticular regions, and staining of the corneal endothelium, resulting in decreased contrast between the lens capsule and cortex.2
Contraindications for injectable NaFl dye
Allergy
A previous history of fluorescein allergy is a contraindication.14
Pregnancy
Pregnancy is a relative contraindication to intravenous administration of fluorescein sodium. NaFl carries a level of inherent risk as categorized by the latest pregnancy and lactation labeling, with side effects on the fetus that have not been studied.
Due to a lack of safety testing and evidence, it might be advisable to avoid NaFl IV administration unless the lesion is vision threatening or juxtafoveal and the patient is in the second or third trimester to minimize the risk to the fetus.
In addition, patients who are breastfeeding should be advised that NaFl appears in breast milk for up to 76 hours after administration.
Children and infants
Children and infants undergoing FA for retinopathy of prematurity may be vulnerable. Due to the lack of safety data, caution might be warranted to perform an FA depending on the case presentation.14
Indocyanine green dye
Indocyanine green (ICG) is a water-soluble vital dye that can stain corneal cells, the anterior capsule, and ILM.15
Two properties make ICG particularly useful for visualizing the choroidal circulation:
- ICG can penetrate the RPE, macular xanthophyll, and other ocular pigments
- ICG has limited diffusion through the small fenestrations of the choriocapillaris.2
Figure 6 features indocynanine green angiogram imaging demonstrating hypofluorescence in the area where the ILM was peeled in macular hole surgery.

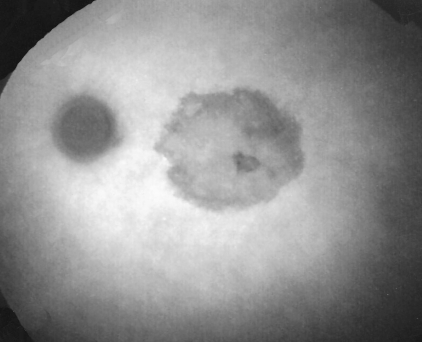
Figure 6: Courtesy of Inoue et al.
Uses for indocynanine green dye
- Angiography: ICG angiography (ICGA) is particularly useful in analyzing choroidal vasculature and is the gold standard for choroidal retinal angiography. ICG is FDA-approved for IV use only.15
- Cataract surgery: Not only is ICG valuable in staining the anterior capsule without any special illumination, but ICG also allows superior capsule visualization in conditions with poor or no red reflex. In ocular surgery, it remains off-label despite widespread popularity in other countries.2
- Corneal transplant surgery: ICG is used for evaluating endothelial cell usability in donor corneas, as ICG almost exclusively stains dead cells. ICG can also color the corneal stroma of the donor disk, making it effective for deep lamellar endothelial keratoplasty (DLEK).2
- ERM/ILM peel: ICG adheres well to the extracellular matrix components of the ILM and helps facilitate ILM peeling in vitreoretinal surgery. Also, ICG has been proposed to allow better visualization of ERMs in vitrectomy for proliferative diabetic vitreoretinopathy (PDVR), idiopathic ERMs, and proliferative vitreoretinopathy (PVR).2
- Glaucoma surgery: ICG can be used to visualize bleb leakage during trabeculectomy.2
- Strabismus surgery: ICG are good vehicles for staining the superior oblique tendon in strabismus surgery. It stains the tendon’s fascia very well, with no staining of the scleral tissue.2
- Other: ICG aids in the visualization of conjunctival cyst capsules. ICG is injected directly into the conjunctival cyst in combination with trypan blue.2
Assessment using ICG dye
NaFl and ICG are often administered simultaneously to provide complete retinal and choroidal vascular imaging.
Pros/cons of ICG dye
- Pros: Rates of adverse reactions to ICG (IV) are significantly lower than NaFl. Nausea and vomiting, which are common with NaFl, are rare with ICG.
- Common reactions specific to ICG include urticaria/hives, hypotension, and vasovagal reaction/syncope. Severe reactions such as hypotensive and anaphylactic shock with ICG are rare.15
- Cons: Intraocular use of ICG is off-label. Similar to NaFl, ICG also carries a level of inherent risk as categorized by the latest pregnancy and lactation labeling.
- In addition, ICG is contraindicated in patients with iodine or shellfish allergies, liver disease, and end-stage renal disease.
