



Geographic atrophy (GA) is an advanced form of age-related macular degeneration (AMD), accounting for a significant portion of vision loss in the population.
The prevalence of GA worldwide is estimated to be about 5 million people, while in the United States, it is approximately 1 million people,1 with 160,000 new cases occurring each year in the US.2
The average age of a patient with GA is 79 years.3 For every decade after 50 years of age, the prevalence quadruples from 0.15% to 2.91% at 80 years of age.4
The incidence of GA is projected to increase in the coming decades because of an increase in the aging population and overall burgeoning awareness of the disease state.5
Intertwining worlds: AMD and GA
In the realm of AMD, the evolution of geographic atrophy might only differ partially but is fundamentally an offshoot when reviewing its timing and progression, risk factors, and underlying mechanisms.
For all intents and purposes, the conception of GA is over 50 years in the making for those at risk, whereas its “march” across the macula is typically accomplished in less than a decade. The interval from incidence of non-central perifoveal GA lesions to central involvement is typically around 2.5 to 3 years.6
Overview of AMD progression to GA
Stepping back for a moment, there are three distinct stages of AMD: early, intermediate, and advanced.7 Breaking it down further within the advanced stage, there are two distinct forms: wet or neovascular AMD (nAMD) and dry AMD.8,9 Zeroing in on GA, this can be defined as the progressive, irreversible, advanced form of dry AMD.10
Although the advanced form of nAMD is known to be caused by abnormal blood vessels leaking blood or other fluids into the macula, GA is characterized by atrophic lesions that start out in the outer retina and retinal pigment epithelium (RPE).11,12
Another distinction between nAMD and GA is that the former is characterized by acute vision loss, while the latter is a progressive disease that can lead to irreversible central blindness over time.13
Several risk factors have been closely associated with GA, with the strongest correlation being age and family history. Further, smoking and genetic mutations can heighten triggers within the complement system as additional risk factors.
Figures 1 and 2 shows the evolution of complete RPE and outer retinal atrophy (cRORA) via OCT imaging. Note the significant choroidal hypertransmission in Figure 1 and atrophic lesion development in Figure 2.

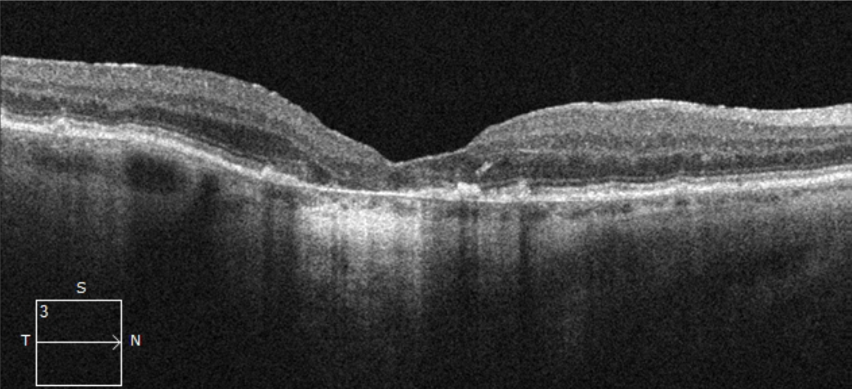
Figure 1: Courtesy of Daniel Epshtein, OD, FAAO.
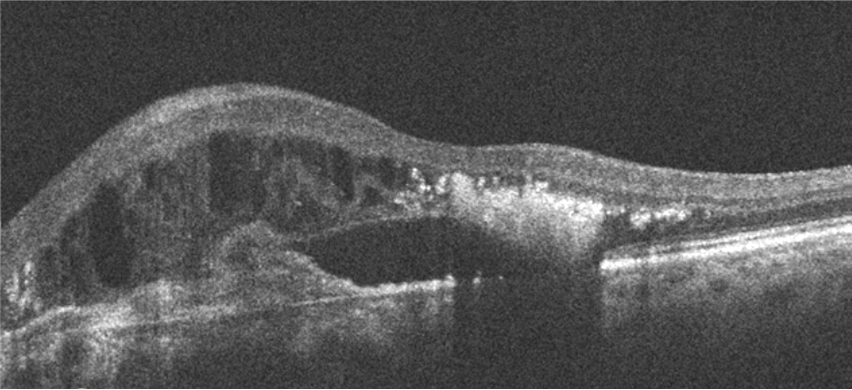
Figure 2: Courtesy of Daniel Epshtein, OD, FAAO.
Vision loss and geographic atrophy
Visual deficits with GA can be rather profound. A retrospective cohort analysis in the UK (n=1,901) found that in patients with bilateral GA, 16% became legally blind (median time to progression of 6.2 years [interquartile range (IQR), 3.3 to 8.5]) and 66.7% became ineligible to drive (median time to progression of 1.6 years [IQR, 0.7 to 2.7]).
When observing typical visual symptomatology in daily life, blurring, distortion, and changes in perception affected activities such as driving, traveling as a passenger in a car, and walking.14 Reading for both pleasure and necessity was also impacted by GA.
Other activities that patients might give up or have difficulty with due to GA would be housework, sewing and crafts, puzzles, reading, music, and watching television. Essentially, losing independence and becoming reliant on others is a significant concern for this population.
