


As a vision therapy and rehabilitation doctor, my approach to vision is a little different.
I think of our visual system as a five-pronged entity. The first leg asks and answers, “Can you see clearly?" and "Is your ocular health intact?” The next three legs encompass the “gathering” portion of our vision: vergence ability, accommodative ability, and oculomotor skills. The last leg is the "processing" part of vision where we take all the visual information we have gathered and put it together with other systems (auditory, vestibular, cognitive) to create a single, unified, clear understandable perception of our world, as shown in Figure 1.

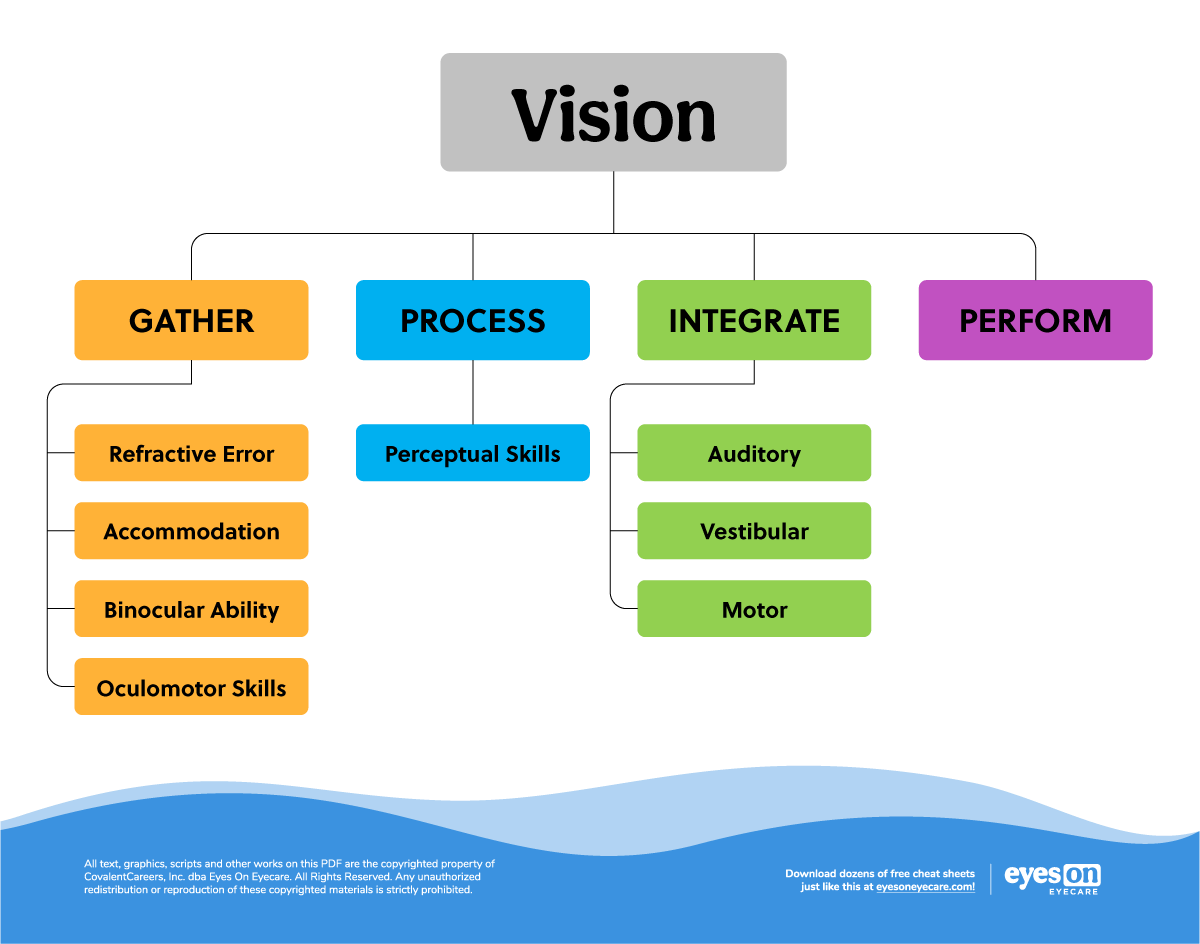
Figure 1
I cohost a weekly podcast dedicated to spreading the word that “Vision is More Than 20/20.” However, seeing clearly is the most important step in the visual process. If we cannot see well, the rest of the process doesn’t work well, no matter how strong the other prongs of vision are.
When it comes to writing prescriptions, I aim to have the patient see as clearly as possible and to feel the most comfortable in their visual world. As optometrists, we often think to just immediately throw someone in glasses, but contacts lenses are an important part of my treatment considerations to attain both of those goals. I am going to highlight three specific ways I use contacts in my office to benefit my patient population.
Refractive amblyopia
This is by far the biggest application of contact lenses in my office and one that I encourage any primary care optometrist to consider. First and foremost, amblyopia is defined as “the decrease in the best-corrected visual acuity of one eye, or less frequently both eyes, in the absence of any structural or pathological changes due to significant refractive errors, a constant, unilateral strabismus or some form of deprivation (i.e. cataract/ptosis) occurring before the age of 6.”1
We know that with refractive amblyopia there is a large difference in refractive error (either anisometropic or isometropic) between the two eyes resulting in decreased visual acuity in one or both eyes (see chart for amblyogenic risk factors).
