When we examine the
optic nerve head in our patients, we usually anticipate seeing that it is mainly circular with distinct margins, pink in color, and with a centred depression that is the cup. When optic nerve anomalies are discovered, it is critical to distinguish between congenital and pathological origins since some irregularities may necessitate extra testing, treatment, and management.
Optic nerve anomalies can range from benign to sight- and life-threatening. This article will review the diagnosis and management of common (and not-so-common) optic disc anomalies that can present clinically.
Congenital optic disc abnormalities
Congenital disc abnormalities can appear in a wide variety of clinical presentations. Some are linked to
systemic and/or neurological disorders, while others are limited to the eye. Patients can have a plethora of visual symptoms with congenital disc abnormalities. These range from no visual symptoms to reduced acuity, visual field, and/or color vision.
Optic disc conditions determined by disc size
Optic nerve hypoplasia
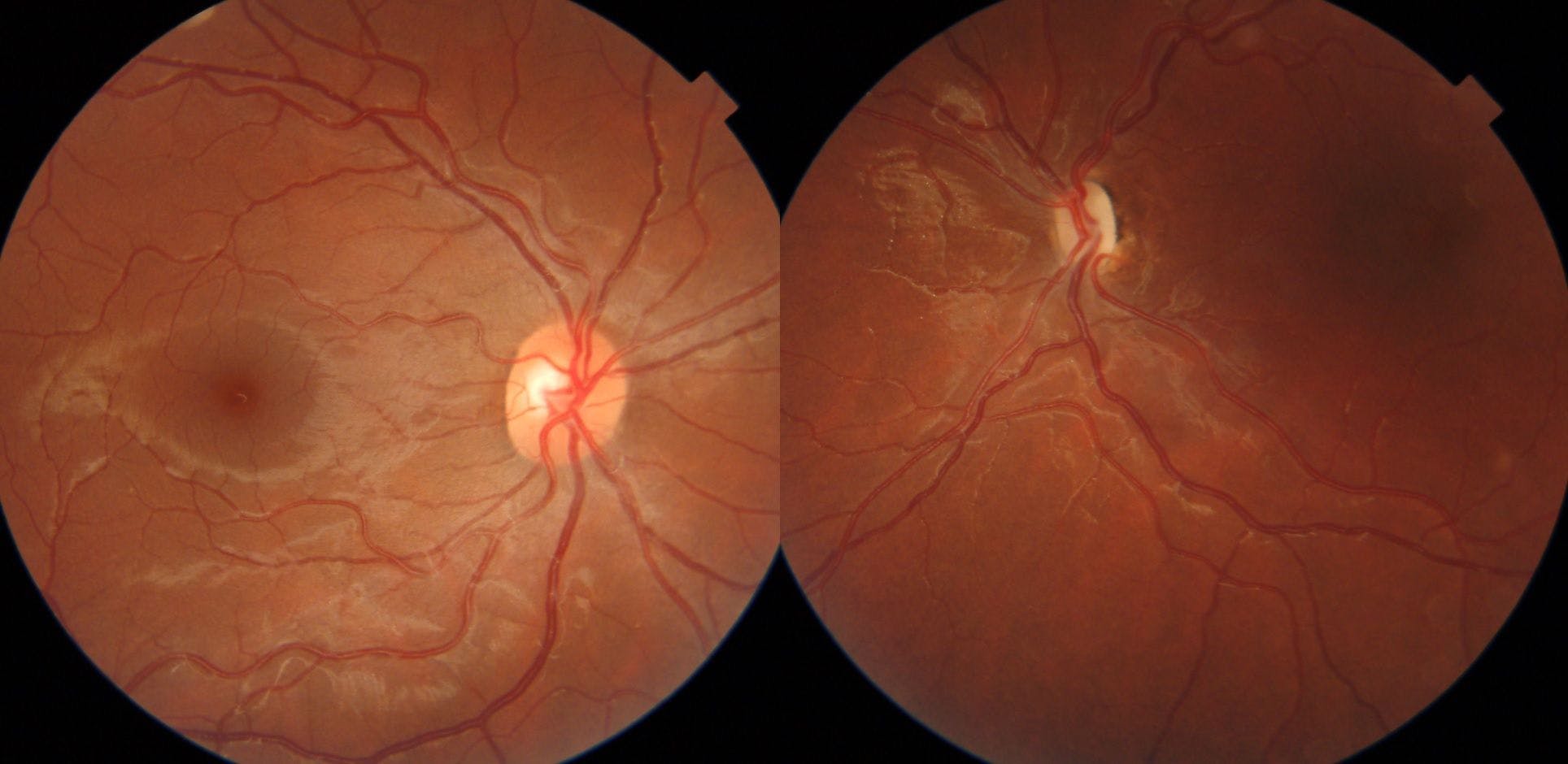
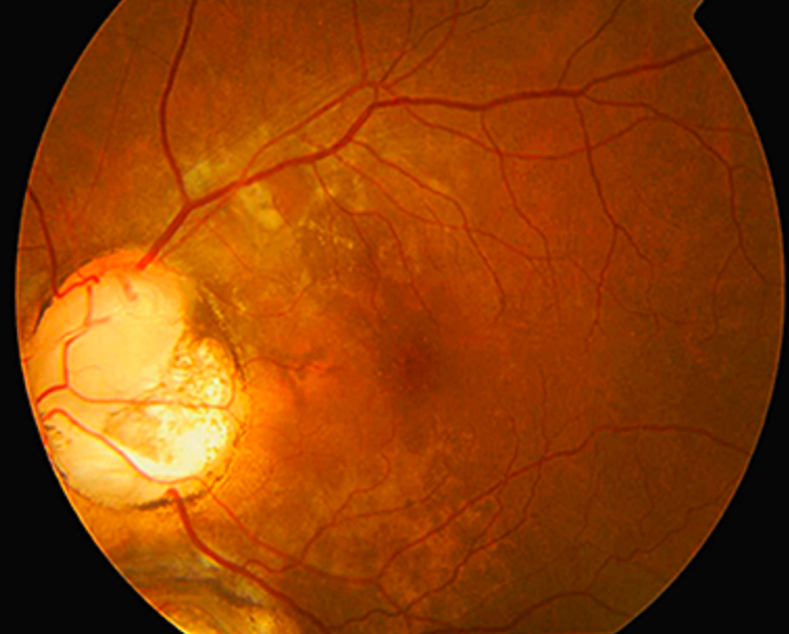
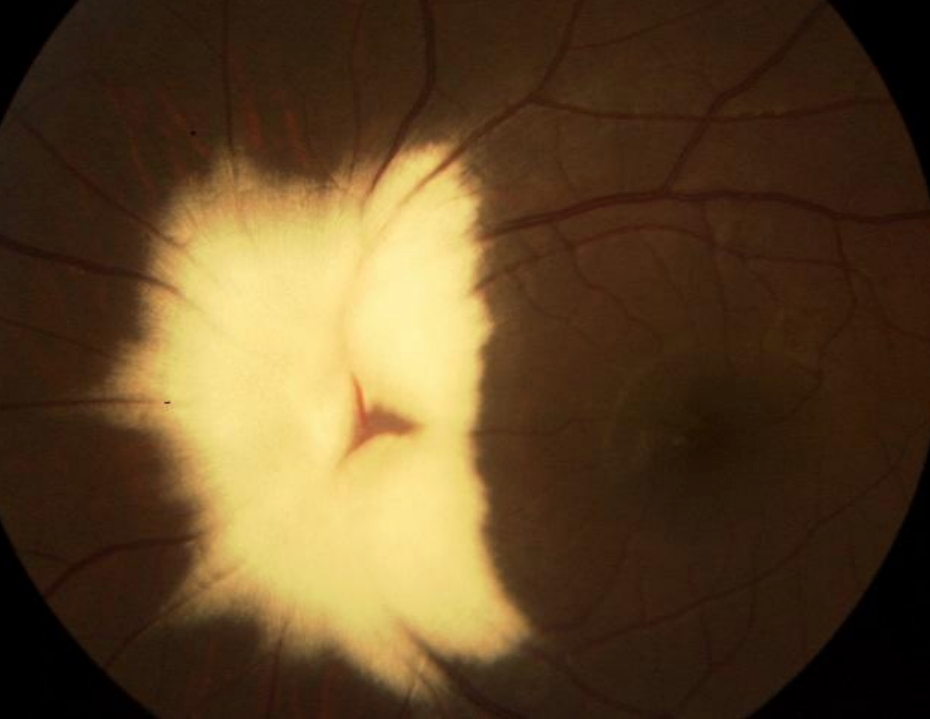
Figure 1 highlights fundus photography of optic nerve hypoplasia OS.