A recurring theme to be noted is that there is a bright future with visual and psychological hope. Both intravitreal pegcetacoplan and avacincaptad pegol have been US Food and Drug Administration (FDA) approved in 2023, which can be used to treat GA secondary to AMD.15
How GA may get triggered
The RPE within the normal aging process can be exposed to intrinsic and extrinsic oxidative stressors, along with environmental stressors such as cigarette smoke. When oxidative tissue damage accumulates, this results in the formation of drusen, which can be inherently visible in the early stages to intermediate AMD. The appearance and progression of drusen deposits are prognostic hallmark features of GA.10
The cumulative nature of excessive drusen coupled with druse components, such as cellular debris, lipids, and lipoproteins, may trigger a relatively acute to chronic inflammatory response via multiple pathways—namely the complement cascade.10 Chronic inflammation can eventually lead to photoreceptor, RPE, and choriocapillaris apoptosis, leading to the appearance of sharply demarcated atrophic lesions.
These areas resemble geographic “hills and valleys” found on maps that are characteristic of GA, with deeper choroidal vessels visibly showing through due to the missing RPE layer.
The complement system conundrum
It is evident from genome-wide association studies (GWAS) that an increased risk of AMD can be associated with genetic variants of factors of the complement pathway. Furthermore, a complement C3 genetic variant was found to be associated with AMD, including GA.16
The overactivation of the complement system is strongly correlated in multiple studies with lesion development and progression in GA. In particular, from a structural retina standpoint, it is associated with the loss of photoreceptors, RPE, and choriocapillaris.10,17
The RPE plays a critical role in the maintenance and survival of the photoreceptor cells (specifically the interconnection with the outer segments), in clearing cellular debris, and in regulating the integrity of the choroidal capillaries.18,19 Looking at the choriocapillaris, this system supplies blood to the outer retina and nourishes the retinal nerve fiber layer network via inner retinal circulation.18
When functioning normally, the complement system is an important part of the “checks and balances” of the body’s natural immune response. Under homeostatic conditions, the purpose of complement proteins would be part of a rapid response when there is an antigen-presenting cell (APC) such as microbes or stress signals.
However, overactivation or loss of regulation of this host response can prove to be quite deleterious by perpetuating a vicious cycle of tissue injury and inflammation similar (but different) to what is found in dry eye disease.
The deleterious effects of an unregulated complement system
When complement activity lifts off and becomes unregulated, it has been found to accelerate tissue damage, which is seen in both GA lesions and areas just outside the lesion. In areas outside the lesion, this is where notable increases in lesion growth pose a heightened risk of progression.
Digging deeper into the complement system, the complement protein C3 can play a central role in driving downstream action that could foment damaging effects, including the progression of GA, for potentially several reasons:20
- All three of the complement activation pathways (classical, lectin, and alternative pathways) converge at C3, with convertase-mediated cleavage of C3 into C3a/C3b, which again has been associated with downstream action along with C3b that acts as a pivot point for amplification of complement activation. Overactivation of both C3 and further downstream C5 can be considered necessary machinery to initiate the assembly of the membrane attack complex (MAC). This unit causes irreparable cell membrane destruction and, consequently, cell death.
- Excess phagocytosis, inflammation, and cell lysis—all of these processes might contribute to retinal cell death and can be linked to complement system overactivation.
- Inflammatory cell recruitment—C3a and further downstream, C5a activate these cells creating a potential vicious inflammatory loop.
Complement system overactivation and AMD pathogenesis
The complement system is involved in drusen formation, with C3 and C5 fragments having been detected in histopathological probes of drusen in patients with AMD. Activation of the complement cascade can result in cleavage of factor C5 into C5a and C5b fragments. To note, the C5a fragment is a key inflammatory activator that is found in drusenoid material of patients with AMD.
Interestingly, the production of vascular endothelial growth factor (VEGF) can echo back to when C5a recruits inflammatory cells and stimulates the RPE. The anatomical flipside would be the C5b fragment that sparks the formation of MAC, precipitating a significant inflammatory response within Bruch’s membrane and choriocapillaris.
An important feature to point out is that the severity of this response is dependent on age and level of AMD. Finally, to close the loop, the deposition of MAC in choriocapillaris and its presentation to choroidal endothelial cells trigger cell lysis, likely contributing to RPE atrophy in both dry AMD and nAMD, respectively.
Complement inhibition treatments to manage geographic atrophy
Due to the complement cascade’s role in the pathology of AMD, complement inhibition has been identified as a key drug target for therapeutic intervention.10
The current mechanism and pathophysiology being targeted include complement factor C5 with the agent avacincaptad pegol, which was recently approved by the FDA in August 2023, is a pegylated RNA aptamer that binds and inhibits C5.21,22
Pegcetacoplan, recently approved by the FDA for intravitreal injection for GA secondary to AMD, is a synthetic peptide inhibitor of C3 that actively binds to complement protein C3 and its activation fragment C3b with high affinity in order to regulate the cleavage of C3 and the generation of downstream effectors of complement activation.15
Geographic atrophy diagnosis 102
It is recognized that GA can ultimately lead to central and parafoveal scotomas within the visual axis. With the fovea containing the highest density of cone photoreceptors, it is unequivocally responsible for central and color vision.
Keeping this thought in mind, GA strikes right at the heart of this anatomical space. However, even without the involvement of the fovea, lesions outside the fovea may still cause visual disabilities in daily life, including reading, writing a check, or recognizing faces.
