


Pachychoroid spectrum conditions are a group of clinical entities that share the common characteristic of a thickened choroid. Advancements in ophthalmic imaging technology have provided more insights to better understand changes in the choroid in certain diseases that were previously identified only by their retinal manifestations.1
Choroid overview
To better understand these pachychoroid spectrum conditions, we must first better understand the choroid itself. The choroid supplies vascular support to the external third of the retina, and its integrity is essential for normal retinal function.2 The capillaries in the choroid are large in diameter (20 to 25μm) and have fenestration of about 700 to 800nm, which allows for rapid transport, especially of bigger molecules.2
The choroid is composed of five layers (inner to outer):
- Bruch’s membrane
- Rush layer (choriocapillaris)
- Sattler’s layer (medium diameter blood vessels)
- Haller’s layer (large diameter blood vessels)
- Suprachoroidal space (transition zone between the choroid and sclera)
Based on optical coherence tomography (OCT) scans, we are able to determine certain anatomical characteristics of the choroid; it is thickest in the subfoveal region (300μm), thinnest in the nasal region, and has progressive thinning through the temporal region. The average thickness is approximately 260μm.2
Figure 1 illustrates a choroid cross-section as seen on enhanced-depth imaging optical coherence tomography (EDI-OCT). In this image, the subfoveal region of the choroid was measured vertically from the outer border of the retinal pigment epithelium (RPE) to the inner border of the sclera.5

Figure 1: Courtesy of Journal of the Korean Ophthalmological Society.
The pachychoroid disease spectrum
With newer technology, especially EDI-OCT and swept-source optical coherence tomography (SS-OCT), increased choroidal thickness was noted in certain conditions. Hence, the term pachychoroid (thick choroid) disease was introduced. A focal or diffuse increase in choroidal thickness is commonly found among these conditions.
Increased choroidal thickness is secondary to dilated choroidal vessels in Haller’s layer (pachyvessels) and thinning in Sattler’s layer, along with/without RPE abnormalities over those thick vessels.1
Other changes within the pachychoroid spectrum include RPE layer alterations and thinning of the outer nuclear layer, pachydrusen or drusen-associated thickened choroid, choroidal neovascularization (CNV), and indocyanine green angiography (ICGA) hyperfluorescence.4
Conditions in the pachychoroid disease spectrum include:
- Central serous chorioretinopathy (CSC)
- Pachychoroid pigment epitheliopathy (PPE)
- Pachychoroid neovasculopathy (PNV)
- Polypoidal choroidal vasculopathy (PCV)/Aneurysmal type 1 neovascularization (AT1)
- Focal choroidal excavation (FCE)
- Peripapillary pachychoroid syndrome (PPS)
Central serous chorioretinopathy (CSC)
Central serous chorioretinopathy, also known as central serous retinopathy, is characterized by serous retinal detachment with or without serous pigment epithelium detachment (PED). This condition occurs in young to middle-aged men with emmetropic or hyperopic eyes, but gender predilection decreases with age.1
The main risk factors include systemic use of corticosteroids and sympathomimetics. The main visual symptoms include distorted or decreased vision, relative scotoma, the manifestation of small hyperopic shifts, and micropsia.1 The typical manifestation of CSC is a neurosensory retinal detachment and a serous PED. Most cases resolve without any intervention in 4 to 6 months.
OCT is an important tool in assessing this condition, as central serous chorioretinopathy can be confined to the macula. Recent research with OCT testing has demonstrated a pathologically thickened choroid in CSC patients.1
There appears to be dilation of Haller layer vessels which leads to this thickening of the choroid. On ICGA, eyes with CSC show dilated choroid vessels that are diagonally oriented and communicate with the vortex ampullae.2
Figure 2 features variations in OCT and fundus autofluorescence (FAF) of central serous chorioretinopathy with letters a through c.1


Figure 2: Courtesy of “Eye.”
Pachychoroid pigment epitheliopathy (PPE)
This condition is characterized by RPE changes that occur in the posterior pole over the regions which have choroidal thickening.1 These patients are often misdiagnosed with age-related macular degeneration (AMD), but PPE is usually asymptomatic.1
Its clinical presentation can include mottling of RPE, irregular areas of RPE elevation (named drusenoid RPE lesions), and the absence of soft drusen commonly seen in eyes with AMD.1
The choroid of patients with pachychoroid pigment epitheliopathy shows hyperpermeability on ICGA and dilated vessels in Haller’s layer. Clinical signs and symptoms include no changes in visual acuity, absence of fundus tessellation, and RPE lesions that could have drusen but no subretinal fluid (SRF).2 This condition is also known as the forme fruste CSC.