Figure 1: Courtesy of Kevin Cornwell, OD
Optic nerve hypoplasia (ONH) is a congenital, non-progressive developmental defect that can be characterized by a tiny optic disc, peripapillary "double-ring sign," vascular tortuosity, and nerve fiber layer thinning.1 ONH occurs bilaterally in 65% of cases and is the third largest cause of childhood blindness in the United States, behind cerebral palsy and retinopathy of prematurity.1
ONH is characterized during prenatal development between the sixth week and the fourth month of gestation by a reduction in axons caused by apoptotic processes triggered by the incomplete creation of other axons.1
ONH can be caused by a variety of factors, including premature delivery, young maternal age, gestational diabetes, fetal infection, fetal alcohol syndrome, or the use of certain drugs during pregnancy.
1 ONH is primarily diagnosed clinically based on a
fundus examination of the optic disc, which typically reveals a tiny optic disc with large vasculature.
More specifically, ONH is probable if the gap between the disc and the macula is >3-disc diameters (DD), as shown in Figure 1.1 Depending on the level of axonal damage, visual acuity might range from 20/20 to no light perception (NLP).1 Visual field defects are prevalent, and every visual field defect linked with ONH reflects the intensity and distribution of axonal deficiency.1
“Patients with uniformly distributed mild axon regression will not have obvious visual field abnormalities.”
Patients with progressive, diffuse axon deficits may have more defects in their visual field. Furthermore, individuals with focal axon regression may have a corresponding focal visual field defect.1 Strabismus commonly appears around 3 months of age if it is bilateral.1 Systemic associations such as neurologic and endocrine disorders should be evaluated in ONH patients.1