The hallmark sign of GA—sharply demarcated atrophic lesions due to loss of photoreceptors, RPE, and choriocapillaris will tend to initially appear extrafoveally. This potentially causes progressive visual impairment by expanding toward the fovea and eventually leading to irreversible central visual loss.10,11
Foveal lesions and visual acuity
Oftentimes, the fovea can be spared until later in GA’s progression timeline, resulting in visual acuity that remains nearly within normal limits. An important distinction comes in the form of contrast sensitivity and ability to read, which may provide the first line of contextual symptomatic clues as early warning signs.
Once lesions encroach on the central portion of the fovea with progressive disease, they are referred to as lesions with subfoveal involvement (or foveal lesions). With subfoveal involvement, central vision can be severely impaired, and the patient may experience rapid loss of visual acuity function with a median time from nonsubfoveal to subfoveal involvement of GA ranging from 1.4 to 2.5 years.6,10,23,24
While GA is not diagnosed by laboratory or genetic testing, it is made with the collective use of visual function tests to assess visual impairments and imaging studies to detect clinical features.
Visual function tests in patients with GA25
1. Reading charts
Reading charts may be used to measure visual acuity (VA); however, these tend to lack the specificity and sensitivity to provide the information necessary for actual retina function due to foveal-sparing and parafoveal scotomas.
Reading ability may be evaluated by the following 2 types of tests:
- Snellen or Early Treatment Diabetic Retinopathy Study (ETDRS) charts
- Reading speed—which can be quantified by the number of correctly read words over a prespecified period, provides information about how much of the visual field is sufficiently preserved to recognize entire words or sentences as opposed to individual letters
With GA progression, reading speed notably declines.11 In a prospective natural history study of GA patients, the median maximum reading rate decreased significantly from 110 words per minute (wpm) at baseline to 51 wpm by Year 2.
When looking at a comparator cohort, which was represented by patients with drusen only, the maximum reading rate decreased from 130wpm at baseline to 117wpm at 2 years, which was not statistically significant.26
2. Low-luminance visual acuity and deficit
Low-luminance visual acuity (LLVA) and low-luminance deficit (LLD). LLVA involves standard VA testing in low-light conditions, often by adding a neutral density filter in front of the testing eye, which could prove useful as a visual marker for GA.27
Further, a reduced LLVA might indicate symptoms of night vision loss. LLD is the difference between a patient’s BCVA and LLVA scores and could be considered predictive of subsequent vision loss and lesion enlargement in GA.28-31 A LLD greater than 13 ETDRS letters suggests an abnormality.18,28-31
3. Microperimetry
Microperimetry is a fundus-tracked perimetry assessment of central retinal sensitivity that acts as an alternative to reading charts. This technique is typically used under mesopic conditions with varying intensity of light to stimulate the macula in multiple locations to identify functional and nonfunctional areas.
Subsequently, the results depend on the patient’s ability to report recognition of the stimuli, similar to traditional perimetry testing performed for glaucoma patients.32
4. Amsler grid
Amsler grid is an at-home test to measure a patient’s central visual field and line detection. Patients with varying stages of AMD may see the grid lines as wavy, blurred, or distorted.
When the visual field is significantly impaired, the grid may appear to be “pushed inward,” contain darkened areas, or exhibit scotomas.33
Multimodal imaging techniques to identify GA
Clinical features of GA are detected by using slit lamp microscopy with condensing lenses, indirect ophthalmoscopy, and imaging studies to delineate whether there is cell layer loss with sharply defined borders and attrition of the RPE, photoreceptors, and underlying choriocapillaris.11
Common multimodal imaging techniques that could enhance visualization of the fundus and surrounding vasculature to diagnose and grade GA include the following:
- Color fundus photography (CFP) has been the historical standard for image capture of GA lesions. While some investigators do not consider CFP to hold utility as a predictor of GA progression,11 technological advancements in resolution and magnification could allow for the detection of multifocal lesions, lesion size grading, and tracking of bilateral disease.
- Optical coherence tomography (OCT) and OCT angiography (OCTA) are imaging studies that can potentially identify progressive GA lesions by visualizing the loss of retinal layers through cross-sectional and/or en-face images.
- It has emerged as the preferred modality to assess GA lesion features.11,36 Further, OCTA can be leveraged in the detection of co-morbid neovascular AMD.
- Fundus autofluorescence (FAF) is an imaging technique that utilizes blue or green wavelengths of light to visualize the loss of RPE cells. Areas of GA lesions often appear as hypoautofluorescent (decreased autofluorescence) due to the loss of RPE cells containing intrinsic fluorophores, such as lipofuscin.
- This is the primary modality for assessing GA lesion size and growth in research trials and in clinical practice (where available).11
- Remote at-home monitoring is an evolving paradigm where the patient has access to diagnostic devices driven by artificial intelligence (AI) algorithms. This form of testing can aid the clinician and patient to jointly partner in closely monitoring retinal diseases, including GA.34,35
- There are companies present, such as Notal Vision, that offer home monitoring services (approved for intermediate AMD and can allow for the detection of metamorphopsia associated with neovascular AMD) in conjunction with an independent diagnostic testing facility (IDTF), which provides consistency and quality control to maintain appropriate standards.