- Also, there can be toxic retinal damage from ICG-assisted chromovitrectomy like RPE changes, visual field defects, and optic nerve atrophy.16
Note: Infracyanine Green (IfCG) is a green dye with the same chemical formula and similar pharmacologic properties as ICG, except IfCG contains no sodium iodine. The absence of iodine reduces retinal toxicity and permits it to attach firmly to the ILM while not coloring the ERM.16
Trypan blue dye
Trypan blue (TB) is an azo dye, part of a large class of synthetic organic dyes that produce bright, high-intensity colors. The anterior capsule, corneal cells, and the ERM are just a few of the structures that TB is able to color. TB lightly tints the vitreous and ILM.2
Figure 7 features trypan bue staining, which aids in delineating the anterior capsule from the cortical material.

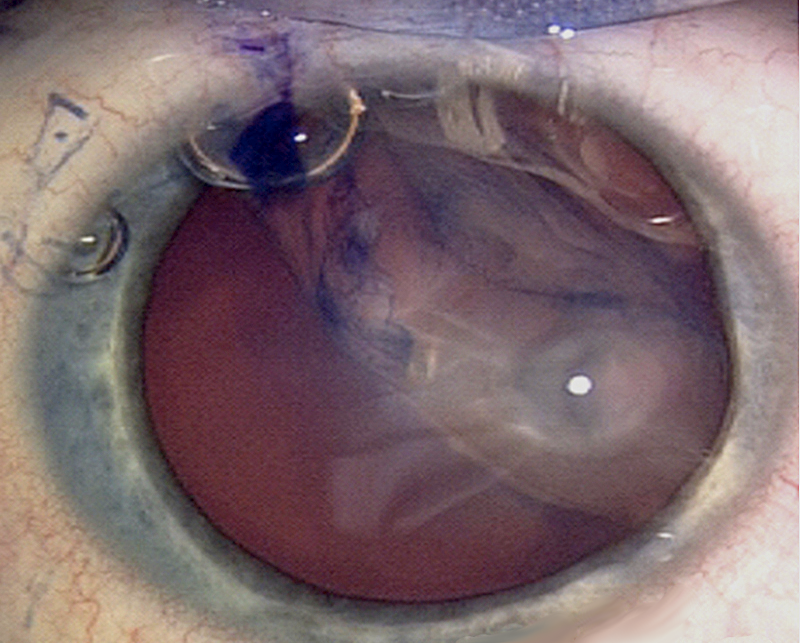
Figure 7: Courtesy of Maassen et al.
Uses of trypan blue dye
TB is FDA-approved for intraocular use.
- Cataract surgery: During cataract surgery, intraoperative TB stains the anterior capsule and its edge intensely, making the differentiation between other tissues easily viewable.2
- Corneal transplant surgery: TB is used to color regions of Descemet’s membrane (DM) lacking endothelial cells as well as the nuclei of injured and dead cells in donor corneas to assess endothelial cell viability.16
- In addition, TB helps in stripping the corneal endothelium from the donor button in deep anterior lamellar keratoplasty (DALK) and Descemet’s stripping endothelial keratoplasty (DSEK).17
- Enucleation: TB is used to stain Tenon’s capsule during enucleation surgery.2
- ERM peel: Because TB has such a high affinity for ERM, it is the dye of choice for ERM identification during chromovitrectomy.2
- Glaucoma surgery: TB can be used to stain the anterior capsule to visualize bleb drainage function during cataract surgery. Mitomycin C and 5-fluorourcil are easily stained with TB, allowing precise placement during filtering surgery.2
- Strabismus surgery: TB, as well as ICG, stains tendon fascia without staining scleral tissue, making it useful in strabismus surgery since it stains the superior oblique tendon so strongly.2
- Other uses:2
- TB is used to coat the phaco incision blade for clear corneal incisions to improve visualization.
- When injected, TB, combined with ICG, aids in the removal of conjunctival cyst capsules.
Pros/cons of indocyanine green dye
- Pros:
- TB is more economical than ICG.
- TB is not toxic to the corneal endothelium.
- TB is considered safe to use in pediatric cataract surgeries.13
- Cons: TB staining might produce retinal damage, especially at higher concentrations.
- The use of TB is contraindicated in the use of dry-state hydrophilic expandable acrylic intraocular lenses (IOLs), as TB can be absorbed by these particular types of IOLs, causing staining and retinal toxicity.2
Brilliant blue G (BBG) dye
Brilliant blue G (BBG) is a synthetic blue agent that has been approved for intraocular use in Europe since 2007. BBG preferentially stains the ILM, without staining the ERM or vitreous.16
Figure 8 shows brilliant blue G staining in a patient undergoing ILM peeling.