Visual evoked potential (VEP) testing and B-scan ultrasonography might be useful when the diagnosis is ambiguous. VEP testing would reveal a lower amplitude in VEP, but an electroretinogram would be normal in patients with ONH, and B-scan ultrasonography would reveal a tiny optic nerve.1
Megalopapilla
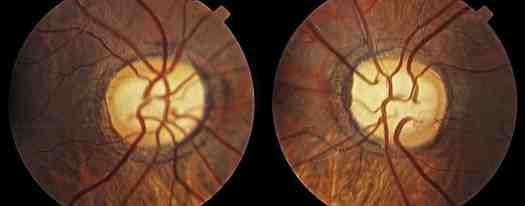
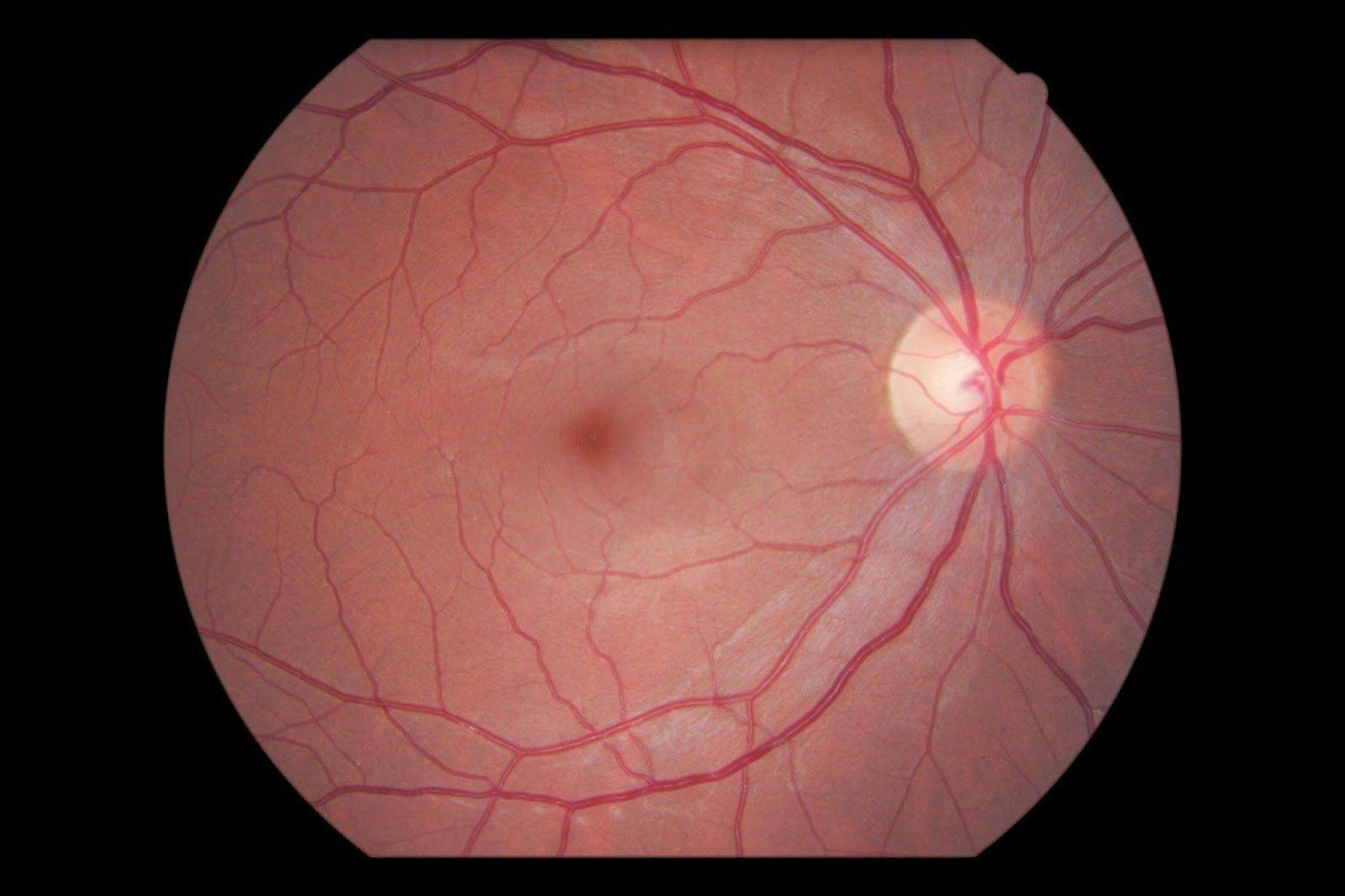
Figure 2 features fundus photography of bilateral megalopapilla.
Figure 2: Courtesy of Michael Cooper, OD
Megalopapilla is a rare condition characterized by an enormously large optic disc. The optic disc diameter in these patients is usually greater than 2.1mm and with a normal disc shape.2 It can be associated with larger than normal blind spots and, on rare occasions, impaired visual acuity.2 The typical optic cup is replaced with a massive excavation that displaces the neighboring neuroretinal rim (as shown in Figure 2).2
The bilateral and unilateral appearance may be readily mistaken with advanced glaucoma due to the increased cup size; however, the disc area in megalopapilla is substantially larger than in glaucomatous eyes.2
Overall, megalopapilla is defined by a huge optic nerve head with an expanded cup, but more importantly, it is characterized by a normal rim volume, normal intraocular pressures (IOP), and a visual field that does not show typical glaucomatous defects. It is imperative to differentiate this condition from true
glaucomatous optic neuropathy.
2Download the Optic Disc Abnormalities Cheat Sheet
📝
Optic Disc Abnormalities Cheat Sheet
Use this cheat sheet to review how to identify, diagnose, and treat optic disc abnormalities.
Optic disc conditions defined by disc conformation
Tilted disc syndrome
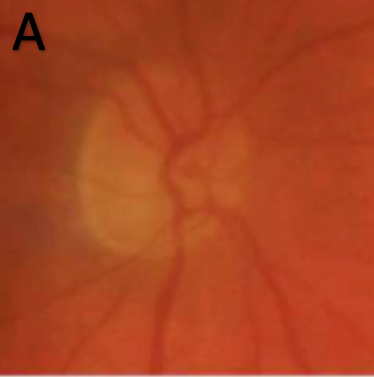
Figure 3 shows fundus photography of tilted disc syndrome.