- IDTFs can be found throughout healthcare in mammography centers, cardiac medicine, and radiology, to name a few.34
Expert group consensus for GA/AMD imaging
With an esteemed group of international experts, the Classification of Atrophy Meetings (CAM) has produced several reports that coin the currently accepted classification system for GA based on imaging.
One of the key takeaways from these meetings was the recommendation to have OCT serve as the benchmark referencing method to define GA and its respective stages, considering the technology has demonstrated the ability to clearly differentiate retinal layers in three dimensions, its wide commercial availability, and the ease of OCT image acquisition along with repeatability.36
While initially, FAF was leveraged for cases in which the diagnosis was relatively unclear, it has gained steam in illustrating high contrast differentiation. This is especially valid in clinical studies where the rate of enlargement of atrophy has been determined to be a regulatory agency-approved anatomical endpoint when utilizing FAF.36 The caveat to FAF is that it still has a deficiency in identifying atrophy near the fovea.
Clinical pearls for identifying and coding for GA
First, a typical diagnostic path for testing would entail vision testing, such as best-corrected visual acuity (BCVA) followed by OCT. If FAF is available, then FAF would be acquired as needed, and in some cases also CFP.
Next, GA has a unique set of International Classification of Diseases, Tenth Revision (ICD-10) codes that define it by foveal involvement and laterality:37
- GA by foveal involvement (without subfoveal involvement [H35.31x3] and with subfoveal involvement [H35.31x4]) in the 7th position of the code.37
- Laterality is routed through “x” in the 6th position of the code, whether it is right (1), left (2), or both (3).
As an example, if the patient has geographic atrophy without subfoveal involvement in the right eye, it would be coded as “H35.3113”. Conversely, if there were GA with subfoveal involvement in the left eye, then it would be “H35.3124”.
Lastly, for imaging studies, here are some helpful Current Procedural Terminology (CPT) codes to remember:38
- OCT retina: 92134
- FAF/CFP: Both share the same code, 92250.
- Microperimetry: An appropriate code would be 92083 since it shares features of a 10-2 extended threshold visual field.39
- Remote screening: These services are categorized under the experimental code set and have a “T” identifier at the end of the code.
- 0379T: Visual field assessment, with concurrent real-time data analysis and accessible data storage with patient-initiated data transmitted to a remote surveillance center for up to 30 days.40
- 0604T: OCT of the retina, remote, patient-initiated image capture and transmission to a remote surveillance center unilateral or bilateral.41,42
- 0605T: The same as 0604T, but this code is used by a remote surveillance center that provides technical support, data analyses, and reports, with a minimum of eight daily recordings over a 30-day time span.41,42
- 0606T: The same as 0604T, but covers the review, interpretation, and report by the prescribing physician or other qualified health professional of remote surveillance center data analysis over a 30-day time span.41,42
Assessing progression through image studies
When discerning the features associated with GA, it is recommended to lock in your focus on certain characteristics, such as focality (unifocal vs. multifocal lesions), location (subfoveal vs. without subfoveal involvement), and lesion size affect the speed of disease progression.
Here is a rundown of what you need to know:
- Multifocal lesions have significantly higher mean (standard error [SE]) growth rates for GA compared to eyes with unifocal lesions (1.97 [0.1]mm2/year vs. 1.05 [0.2]mm2/year, respectively; P < 0.001).43
- Mean (SE) atrophy progression was observed to be significantly greater among eyes without subfoveal lesions compared with eyes with subfoveal lesions at month 6 (0.99 [0.1]mm2 vs. 0.65 [0.1]mm2; P = 0.011) and at month 12 (2.05 [0.2] vs. 1.28 [0.2]; P = 0.001). This data emanates from the Geographic Atrophy Progression (GAP) study (N = 603).43
Lesion size and SDD to measure GA progression
Studies showed that a larger baseline lesion size is associated with higher progression rates than a smaller baseline lesion size.44,45 Further, the GA growth rate in a study size of 213 patients was significantly correlated with the mean GA perimeter.46
When reviewing the literature, it showed that when there was a larger baseline GA area (mm2), it significantly correlated with a larger mean GA growth rate. For every 1mm2 increase in mean baseline GA area, the mean GA growth rate increased by 0.14mm2 per year, which could lend credence to the potential rapid advancement of these lesions within 2.5 years.47
Figure 3 features line scanning ophthalmoscope OCT that reveals multifocal RPE atrophy consistent with geographic atrophy.

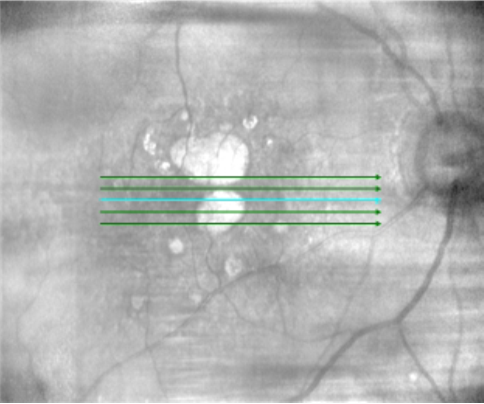
Figure 3: Courtesy of Daniel Epshtein, OD, FAAO.