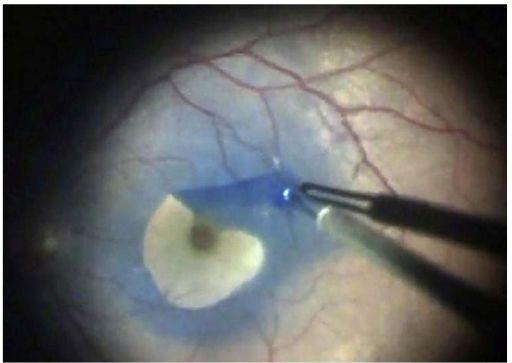
Figure 8: Courtesy of Gelman et al.
Uses of BBG dye
BBG is FDA-approved for ILM staining only.
- Cataract surgery: BBG is used to stain the anterior capsule in cataract surgery.2
- ILM/ERM peel: BBG dyes the ILM but not the overlying ERM, causing the ERM to be visible against the blue background of the underlying ILM, called negative staining.
- This helps facilitate the peeling of the ERM. After the ERM is peeled away, BBG is instilled again to stain the ILM, which is then peeled. This process is called double staining.17
Pros of BBG dye
BBG stains the ILM very well and is less toxic to the RPE cells than ICG, making it a good alternative in chromovitrectomy.2
Bromophenol blue (BroB) dye
Bromophenol blue (BroB) is a blue color marker dye mostly used in laboratory settings.2 BroB is approved for intra-operative use in Europe and is marketed as a combined dye formulation of BroB and BBG.13
Uses for BroB dye
- Cataract surgery: BroB is capable of staining the anterior capsule for enhanced visibility during cataract surgery.2
- ERM/ILM peel: Being less toxic, BroB is a safer alternative to ICG for staining the ERM, ILM, and vitreous in chromovitrectomy.2
Cons of BroB dye
The most significant drawback to BroB is that it is currently not FDA-approved for any kind of ocular use in the US.13
Patent blue (PB) dye
Another arylmethane dye is patent blue (PB), which stains the ERM and vitreous selectively while only faintly coloring the ILM.2
Uses for PB dye
- Cataract surgery: PB has been certified in Europe since 2003 for anterior capsule staining during cataract surgery.
- ERM peel: PB is an adjunctive tool in chromovitrectomy to stain the ERM selectively.
Pros/cons of PB dye
- Pros: PB and TB have comparable safety profiles, being that they are both less hazardous to the retina than ICG.
- Cons: PB is not FDA-approved in the US, nor is it certified for vitreoretinal surgery in Europe.13
Triamcinolone acetonide dye
Triamcinolone acetonide (TA) is a synthetic, non-soluble corticosteroid that is FDA-approved for intraocular use. As a dye, it is used to stain the vitreous and ILM. TA is composed of white crystals suspended in an aqueous solution. These crystals are responsible for its staining capabilities.13
Figure 9 highlights triamcinolone acetonide staining of a patient undergoing vitreous cortex removal.

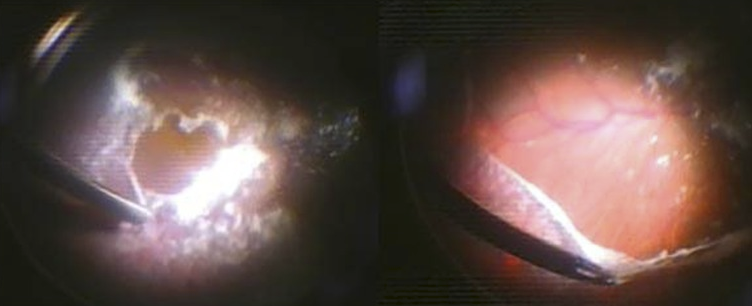
Figure 9: Courtesy of Mohammad A Rashad.
Uses for TA dye
- Anterior vitrectomy: TA can be injected into the anterior chamber to view the vitreous for prolapse.2
- ILM peel: ILM removal with TA yields effective outcomes comparable to ICG-guided ILM removal without the toxic side effects.2
Pros/cons of TA dye
- Pros: TA is a low-cost option as a staining dye. Furthermore, it is hypothesized that using TA as a visual aid may have the extra benefit of reducing post-operative inflammation and vitreoretinopathy.
- Cons: Intra-operative TA during vitreoretinal surgery decreases the risk of post-operative RD, but there is a risk of increased IOP requiring glaucoma drops post-operatively.2
In summary
In summary, vital dyes, with selective wavelengths of light and fluorescence, have transformed semi-transparent tissues seen previously only in grayscale, into colorful and vivid architectural structures.
This use of vital dyes has enabled the visualization of biological anatomy in science and eyecare, advancing and improving the detection, surgical treatment, and management of ocular disease.