Figure 3 demonstrates PPE in a 37-year-old white female. Images a and b feature color fundus photographs that show absent drusen and reduced fundus tessellation. Images c and d show FAF with non-specific pigment epithelial changes. Images e and f highlight spectral domain optical coherence tomography (SD-OCT) with thick choroid and vessel dilatation in Haller’s layer.6

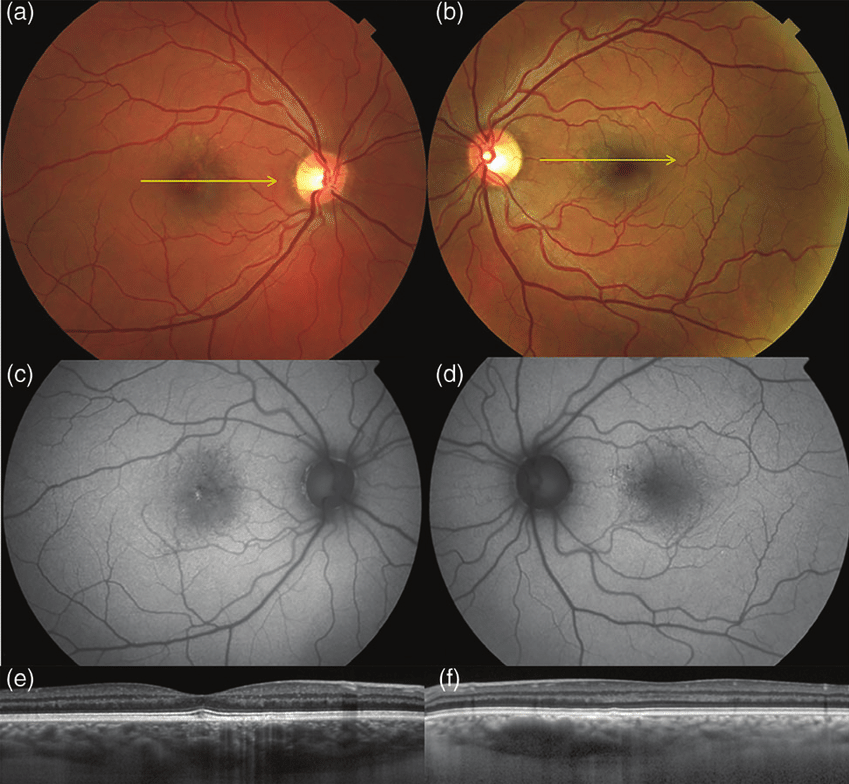
Figure 3: Courtesy of “Clinical & Experimental Ophthalmology.”
Pachychoroid neovasculopathy (PNV)
As we learned in optometry school, there are three different types of choroidal neovascular membranes.
Types of choroidal neovascular membranes:
- Type 1: “Occult,” in which the CNV is below the RPE3
- Type 2: “Classic,” where it passes through the RPE and is located above RPE in the subretinal space3
- Type 3: Retinal angiomatous proliferation (RAP), which occurs in the neurosensory retina and progresses posteriorly into subretinal space3
Type 1 CNV is seen more frequently in PNV. This condition is typically distinguished from AMD by the age of onset, the relative absence of drusen, and a thicker choroid with pachyvessels.3 The presence of type 1 neovascularization and absence of drusen is uncommon in AMD.3
A clinical feature of PNV is the presence of type 1 neovascularization, which appears on OCT as shallow irregular separation of RPE from Bruch’s membrane overlying pachyvessels.1 An additional clinical feature is heterogeneously hyperreflective material in the sub-RPE space, which suggests the presence of sub-RPE neovascularization.1
Small-packed PEDs may develop at the margin of these lesions. The background features of pachychoroid spectrum disease are also present. These include the absence of soft drusen and reduced fundus tessellation, indicative of a thickened choroid.1
Figure 4 is a collection of imaging done on a 46-year-old female with PNV. In the figure, images a to c are OCT imaging of shallow elevation of RPE, and image d demonstrates a resolution of subretinal fluid. Image e features the development of narrow-peaked PED, image f shows a localized area of abnormal flow signal with PED, image g is OCT-A imaging with a neovascular network with aneurysms in its temporal margin, and image h shows the outline of pachyvessels on optical coherence tomography angiography (OCT-A).1

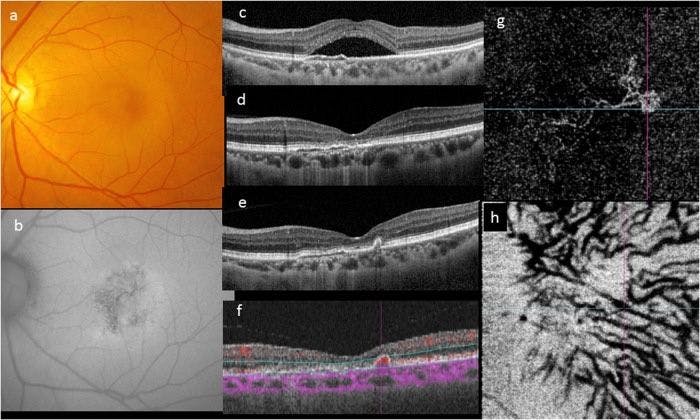
Figure 4: Courtesy of “Eye.”