Another feature to keep in mind is the presence of subretinal drusenoid deposits (SDDs), which have been associated with a more rapid progression of GA.48-50 This clinical sign is defined as subretinal drusenoid deposits above the RPE layer, in contrast to drusen accumulating under the RPE, is associated with a more rapid progression of GA.48
Figure 4 highlights druse with RPE overlying the lesion.

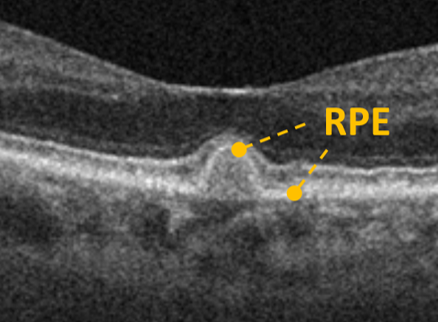
Figure 4: Courtesy of Daniel Epshtein, OD, FAAO.
Figure 5 shows an SDD with the RPE underlying the lesion.

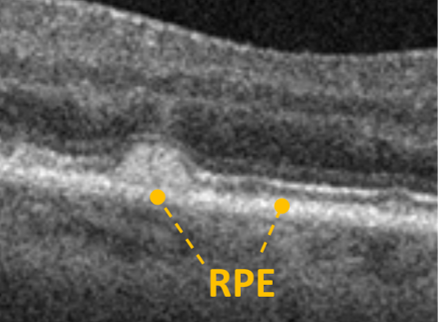
Figure 5: Courtesy of Daniel Epshtein, OD, FAAO.
Using CFP and FAF to assess GA progression
As a reminder, several imaging modalities can be used to monitor the progression of GA. While color fundus photography has been considered the historical standard for imaging GA, there is a significant limitation in contrast detail.51,52 GA on CFP appears as sharply demarcated areas of hypopigmentation.51
Conversely, FAF provides a higher contrast than CFP.51 With the loss of RPE cells found in GA cases, atrophy on FAF presents as regions of hypoautofluorescence.11,51 The rub is that FAF assessment of the foveal region can be rather difficult since macular pigment masks and/or blocks blue light, reducing signal intensity specifically in the atrophic region(s) close to the fovea.
Figure 6 is a color fundus photograph with a central atrophic lesion surrounded by druse and other punctate lesions.

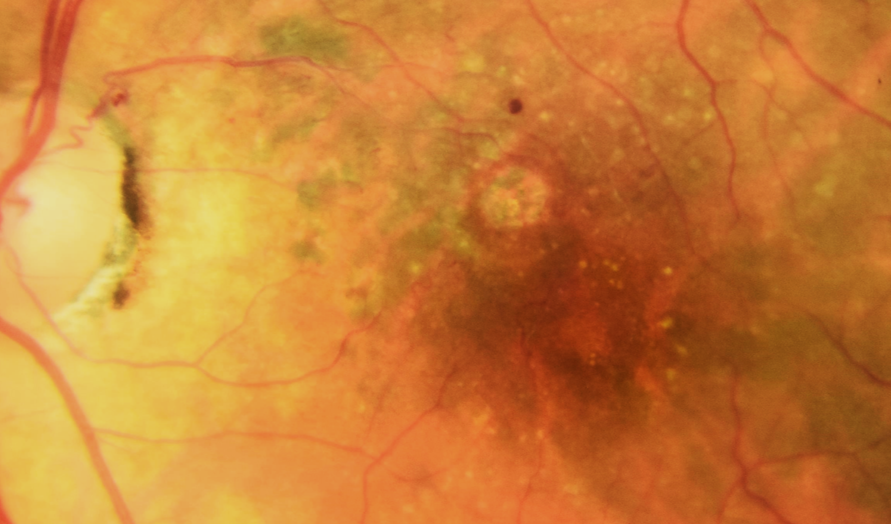
Figure 6: Courtesy of Daniel Epshtein, OD, FAAO.
Comparing swept-source and spectral-domain OCT imaging for GA
Considering these drawbacks found in CFP and FAF, additional imaging modalities are needed to assess GA lesions further.51 Spectral-domain and now swept-source OCT (SD-OCT and SS-OCT) have notable advantages for visualizing GA.
These imaging modalities offer ECPs the ability to analyze cross-sectional and en-face slabs for 3D quantitative assessment, drilling down to specific retinal layers to observe atrophy.36,51 In fact, SS-OCT has advantages in that it allows for a greater field of view with wider imaging areas and enhanced detail to the choroid.51
A closer look at OCT and AMD/GA nomenclature
As was noted in CAM, OCT can be used to identify early atrophy in AMD.36 Proactive GA identification can now be considered imperative for determining whether investigational and commercially available therapeutics could be leveraged to reduce GA progression at early stages.36,53
There were four categories of GA based on OCT criteria proposed by the CAM group, which describe whether the atrophy is incomplete or complete and whether it occurs in the presence of RPE atrophy:36
- Complete RPE and outer retinal atrophy (cRORA)
- Incomplete RPE and outer retinal atrophy (iRORA)
- Complete outer retinal atrophy (cORA)
- Incomplete outer retinal atrophy (iORA)
According to this framework, emerging GA and GA are considered subsets of cRORA and iRORA, respectively, which occur in the absence of macular neovascularization (MNV).36
Table 1 outlines key GA nomenclature and descriptions of the findings.
| AMD Findings | Description |
|---|---|
| Geographic Atrophy | Clinical term used to denote areas of retinal and RPE atrophy without the presence of current/past MNV. |
| iRORA | Vertically aligned photoreceptor/outer retinal degeneration, RPE attenuation or disruption, and increased signal transmission into the choroid. Must not qualify as cRORA. |
| cRORA | Vertically aligned zone of hypertransmission of ≥250μm, zone of attenuation or disruption of RPE band of ≥250μm, and evidence of overlying photoreceptor degeneration whose features include outer nuclear layer (ONL) thinning, external limiting membrane (ELM) loss, and ellipsoid zone (EZ) or interdigitation zone (IZ) loss. Must exclude scrolled RPE or other signs of RPE tear. |
Table 1: Courtesy of the authors.
