



Syphilis is a sexually transmitted infection with the spirochete Treponema pallidum that can progress to neurosyphilis, otosyphilis, and ocular syphilis if left untreated.
Recently, there has been an uptick in reported cases of ocular syphilis.1 The reasons for this are not entirely understood. The increase in cases is concurrent with an overall increase in syphilis cases since 2000, particularly in men who have sex with men.
However, increasingly, syphilis is seen in people from both sexes and all sexual orientations.2,3 In one instance, five women were found to have ocular syphilis from a common sexual partner.
This raises questions as to whether there may be an as-of-yet unidentified strain of T. pallidum that may be more likely to manifest itself as ocular syphilis.4
Overview of ocular syphilis
An understanding of the clinical features of ocular syphilis is crucial as it may be the initial presentation of the disease. Most likely, patients may have signs and symptoms of disseminated infection and they may not volunteer to have the physician perform an ophthalmic exam.
The exact incidence of ocular syphilis in the United States is not known. The British Ocular Syphilis Study, one of the most extensive studies of ocular syphilis to date, showed that it affected approximately 0.6% of all those infected with syphilis.3
Failure to identify syphilis may worsen outcomes not only because of disease progression but also because improper treatment (i.e., with topical or systemic corticosteroids alone) may exacerbate the infection.
Ocular syphilis in patients with HIV/AIDS
Around 55,000 people in the US are infected with syphilis annually, most of whom are men. Significantly, it is commonly associated with human immunodeficiency virus (HIV) infection. Ocular syphilis has been the initial presentation leading to a diagnosis of HIV, underscoring the importance of early recognition.5
In patients who have acquired immunodeficiency syndrome (AIDS), syphilis manifestations in general are often more severe.2 Ocular manifestations in AIDS patients may be more common and vary slightly from individuals who do not have AIDS.
Despite this, ophthalmic involvement does not appear to be worse clinically or have poorer outcomes in this population.
The 4 stages of syphilis
Syphilis may be seen in four stages—primary, secondary, latent, and tertiary—depending on the physical spread of the disease.
The primary stage is characterized by a painless chancre sore at the site of infection—usually the genitals, anus, or mouth. If not treated, the disease progresses to the secondary stage after weeks to months. Systemic symptoms such as fever and fatigue are usually present, along with skin rash on the palms and soles and lymphadenopathy.
Syphilis may enter a latent stage, during which the carrier becomes asymptomatic. This stage may last for years. Following the latent stage, some individuals may progress to a tertiary stage. Manifestations in the tertiary stage include damage to the cardiovascular, central nervous, skin, and other organs. Tertiary syphilis can be life-threatening and cause significant and irreversible damage.
At which stage does ocular syphilis appear?
A common misconception is that ocular syphilis is seen in more advanced stages of the disease. However, ocular syphilis can occur at any stage. Its appearance does vary throughout syphilis progression, as we will discuss here.
However, it is important to note that the manifestations of ocular syphilis are highly variable and cannot be reliably employed for syphilis staging. Ocular syphilis commonly occurs as much as 6 months after the initial infection when many of the systemic symptoms have resolved.6
Clinical features of ocular syphilis
Primary syphilis
Primary syphilis manifestations are due to direct inoculation of the bacteria at the site. Therefore, primary syphilis ocular manifestations are more superficial, including chancre sores of the eyelid and conjunctiva. This is generally thought to be due to contact with a contaminated surface, such as hands and fingers.7
Figure 1 demonstrates an ulceration above the external canthus of the left eye.


Figure 1: Courtesy of BMC Infectious Diseases.
Secondary syphilis
In secondary syphilis, T. pallidum has disseminated and may, therefore, present deeper in the uvea. Anterior uveitis is one possible presentation; however, posterior uveitis and panuveitis are more common.3
Figure 2 is a color fundus photograph of a case of macular placoid syphilis with characteristic retinal pigment epithelium (RPE) hyperpigmentation.


Figure 2: Courtesy of David Almeida, MD.
Anterior uveitis typically presents with symptoms of unilateral pain, redness, blurred vision, and sensitivity to light. Clinical signs may include lid edema, circumcorneal congestion, keratic precipitates, aqueous cells, flare, miosis, iris nodules, and posterior synechiae.9
While anterior uveitis is a common finding in ocular syphilis, it is not specific to or diagnostic of the disease, as there are a variety of causes of anterior uveitis. Posterior uveitis encompasses several presentations, including retinitis, acute syphilitic posterior placoid chorioretinitis (ASPPC), and central retinal artery or vein occlusion.
Figure 3 demonstrates syphilitic chorioretinitis with optic disc edema.

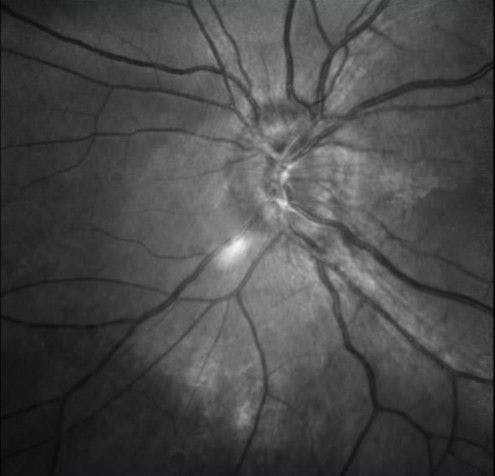
Figure 3: Courtesy of Cory Lappin, OD, MS, FAAO.
Figure 4 illustrates syphilitic chorioretinitis on salt-and-pepper fundus.