Potentially Amblyopiogenic Refractive Errors2
| Isoametropia | Diopters |
|---|---|
| Anisometropia | |
| Astigmatism | >2.50D |
| Hyperopia | >5.00D |
| Myopia | >8.00D |
| Astigmatism | >1.50D |
| Hyperopia | >1.00D |
| Myopia | >3.00D |
AOA: Care of the Patient with Amblyopia
Once we identify the appropriate prescription for the patient, we must consider our options for treatment. Why I reach for contact lenses in these cases often is to address the visual distortions that come with higher, anisometropic prescription in glasses. We know that there are intrinsic aniseikonic effects with spectacles in these cases and even cosmetic distortions (i.e., one hyperopic eye vs. myopic eye) and other limitations with glasses in terms of the visual field. Another large factor in reaching for contacts in lieu of spectacles is that initially there may be frequent lens changes to help the patient adapt to their prescription.
If you are working with a young patient do not be afraid to offer this option to parents. I have fit kids as young as 5 or 6 in soft contact lenses. Yes, it must be the right parent and the right patient, BUT it is an option especially if the child is struggling to wear the glasses consistently. As an aside, I always recommend a pair of plano, polycarbonate lenses to be worn for protection with these patients.
Another benefit of wearing contacts with this population is from the treatment perspective. We know that amblyopia is a pervasive visual disorder that does not just affect visual acuity, but rather the functionality of the whole visual system. We see reduced contrast sensitivity, accommodation, oculomotor skills, and overall depression of the binocular system and stereopsis.3
I like to refer to amblyopia as a monocular manifestation of a binocular disorder and thus this dictates my treatment plan. Treatment with this population is based on the severity of the amblyopia, the patient’s age and commitment to resolving the amblyopia that often consists of patching, MFBF (monocular fixation in a binocular field), and vision therapy with lenses and prisms—all of which are easier to manage with contacts vs. glasses.
Head trauma/concussion patients
This population is unique for two reasons:
- Small prescriptions can make a huge difference in their visual function.
- Due to the instability in their visual systems, prescriptions are just needed temporarily or may change frequently.
In my opinion, contact lenses make both things easier to tackle because we can trial these small prescriptions and see how the patient responds. It is much cheaper to change a contact lens out when compared to frequently remaking glasses. One thing to note with this population is that they often also suffer from dry eye,4 so my recommendation is to offer a daily contact lens option to help reduce this comorbidity.
An additional consideration for this population is that they may require multiple different prescriptions depending on their different visual demands, so do not be afraid to write a few different prescriptions. I have a current patient that has "work contacts," "weekend contacts," and even "golf contacts."
Check out this recent podcast episode that highlights how the application of a contact lens dramatically changed a traumatic brain injury patient’s symptoms almost immediately!
Myopia management
Myopia management is a hot topic in the optometric world right now and for good reason: we know that by 2050, half of the world’s population will be myopic.5 We also know as eye care providers that myopia is not just as simple as needing a pair of distance glasses. There are true ocular health concerns that are associated with higher levels of nearsightedness.
The demographic of my practice specializing in vision therapy is skewed towards a huge number of young adolescents. These patients are often just starting to need glasses or are a few years into wearing them on top of struggling with other parts of their vision. I am already managing their visual function, so managing their myopia is a natural tie-in.
My treatment approach to any case is education and this is a critical part of myopia management. Every parent wants what is best for their child, so even if you are not practicing in a setting that allows for a ton of extra time, still be the provider that takes the few minutes to discuss what it means to be nearsighted, the future ocular health implications, the limitations to refractive surgery and the current treatment options available. Parents will be more on board with your treatment plan as they understand the options and why you want to intervene.
The Big Vision Therapy Question: To Take Insurance or To Not Take Insurance? Learn the pros and cons of each option from a veteran vision therapy & rehabilitation practice. Find out now >>
The way that I present the options to parents is straightforward: either we do something to address their child’s rapidly changing prescription or we do nothing. The treatment options I present include atropine, orthokeratology, or a soft contact lens that is designed to slow the progression of myopia. The new MiSight soft contact lens is included in this conversation.
I discuss the pros and cons of each option, give my recommendations and then put the ball in the parent’s court. I will note that my go-to choice is the MiSight contact lens—it has been a total game-changer with getting parents on board. It is something familiar to them (a soft contact lens) just with new technology. CooperVision has made the whole process user-friendly and easily accessible from the parent’s perspective.
At the end of the day, contact lenses should not be an afterthought or something the patient brings up that they want to "try," but rather it should be considered a critical tool in the optometrist’s toolbox to get your patients the best vision while also improving their visual function!
References
- Holmes J, Clarke M. Amblyopia. The Lancet. 2006;367: 1343-51.
- https://www.aoa.org/AOA/Documents/Practice%20Management/Clinical%20Guidelines/Consensus-based%20guidelines/Care%20of%20Patient%20with%20Amblyopia.pdf
- Niechwiej-Szwedo E, Colpa L, Wong AMF. Visuomotor Behaviour in Amblyopia: Deficits and Compensatory Adaptations. Neural Plast. 2019;2019:6817839. Published 2019 Jun 9. doi:10.1155/2019/6817839
- Lee CJ, Felix ER, Levitt RC, Eddy C, Vanner EA, Feuer WJ, Sarantopoulos CD, Galor A. Traumatic brain injury, dry eye and comorbid pain diagnoses in US veterans. Br J Ophthalmol. 2018 May;102(5):667-673. doi: 10.1136/bjophthalmol-2017-310509. Epub 2017 Aug 26. PMID: 28844048.
- Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, Wong TY, Naduvilath TJ, Resnikoff S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016 May;123(5):1036-42. doi: 10.1016/j.ophtha.2016.01.006. Epub 2016 Feb 11. PMID: 26875007.