Figure 7 features an OCT image with labels of key characteristics of GA.

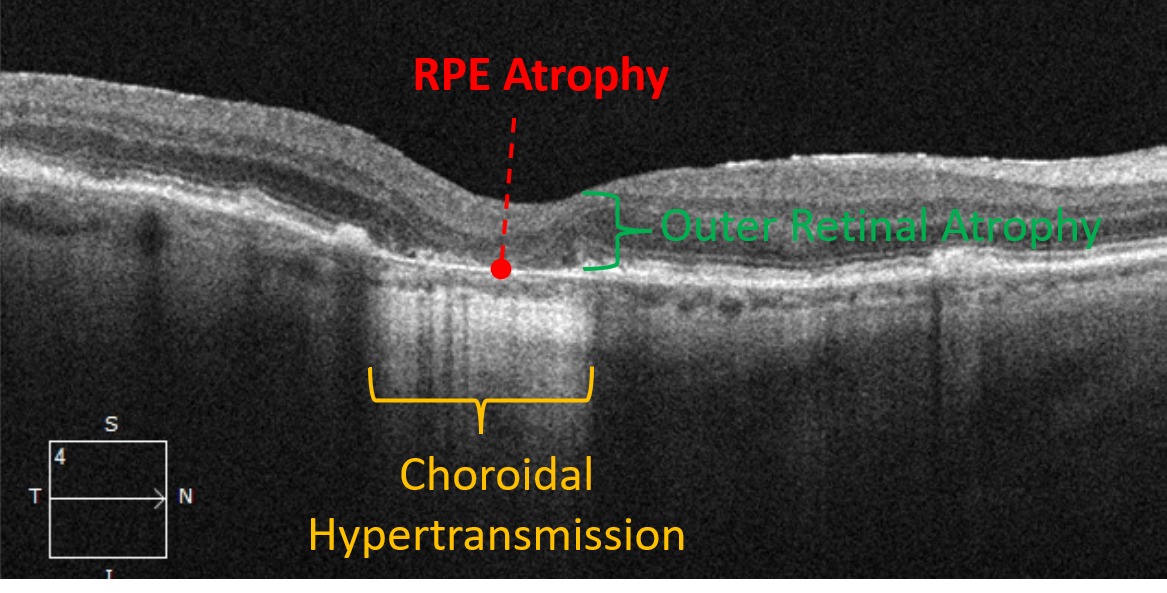
Figure 7: Courtesy of Daniel Epshtein, OD, FAAO.
Imaging features that can be predictive of GA development and progression
Several imaging features have been found to be predictive in the development of GA, including certain drusen characteristics and pigmentary abnormalities.
In a study of individuals ≥49 years of age, characteristics of drusen that were strongly associated with the development of GA over a 15-year period included soft indistinct drusen, drusen within 500µm from the foveal center, and a total drusen area >375µm in diameter.54
Subretinal drusenoid deposits
The presence of subretinal drusenoid deposits (or reticular drusen), RPE depigmentation, and hyperpigmentation was also strongly associated with the development of GA.54 These features can be valuable in identifying patients who may benefit from currently available and future GA treatments.
Further, Spaide et al. determined that SDD regression, while previously unrecognized as a sign that could develop in late AMD, could be a differentiation between GA and outer retinal atrophy (ORA).55 Even with an intact RPE, this latter condition has been characterized by the collapse of the outer nuclear layer, an attenuated ellipsoid zone, and a thin choroid.55
OCT-reflective foci and drusen substructures
Other OCT imaging features, including the presence of intraretinal hyper-reflective foci, were found to be a signal of progression to late AMD (cRORA) alone, though no correlation was evident for MNV alone over 1 year.56
Observing OCT-reflective drusen substructures, including low- and high-reflective cores, conical debris, and split drusen, these findings were associated with an increase in GA area over 2 years.57 Additionally, the presence of calcified drusen with heterogeneous internal reflectivity was associated with progression to advanced AMD (neovascular AMD or GA) over 1 year.58
Finally, the appearance of persistent hyper-transmission defects with a minimum size of 250µm on en-face swept-source OCT scans was directly correlated to an increased risk of GA progression.59
Figure 8 shows en-face OCT imaging revealing drusen regression and GA progression.

Figure 8: Courtesy of Daniel Epshtein, OD, FAAO.