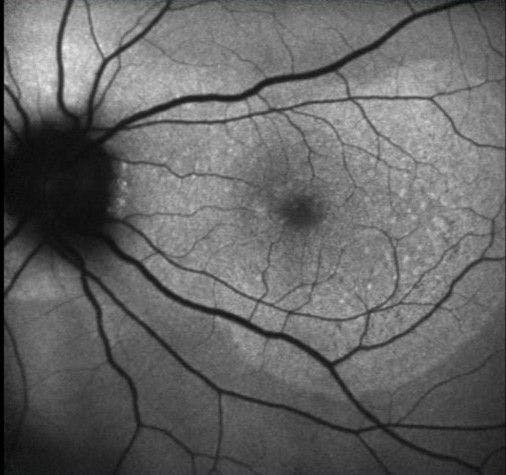
Figure 4: Courtesy of Cory Lappin, OD, MS, FAAO.
Retinitis in ocular syphilis often presents with a “ground glass” appearance and is frequently associated with retinal vasculitis.10 However, retinitis in syphilis can take several appearances, and no one presentation is pathognomonic. One unique characteristic of syphilitic retinitis is its relatively fast response to treatment compared to viral retinitis, which may support the diagnosis.
A strong association between syphilitic retinitis and HIV co-infection has been found. This is important for clinicians to understand as it may be confused with cytomegalovirus (CMV) retinitis in HIV/AIDS patients.11
ASPPC is considered among the classic and unique findings of ocular syphilis. Gass et al. framed our understanding of ASPPC with their description of “vitritis associated with bilateral large, solitary, placoid, pale-yellowish subretinal lesions usually showing evidence of central fading and a pattern of coarsely stippled hyperpigmentation of the pigment epithelium.”12
Tertiary syphilis
In tertiary syphilis, gummas, or granulomatous lesions that scar in a tumor-like growth, are a common finding. Gummas can involve the eyelid and other tissue surrounding the eye, leading to severe discomfort and complications.
The most common finding in tertiary syphilis relating to the eye is orbital periostitis. Common symptoms of orbital periostitis include pain, swelling, redness, and sometimes a palpable mass around the eye socket.
Argyll Robertson pupils (AR pupils) were once considered among the characteristic clinical findings of neurosyphilis in tertiary syphilis. An AR pupil is a medical condition in which pupils constrict in accommodation (focusing on a nearby object) but not to light exposure. (“light-near dissociation”).
However, with time, the incidence of tertiary syphilis has declined, and the proportion of non-syphilitic AR pupils has increased, caused by diabetes mellitus, neurosarcoidosis, chronic alcoholism, encephalitis, multiple sclerosis, Lyme disease, and herpes zoster.13 Late syphilis infection should be considered in cases of AR pupils where the cause is unknown.
Congenital syphilis
The classic ocular finding in congenital syphilis is interstitial keratitis, part of Hutchinson’s triad, which includes Hutchinson’s teeth and sensorineural deafness.2 If left untreated, interstitial keratitis can progress to corneal scarring and permanent vision loss.
Figure 5 highlights stromal scarring with ghost vessels due to interstitial keratitis secondary to congenital syphilis.