Polypoidal choroidal vasculopathy (PCV)/aneurysmal type 1 neovascularization (AT1)
PCV was first described by Yannuzzi et al. in 1990 as a new clinical entity where hemorrhagic and exudative sensory detachments occur in the peripapillary and macular regions in people of Asian or African ancestry and middle-aged women.1 Recent studies of this condition with OCT categorized this condition as a type 1 (sub-RPE) neovascularization.1
Researchers also noted that these “polypoidal” lesions are vascular structures that tend to bleed and rupture. Hence this sub-RPE vascular proliferation was also referred to as aneurysmal type 1 neovascularization to clarify its true nature.
Further examination via OCT can reveal a branching vascular network and aneurysms that are below RPE and its basal lamina, anterior to the inner collagenous layer of Bruch’s membrane hence being type-1 neovascularization.1 These patients tend to have thick choroids and choroidal hyperpermeability as compared to those with AMD.
Minimal or absent drusen, pachyvessels in the inner choroid, and shallow irregular PEDs are also common findings.3 The visual prognosis of these patients is variable, but many patients lose central vision eventually.1
Figure 5 demonstrates scans of choroidal features that show PCV/AT1. Images a and b are the ICGA of a patient with PCV, and images c and d show increased subfoveal choroidal thickness.1

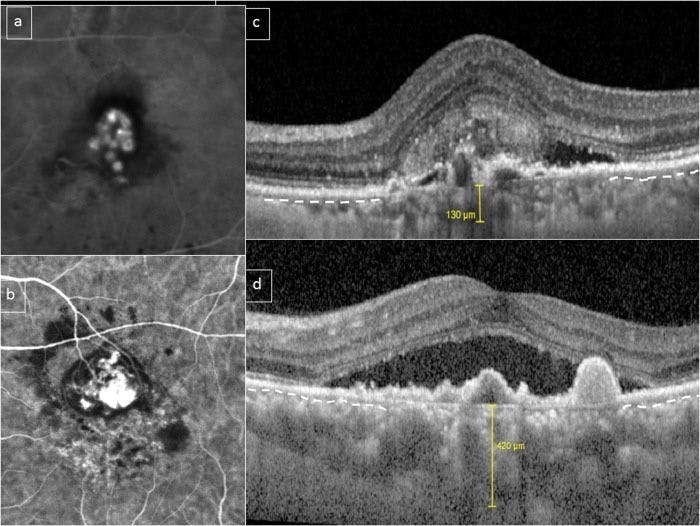
Figure 5: Courtesy of “Eye.”
Focal choroidal excavation (FCE)
FCE is characterized by localized areas of choroidal excavation without posterior staphyloma or scleral ectasia.1 These patients are usually diagnosed in the fourth or fifth decade of life with no gender predilection. In addition, patients tend to be asymptomatic but can sometimes report metamorphopsia or mild blurring.1
Clinical signs on fundus may appear to be normal, have non-specific pigmentary changes, or have indistinct yellow-whitish spots in the area of reduced tessellation.1 Upon OCT, two different patterns are observed. In conforming FCE, the photoreceptor tips are in direct contact with the RPE, but in non-conforming FCE, the photoreceptor tips appear detached from the underlying RPE with a hyporeflective cleft (giving SRF representation).1
Pachychoroid features are evident in FCE with increased subfoveal choroidal thickness and choroidal vascular hyperpermeability in ICGA.1 Overall, most studies so far have shown FCE to be a relatively stationary lesion.1
Figure 6 illustrates focal choroidal excavation.7 As we see in this 59-year-old patient, images A and B show color fundus photographs of a depigmented lesion surrounded by hyperpigmentation. Images C and D show SS-OCT with thick choroids.