Photoreceptor loss
Recent studies have begun to hone in on photoreceptor integrity, as photoreceptor loss is part of the criterion for GA. Reiter and colleagues demonstrated a significant association between the junctional zone and GA growth after 12 months. This suggests that the perifoveal area may be a predictor of GA growth.60
It has also been demonstrated that qualitatively, progressive photoreceptor degeneration outside GA correlated with GA progression rates.61 Quantitatively, ellipsoid zone-loss-to-GA boundary distance and thickness of the outer nuclear layer, outer segment, and inner segment were all associated with future progression rates.62
These studies suggest that photoreceptor loss and thinning identified on OCT imaging could be an important signal for progression beyond GA lesion size.60,61
Multifocal lesions
Certain features of GA have been found to predict faster rates of growth, specifically multifocal lesions. Studies have determined that multifocal lesions tend to grow at a quicker pace compared to unifocal lesions.
Beyond the quantification of lesions, shape matters in that irregularly shaped lesions have higher growth rates than more circular lesions.62,63 Extrafoveal lesions carry greater significance since they have been found to have higher growth rates than foveal lesions.45
Outside of OCT, FAF imaging studies have identified banded or diffuse patterns that can be linked to higher growth rates than lesions with no abnormal FAF pattern or focal FAF patterns.64
Figure 9 shows a fundus autofluorescence image with a central line scan on the left illustrating central atrophy along perifoveal multifocal lesions. On the right is the corresponding OCT image.

Figure 9: Courtesy of Daniel Epshtein, OD, FAAO.
Targeted GA treatment: The here and now
The complement system has been explored through various studies demonstrating that it can play a pivotal role in the development of GA. With this in mind, a myriad of complement genes have been both discovered and linked to AMD in genome-wide association studies.65,66
When the common risk allele (Y402H) of the CFH gene is present in individuals of European ancestry, the odds of GA were estimated to be 2.5 times higher.67 Beyond genetic studies, benchwork in histology has found complement proteins within drusen coupled with elevated levels of complement proteins in postmortem outer retinal tissue with patients who had AMD.68-70
As one might expect, these same activated complement products in plasma also appear to be elevated in individuals with GA.71 Subsequently, two drugs targeting the complement system have been commercially FDA-approved—Syfovre (pegacetacoplan injection) 15mg/0.1 mL and Izervay (avacincaptad pegol intravitreal injection) 2mg.
There are a plethora of other chemical entities currently in clinical investigational phases for GA treatment.
Pegcetacoplan
These two FDA drugs specifically targeting the complement cascade with phase 3 efficacy and safety data up to 24 to 30 months in GA to date include pegcetacoplan (Apellis Pharmaceuticals, Waltham, MA) and avacincaptad pegol (Iveric Bio, An Astellas Company, Cranbury, NJ), which are complement C3 and complement C5 inhibitors, respectively.72,73
Clinical studies on the safety and efficacy of pegcetacoplan
The efficacy and safety of pegcetacoplan administered via intravitreal injections every month or every other month in patients with GA were examined in the multicenter, randomized, double-masked, sham-controlled DERBY and OAKS phase 3 studies.73,74
In the OAKS study (n=637), they found a significant reduction in GA lesion growth (mm2) with pegcetacoplan monthly (22% reduction) and pegcetacoplan every other month (16% reduction) compared with sham at month 12.
Conversely, the DERBY study (n=621) failed to find a significant reduction.74 When Apellis Pharmaceuticals did a combined analysis of OAKS and DERBY, they uncovered a reduction in growth with pegcetacoplan monthly (17% reduction) and pegcetacoplan every other month (14% reduction) at month 12.74
Treatment-emergent adverse events for pegcetacoplan
When looking at the safety data, this demonstrated rates of serious ocular treatment-emergent adverse events (TEAEs) of 1.4% for pegcetacoplan monthly, 1.9% for pegcetacoplan every other month, and 0.0% for sham in OAKS.
Separately, DERBY illustrated TEAEs of 0.5% for pegcetacoplan monthly, 0.0% for pegcetacoplan every other month, and 1.0% for sham.75 In both OAKS and DERBY, the investigators determined the rates of exudative AMD were 5.2%, 4.7%, and 1.4% for pegcetacoplan monthly, every other month, and sham in OAKS, and 6.8%, 3.4%, and 3.4% in DERBY.75,76
2-year data on pegcetacoplan efficacy
When looking at the pegcetacoplan data set further out in time, the rate of GA lesion growth through 24 months compared to sham clocked in for OAKS at 22% monthly and 18% every other month, while DERBY registered 18% monthly and 17% every other month.77,78
Further, the analysis illustrated pegcetacoplan-treated patients compared to sham demonstrated preservation of 5.6 letters, equivalent to more than one line of vision on an ETDRS chart, as measured by BCVA along with a 4.1-point benefit in vision-related quality-of-life outcomes, as measured by the National Eye Institute Visual Function Questionnaire (NEI-VFQ-25).79,80
In the 24-month analysis of OAKS (n=456) and DERBY (n=435), pegcetacoplan did appear to slow both photoreceptor (Table 2) and RPE cell (Table 3) loss with a meaningful reduction noted compared to sham (all p-values nominal) in the following manner.79
Table 2 summarizes the 24-month data on reduced photoreceptor cell loss with pegcetacoplan.79
| Study | Monthly | Every Other Month |
|---|---|---|
| OAKS | 53% (p<0.0001) | 46% (p<0.0001) |
| DERBY | 47% (p<0.0001) | 46% (p<0.0001) |
Table 2: Courtesy of Apellis Pharmaceuticals.