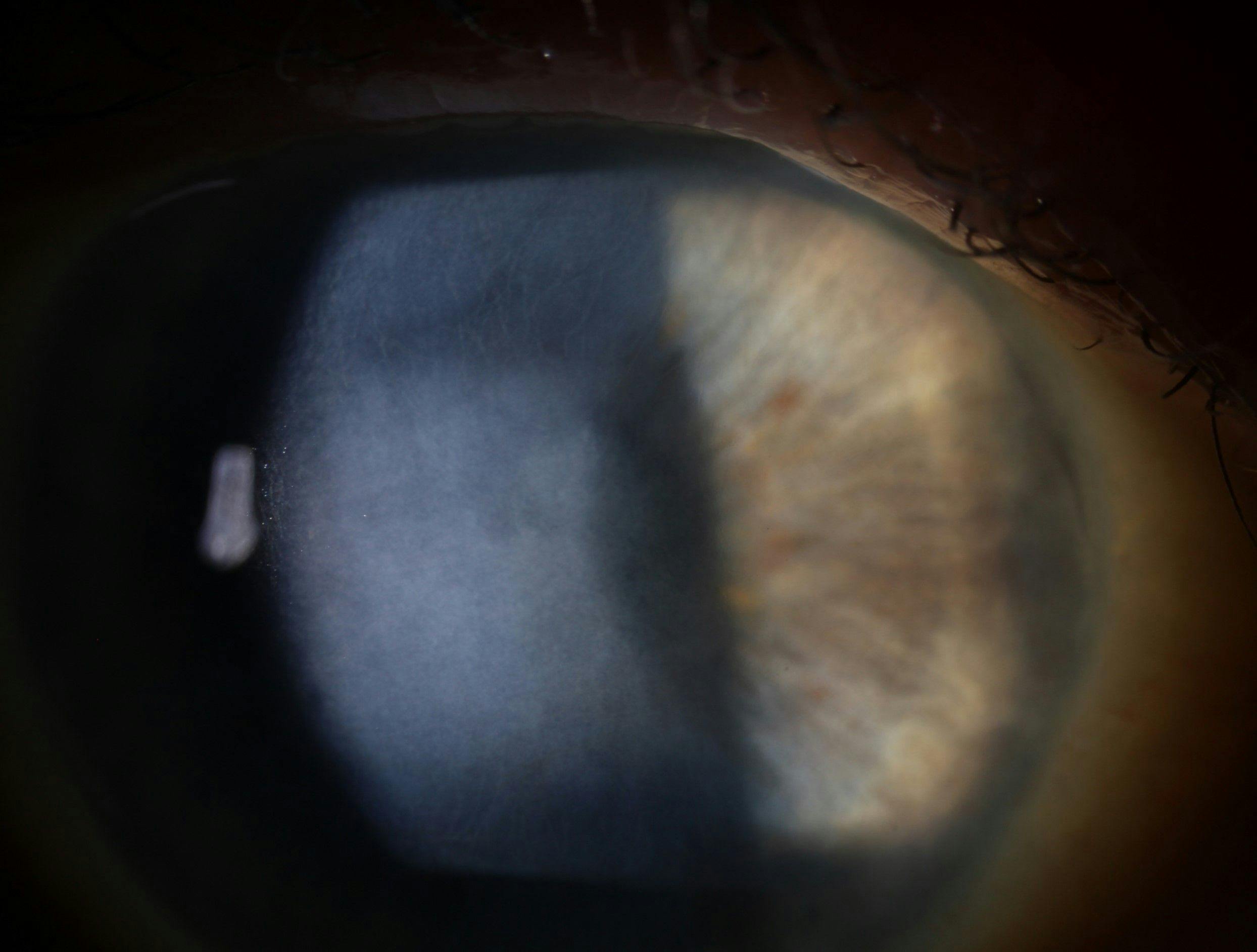
Figure 5: Courtesy of Cory Lappin, OD, MS, FAAO.
Syphilis diagnostic testing
Darkfield microscopy can be used to visualize the spirochetes and diagnose syphilis; however, this form of testing is not readily available in most clinical settings. Further, it requires tissue samples with high spirochete density—which is not practical in ocular syphilis.
Serologic tests are used for diagnosing syphilis, comprising nontreponemal and treponemal tests. Nontreponemal tests, like rapid plasma reagin (RPR) and venereal disease research lab (VDRL), are cost-effective and quantifiable, measuring antibody levels to assess infection activity. False results are possible.
Treponemal tests (e.g., fluorescent treponemal antibody-absorption [FTA-ABS], T. pallidum enzyme immunoassay [TP-EIA]) are more specific, detecting antibodies against treponemal antigens. Treponemal tests tend to remain positive for life, but some treated individuals may become seronegative after a few years.
The TP-EIA test is widely used. Combining different treponemal tests aids in diagnosing late latent syphilis.14
Management and treatment of neurosyphilis
Current Centers for Disease Control and Prevention (CDC) guidelines call for treatment of neurosyphilis, including ocular and otosyphilis, as follows:
- Aqueous crystalline penicillin G (18 to 24 million units per day, administered as 3 to 4 million units intravenous (IV) every 4 hours, or 18 to 24 million units daily as a continuous infusion) for 10 to 14 days.
- Procaine penicillin G (2.4 million units intramuscular [IM] once daily) plus probenecid (500mg PO four times a day), both for 10 to 14 days.
- Penicillin desensitization can be initiated for patients with severe penicillin allergies. An approved alternative treatment is ceftriaxone (2g IV or IM daily) for 10 to 14 days.15
- Combination therapy with topical or oral glucocorticoids can be initiated for ocular syphilis. This may also combat the possibility of the Jarish-Herxheimer reaction.
Conclusions
The rising incidence of ocular syphilis necessitates increased awareness and vigilance among healthcare providers. The broadening demographics affected by syphilis, now affecting individuals across all genders and sexual orientations, emphasizes the need for a comprehensive understanding of ocular syphilis manifestations.
Ophthalmic exams play a crucial role in early detection. The clinical features across the stages of syphilis highlight the diverse and sometimes unique ocular presentations, reinforcing the complexity of diagnosis.
Moreover, the association with HIV infection necessitates a broad approach to patient care. Timely recognition and appropriate management, as outlined in current CDC guidelines, are vital to prevent ocular complications and systemic disease progression.
Continued research is necessary to elucidate the reasons behind the increase in ocular syphilis cases and explore potential strains of Treponema pallidum that may contribute to its presentation. Ongoing clinical education will be key in addressing the challenges posed by ocular syphilis and improving patient outcomes in the face of this reemerging public health concern.