Figure 3
Tilted disc syndrome (TDS), also known as Fuch's coloboma, is a congenital condition with a 1 to 2% frequency; of these, 80% are bilateral.3 It is a clinical disorder in which the optic nerve seems to enter the eye at an oblique angle instead of perpendicularly. TDS is distinguished by an elevation of the superotemporal disc, posterior displacement of the inferonasal disc, and retinal vascular situs inversus.3
TDS is associated with an inadequate closure of the embryonic optic fissure.3 High myopia, color vision changes, visual field defects, and retinal abnormalities can all be associated with TDS patients.3
Common related retinal abnormalities include chorioretinal thinning, retinal pigment epithelium thinning, and peripapillary atrophy.3 A scotoma in the superior temporal quadrant is the most prevalent visual field defect identified in TDS patients.3 Best-corrected visual acuity is rarely altered and typically remains stable at 20/20.3 When no additional related ocular issues are discovered, TDS can be monitored with yearly comprehensive eye examinations.3
Morning glory syndrome
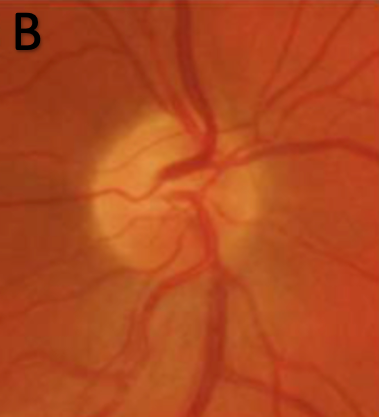
Figure 4 exhibits clinical photography of morning glory syndrome.
Figure 4
Morning glory syndrome (MGS) nearly always manifests unilaterally and is generally sporadic. No specific genetic abnormality has been linked to this optic disc abnormality.4 Physical examination reveals a large, excavated disc with a glial tuft that is centrally surrounded by peripapillary pigment changes, which may involve the macula and an aberrant retinal vascular pattern in affected individuals.4 MGS closely resembles the morning glory flower (Figure 4).
“MGS is caused by a change in embryonic development of the lamina cribrosa and posterior sclera.”
Entering acuity ranges from 20/20 to NLP, with just 30% achieving 20/40 or better.
4 Serous retinal detachments occur in 30% of morning glory patients as a result of tiny fissures in the peripapillary zone.
4 Afferent pupillary defects and visual field defects are common, particularly in unilateral conditions.
4 Management begins with an accurate diagnosis, followed by treatment of serous retinal detachments if present, as well as treatment of early amblyopia to improve visual acuity.
4MGS is frequently associated with central nervous system (CNS) problems like encephaloceles, corpus callosum agenesis, and endocrine abnormalities, thus, a full examination of the CNS using magnetic resonance imaging (MRI) and computed tomography angiography (CTA) is recommended.4
Optic disc coloboma
Figure 5 highlights fundus photography of optic disc coloboma.
Figure 5
Optic disc coloboma (ODC) is a congenital disorder with a 0.14% frequency in the general population and is generally sporadic.5 They can happen unilaterally or bilaterally and with similar frequency.5 ODC manifest themselves as finely defined, white, bowl-shaped, inferiorly decentered excavations that seldom involve the entire disc (Figure 5).5 ODC often affects the inferonasal portion of the disc and can also impact the retina, uvea, and sclera.5
“ODC is caused by an incomplete closure of the embryonic fissure.”
Microphthalmos, iris coloboma, ciliary coloboma, lens notching, neovascular membranes, macular holes, and retinal detachments are typical of ocular associations.
5 Retinal detachment is caused by tears in the fragile membrane that covers the coloboma, allowing liquid vitreous to enter and separate the subretinal space.