Table 3 summarizes the 24-month data on reduced RPE cell loss with pegcetacoplan.79
| Study | Monthly | Every Other Month |
|---|---|---|
| OAKS | 22% (p=0.0002) | 20% (p=0.0002) |
| DERBY | 27% (p<0.0001) | 21% (p=0.0005) |
Table 3: Courtesy of Apellis Pharmaceuticals.
30-month data on pegcetacoplan efficacy
Finally, the GALE extension study (n=792) exhibited pegcetacoplan’s continuous improvement in efficacy through 30 months for both monthly and every other month injections—consistent with the DERBY and OAKS studies.81
For background, sham patients from both original phase 3 trials were allowed to transition to receiving pegcetacoplan in the extension study after Month 24. A projected sham arm was used to gauge GA lesion growth as a treatment for the remaining 6 months (to Month 30).
The study data revealed a reduction in GA lesion growth for both monthly (39%; p<0.0001) and every other month (32%; p<0.0001) injections vs. the projected sham arm (all p-values nominal) from Month 24 to 30.82 Further, investigators determined there was a reduction in GA lesion growth by up to 45% (monthly) and 33% (every other month) in patients with nonsubfoveal lesions.82
For the safety profile, there were no serious adverse events (SAEs) of ischemic optic neuropathy (ION) or endophthalmitis reported for both treatment groups; however, one SAE of ION was noted in the monthly group.
The investigators reported an overall IOI rate of 0.26% per injection among all patients treated with pegcetacoplan.83 Lastly, there were no reported cases of retinal vasculitis in the pegcetacoplan clinical trial program, after more than 24,000 injections.84
Note: Since pegcetacoplan was FDA-approved, 100,000 vials have been commercially distributed throughout the United States.84 There have been eight reported cases of retinal vasculitis parsed out into occlusive (five) and non-occlusive (three).
Apellis has recommended that ECPs immediately discontinue the use of 19-gauge filtering needles in favor of the 18-gauge version as a precautionary measure.
Avacincaptad pegol
The second molecule recently approved for the treatment of GA, was investigated through several studies to examine the efficacy and safety of avacincaptad pegol 2mg and 4mg administered through monthly intravitreal injections in patients with GA.
Clinical studies on avacincaptad pegol
GATHER1, a randomized, double-masked, and sham-controlled phase 2/3 study, found a significant reduction in GA growth rate (mm) with both avacincaptad pegol 2mg (27% reduction) and avacincaptad pegol 4mg (28% reduction) compared with sham at Month 12.85
Further, there was no evidence or reported serious ocular adverse events in avacincaptad pegol groups or sham groups at the 12-month mark.85,86 The most common ocular adverse events related to the injection procedure were conjunctival hemorrhage, conjunctival hyperemia, punctate epithelial keratitis (PEK), and increased intraocular pressure (IOP).86
The rates of choroidal neovascularization (CNV) reported were 9.0%, 9.6%, and 2.7% in the avacincaptad pegol 2mg and 4mg and sham groups, respectively.85,86
2-year data on avacincaptad pegol
GATHER2 was a randomized, double-masked, sham-controlled, 24-month trial that evaluated monthly and every-other-month intravitreal injections of avacincaptad pegol 2mg compared with sham in patients with GA.
The data for the first 12 months, for which patients received monthly avacincaptad pegol 2mg or sham, met its primary objectives with a significant reduction in observed GA growth rate (mm2) with avacincaptad pegol 2mg (17.7% reduction) compared with sham at month 12.86
Similar to OAKS and DERBY from the pegcetacoplan studies, GATHER2 had a consistent safety profile with GATHER1 with the most frequently reported ocular adverse events related to the injection procedure.
A comprehensive surveillance of CNV was performed by the investigators, with the reported incidence of CNV in the study eye at 12 months being 6.7% for avacincaptad pegol 2mg compared with 4.1% for sham.86
Snapshot of post hoc analyses
With respect to iRORA conversion to cRORA as well as reduced photoreceptor loss and thinning, the investigators demonstrated through a post hoc analysis of the FILLY phase 2 study that pegcetacoplan lowered these rates compared with sham.87,88
Shifting to GATHER1, a post hoc analysis also found that avacincaptad pegol reduced the progression of drusen to iRORA/cRORA, the progression from iRORA to cRORA, and a reduction in the growth of ellipsoid zone degradation, all compared to sham.89
A final word: Hope
It is clinically and socially evident that GA can profoundly affect activities of daily living or overall psychological well-being due to severe vision loss.90 Subsequently, the consequences can be rather devastating to patients in that it can impact their ability to read, write, drive, or even recognize the faces of family and friends.91
While this might paint a less than favorable prognosis for GA patients, there has been only what one could call a tsunami of pharmacologic and technological innovation in recent years that has revolutionized the management of retinal diseases, including GA. A multitude of these advancements have illustrated enhanced efficacy to potentially improve the quality of life for patients while concurrently reducing complications.
The proverbial “light at the end of the tunnel” is that there is a bright future that lies ahead—countless other therapeutics and delivery systems are in various stages of development, promising further improvements as the new frontier in the management of retinal disease.
Consequently, the overarching goal will be to target some level of retinal tissue rehabilitation or even restoration coupled with improved daily function in GA patients with significant visual impairment to blindness, which is uncharted territory in the retina space.
In a word, there is “hope”!