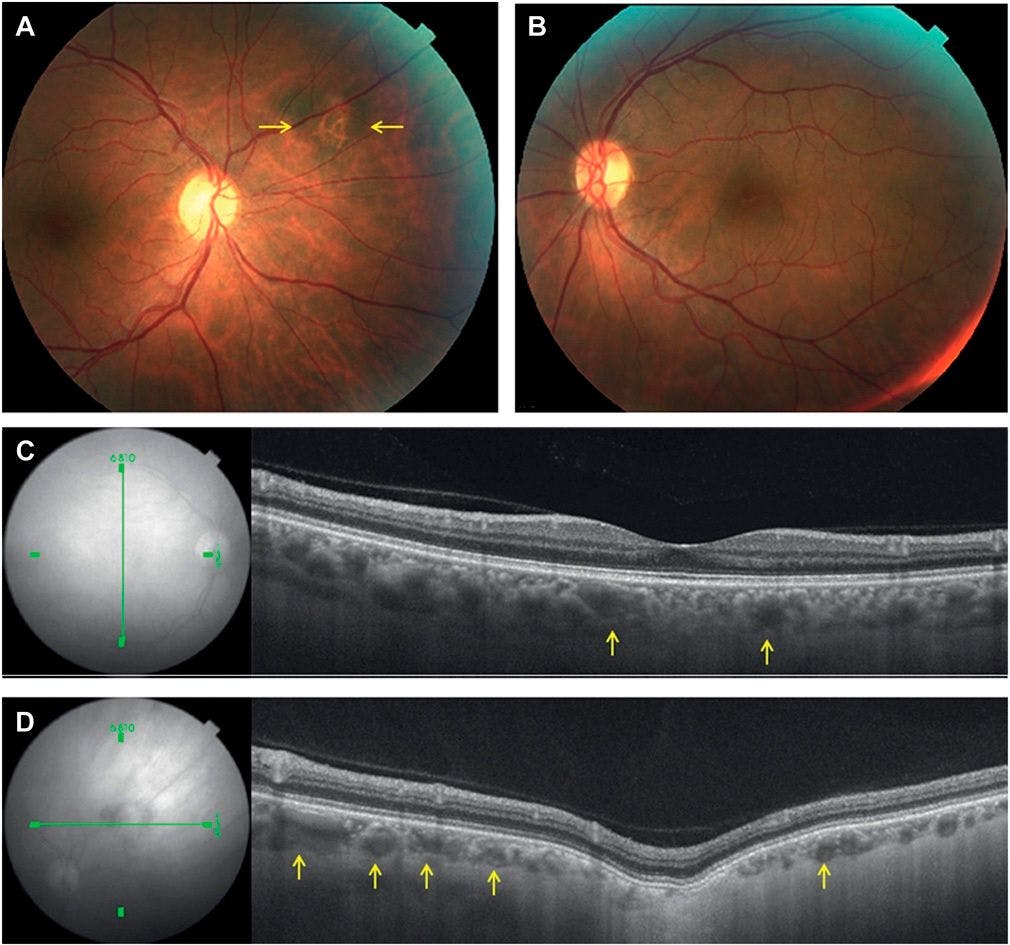
Figure 6: Courtesy of “Retina.”
Peripapillary pachychoroid syndrome (PPS)
This condition was recently described by Phasukkijwatana and colleagues as a distinct variant of the pachychoroid spectrum where choroidal thickness occurs close to the optic nerve instead of the subfoveal region.1
Clinical signs include nasal macular intraretinal and/or SRF and occasional optic nerve edema.1 Other signs include serous PED, pachyvessels, and overlying choroidal thinning choroidal hyperpermeability, all of which are associated with the pachychoroid spectrum. Common features include choroidal folds (77% of cases), short axial lengths, and hyperopic refractive error, along with older age and a small cup-to-disc ratio.2
Figure 7 shows clinical imaging and OCT scans of features of peripapillary pachychoroid syndrome.8

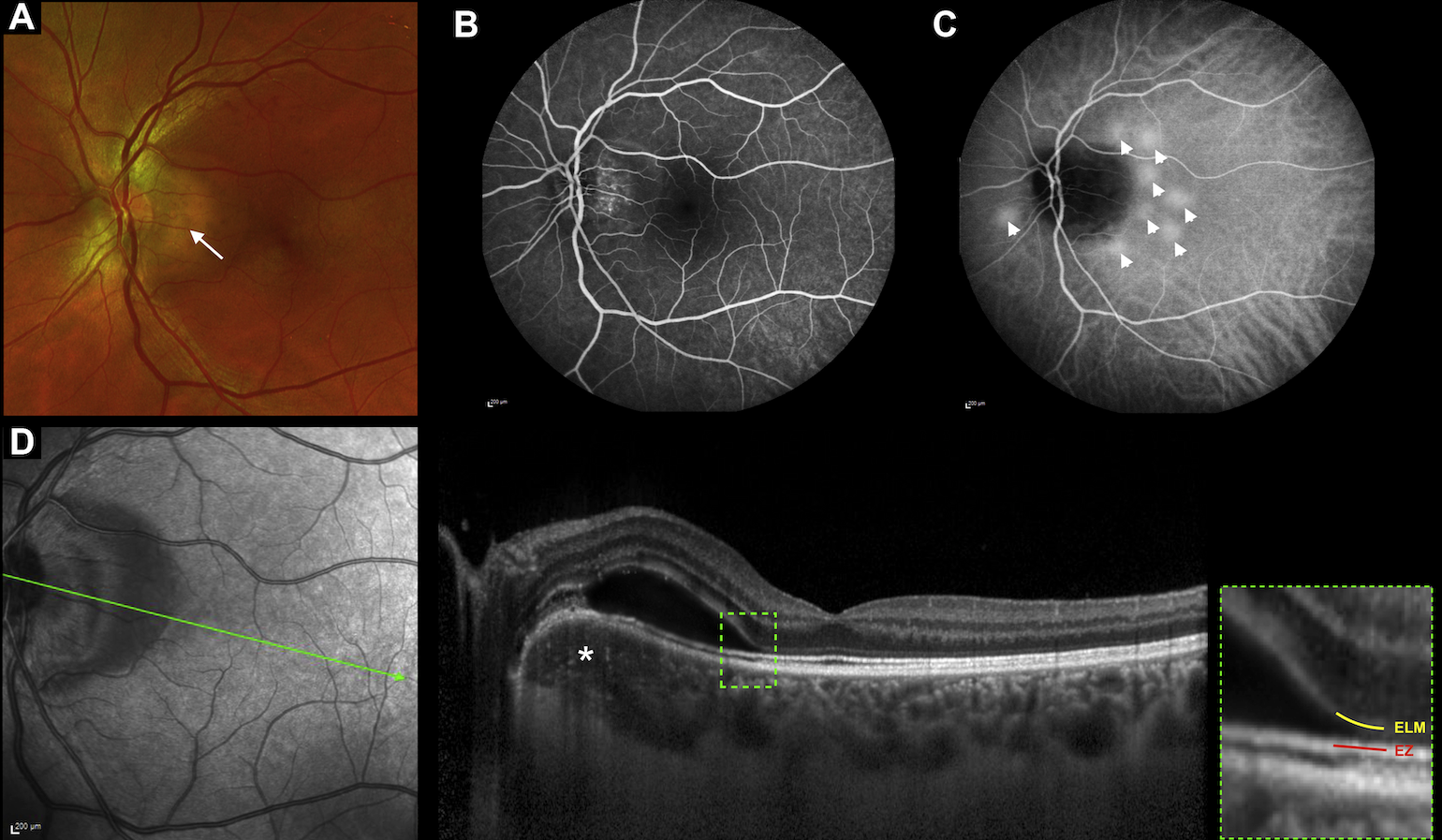
Figure 7: Courtesy of “Ophthalmology Retina.”
Pathogenesis of pachychoroid spectrum disease
In brief, the pathogenesis of pachychoroid disease remains largely unknown, but evidence points toward aberrant steroid metabolism as a factor.1 This altered steroid metabolism often explains why patients with CSC can have psychological stress or sleep deprivation at the peak of their symptoms.1
Mineralocorticoid receptors are expressed in the choroid; hence their stimulation leads to increased choroidal thickness and congestion.1 Chronic inflammation or focal RPE disturbances may be the cause of the neovascular process.1
Treatment and management of pachychoroid spectrum disease
The generalized treatment choice for the majority of the conditions ranges from observation (such as for cases of CSC) to laser photocoagulation. If any leakage is present, then photodynamic therapy (PDT) can also be indicated.2 Anti-VEGF treatment therapies could also be used in cases of neovascularization.
Differential diagnosis
The differential diagnosis for any pachychoroid spectrum condition should include uveitis (e.g., Vogt-Koyanagi-Harada disease), posterior scleritis, choroidal granulomas due to infectious or inflammatory etiology, and infiltrative diseases such as lymphomas or intraocular tumors.
Any of these conditions could potentially lead to a thickened choroid.4 The presence of other pachychoroid features in the absence of systemic conditions would also support pachychoroid disease.4
Conclusion
Better ophthalmic imaging technology has enhanced our understanding and classification of many ocular conditions. Improvement in future technology and testing would help us further understand the pachychoroid disease spectrum, especially within areas of uncertainty. With this improved awareness, therapies can be aimed at treating changes within the choroid, which are common to all pachychoroid diseases.1