5In ODC individuals with a retinal detachment, vitrectomy using silicon oil has a high success rate.5 Visual acuity might differ clinically depending on the direct impact on the papillomacular bundle.5 In situations with poor visual acuity, management should include therapy for amblyopia.5
It is vital to emphasize the possible link between ODC and renal coloboma syndrome, which can cause serious kidney complications.5 Because related kidney problems can be fatal, patients diagnosed with ODC should be referred for a renal ultrasonography.5
Optic pit
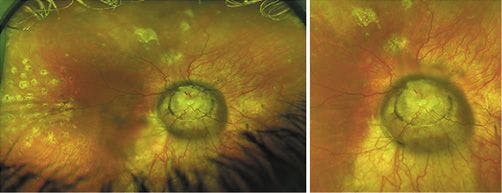
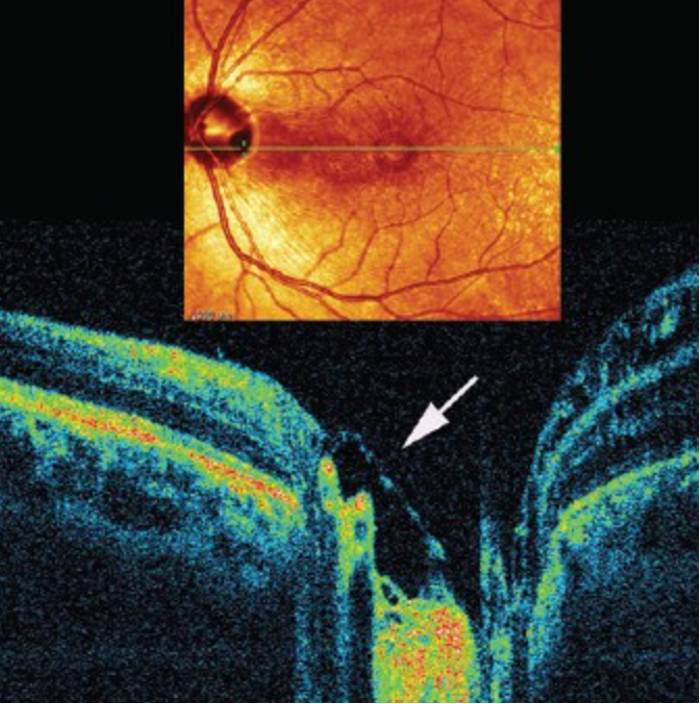
Figure 6 features fundus photography and optical coherence tomography (OCT) of optic nerve pits.
Figure 6
Optic nerve pits (OP) are uncommon and have no known systemic associations.
6 OP are thought to form during the first trimester of
pregnancy as grey, yellow, or black excavations in the optic disc and is usually unilateral.
6 In a fundus examination, they appear as a circular excavation with a size ranging from a quarter to an eighth of the disc at the edge of the optic nerve, more typically positioned temporally. (Figure 6).
6 There is normally one pit per optic disc, although two or three can occasionally develop.
6 Optic nerve pits arise due to partial closure of the fetal fissure.
6Unless the patient has a serous retinal detachment, OP has no effect on visual acuity.6 Large temporal pits are linked to an increased incidence of macular detachment.6 Visual symptoms generally appear when there is an accompanying serous macular elevation and are more common in the third and fourth decades of life.6 The two commonly accepted explanations for how OP-related significant macular detachments arise are liquid vitreous material entering the subretinal region via the optic pit or cerebrospinal fluid (CSF) from the optic nerve seeping into the subretinal space via the optic pit.6
“Fundus autofluorescence, OCT, and visual fields are all used to diagnose serous retinal detachments.”
Large schisis cavities in the macula exhibit hypo autofluorescence, and
OCT may establish the presence of a schisis cavity inside the macula.
6 The most common visual field defect found in OP is an arcuate scotoma, however, practically any visual field defect can be present due to nerve fiber displacement.
6 Early surgical management, such as juxtapapillary photocoagulation and vitrectomy, has shown the highest likelihood of improving visual acuity if a serous retinal detachment is present.
6Peripapillary staphyloma
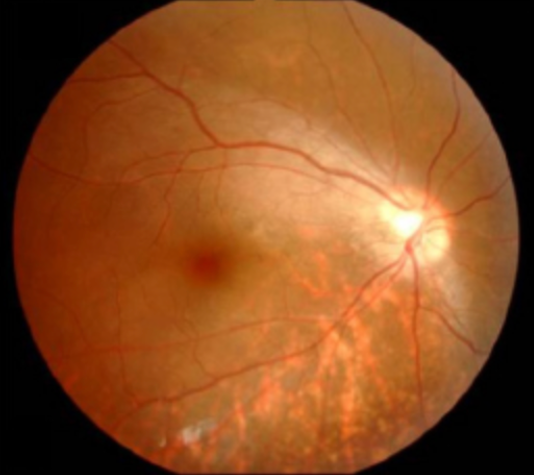
Figure 7 shows fundus photography of peripapillary staphyloma OD.
Figure 7: Courtesy of Kevin Cornwell, OD
Peripapillary staphyloma (PS) is an uncommon congenital condition that is generally unilateral.
7 It appears as a deep excavation around the optic disc (Figure 7).
7 The pathogenesis of staphylomas is unknown; however, it is suspected that diminished local choroidal and scleral resistance, resulting in a protruding Bruch's membrane, can result in staphylomas.
7 Peripapillary staphyloma is frequently linked with
highly myopic eyes owing to the sclera's higher elasticity due to its longer axial length, causing it to stretch and subsequently thin to generate these outpouchings.
7Staphylomas are frequently linked with choroidal neovascularization, retinoschisis, and glaucomatous optic neuropathy.7
In myopic individuals, symptoms of staphylomas may include decreasing vision. OCT allows doctors to assess the curvature and scope of the staphyloma. A computed tomography (CT) scan or MRI may be used in more advanced cases to view the staphyloma's posterior extension.7 Since the pathophysiology of PS is still unknown, there is no gold standard therapy. These individuals should be followed on a regular basis. Many patients may not need therapy and remain stable over time. Patients have a favorable prognosis since progression is often gradual.7
Conditions involving pseudo disc swelling
Hyperopia
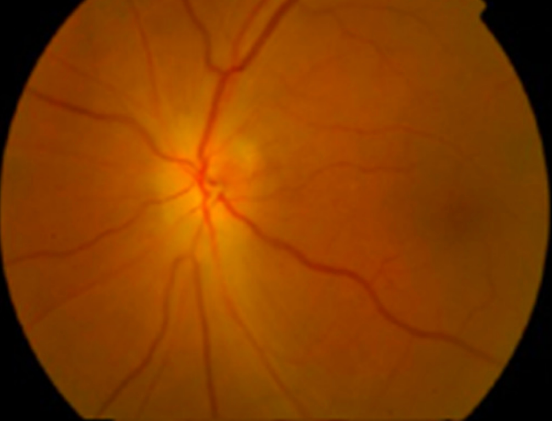
Figure 8 highlights fundus photography of hyperopia.
Figure 8
A nerve that is smaller than the typical diameter of an optic disc is frequently connected with
hyperopic eyes.
8 Because of the limited size of the optic cup caused by hyperopia, the axons exiting the disc are packed, producing the impression of a raised disc.
8 A hyperopic crowded disc can occur when a normal number of retinal axons pass through a narrow posterior scleral foramen, resulting in the appearance of a densely packed or crowded optic nerve head as the axons depart the globe.
8The optic nerve is often somewhat hyperemic in color, with little to no physiological cupping and indistinct superonasal and inferonasal borders (Figure 8).8 Annual comprehensive eye exams that include a dilated fundus exam, retinal imaging, and OCT can be used to monitor these individuals for any physical changes.8
Optic disc drusen
Figure 9 features fundus photography of optic disc drusen OU.
Figure 9: Courtesy of Kevin Cornwell, OD
Optic disc drusen (ODD) occur as a cluster of round to irregular whitish-yellow spots on the surface of the optic nerve.9 Drusen are bilateral 70% of the time.9 ODD is composed of globular concretions of calcium, amino and nucleic acids, mucopolysaccharides, and occasionally iron that are found anterior to the lamina cribrosa.9
Clinically significant results include a tiny and packed nerve full of distinct refractile aggregates, spontaneous venous pulsation, and the lack of Paton's lines.9 Such drusen are typically not apparent at a young age because they are hidden and appear to grow in size as they travel closer to the surface and become more visible with time.9
Fundus autofluorescence may make the drusen look more prominent, and because ODD may demonstrate substantial elevation, it is ideal for observing them using OCT.
9 Visual field abnormalities can cause an expanded blind spot, although they can also be non-specific.
9 Ultrasound B-scan can typically distinguish patients with edematous optic discs, and in whom drusen are suspected.
9 The long-term prognosis is favorable; patients are normally asymptomatic, but in severe situations, drusen can cause changes in visual acuity and visual fields from drusen development, placing additional pressure on the axons.9 ODD patients can typically be followed with yearly comprehensive eye exams; however, more advanced cases (e.g., significant visual field defect) may warrant off-label treatment to lower IOP.9
Myelinated fibers
Figure 10 shows fundus photography of myelinated fibers.
Figure 10
Myelinated nerve fibers (MNF) affect about 1% of the population and are bilateral in 20% of occurrences.10 MNF does not exist in normal retinal nerve fibers. The visual pathway begins myelination in the fifth month of pregnancy and finishes at birth at the lamina cribrosa; however, in this 1% of the population, myelinization extends past the lamina cribrosa along the nerve fibers of the optic nerve head and the sensory retina.10
MNF appears clinically as a flame-like patch of white or yellow color along the upper or lower margins of the optic disc (Figure 10).10 The abnormal placement of retinal oligodendrocyte glial cells that migrate before the development of the lamina cribrosa has been hypothesized as an etiology for this deformity.10
Visual acuity is seldom impacted, and
visual field abnormalities may exist depending on the extent of the MNF deficiency.
10 MNF can also exhibit distinct hypofluorescence on fundus autofluorescence due to the blockage of choroidal fluorescence.
10 The primary treatment for MNF is to treat any accompanying ocular disease; otherwise, annual comprehensive eye examinations are indicated to monitor the condition.
10Acquired optic disc abnormalities
Papilledema
Figure 11 exhibits fundus photography of papilledema.
Figure 11
Papilledema is disc swelling caused by elevated intracranial pressure, with idiopathic intracranial hypertension (also known as pseudotumor cerebri) being the most prevalent cause.
11 Although the actual cause of papilledema is uncertain, overweight or obese women of reproductive age are at a higher risk of developing it.
11 Bilateral disc enlargement with blood vessel obscuration, blurred disc borders, vascular tortuosity, hemorrhages, and Paton's lines are all possible clinical presentations (Figure 11).
11 “Patients frequently complain of blurred vision, transient vision loss, dizziness, tinnitus, and headaches.”
If papilledema is suspected clinically, a brain MRI or CT scan is performed as a way to rule out other possibilities, such as an intracranial tumor.11 MR venogram or CT venogram is commonly done to rule out a dural venous sinus thrombosis.11 If a mass lesion has been ruled out, a lumbar puncture (LP) with opening CSF pressure measurement should be performed.11
If an MRI reveals no tumor, the opening pressure on LP is elevated, and all other causes of excessive intracranial pressure have been ruled out, the diagnosis is usually
idiopathic intracranial hypertension.
11 Urgent therapy is recommended to relieve intracranial pressure. If intracranial pressure is not controlled, subsequent optic nerve atrophy and visual field loss may result.
11Treatment options include weight loss, avoidance of triggering medicines (e.g., contraceptives, tetracycline antibiotics, and vitamin A derivatives), and managing underlying risk factors (e.g., obesity). Other treatments include oral acetazolamide and/or topimarate, as well as surgical management.11
The visual prognosis is generally favorable, with less than 25% of patients sustaining permanent vision loss. Nevertheless, persistent papilledema can cause progressive optic atrophy.11
Inflammation – optic neuritis
Figure 12 shows fundus photography of optic neuritis caused by retrobulbar inflammation of the optic nerve.
Figure 12
Multiple sclerosis (MS) and neuromyelitis optica (NMO) are examples of
demyelinating neurological conditions that can cause optic nerve inflammation.
12 These diseases often manifest in the second to fifth decades of life, with white females having the highest frequency.
12 NMO can also be caused by ocular or systemic infection.
12 Common clinical signs and symptoms are acute unilateral vision loss that lasts hours or days, discomfort and pain upon eye movement, afferent pupillary defect, and visual field defects. In many cases, the optic nerve inflammation is retrobulbar; thus, the funduscopic examination is normal (Figure 12).
12“A common catch phrase used when considering a diagnosis of retrobulbar optic neuritis is ‘The doctor sees nothing, the patient sees nothing.’”
New cases of optic nerve inflammation should be reviewed with an on-call neurologist or neuro-ophthalmologist immediately to establish the best course management and treatment.12 After the first incidence, 75% of patients recover to 20/40 or better, however, with each subsequent occurrence of NMO, additional visual deterioration is expected.12
Ischemic optic neuropathy
A reduction in blood flow to the ganglion cells of the optic nerve causes ischemic optic neuropathy (ION).
13 Arteritic ION (AION) is caused by giant cell arteritis (GCA), whereas
non-arteritic ION (NAION) can be caused by a number of vascular abnormalities.
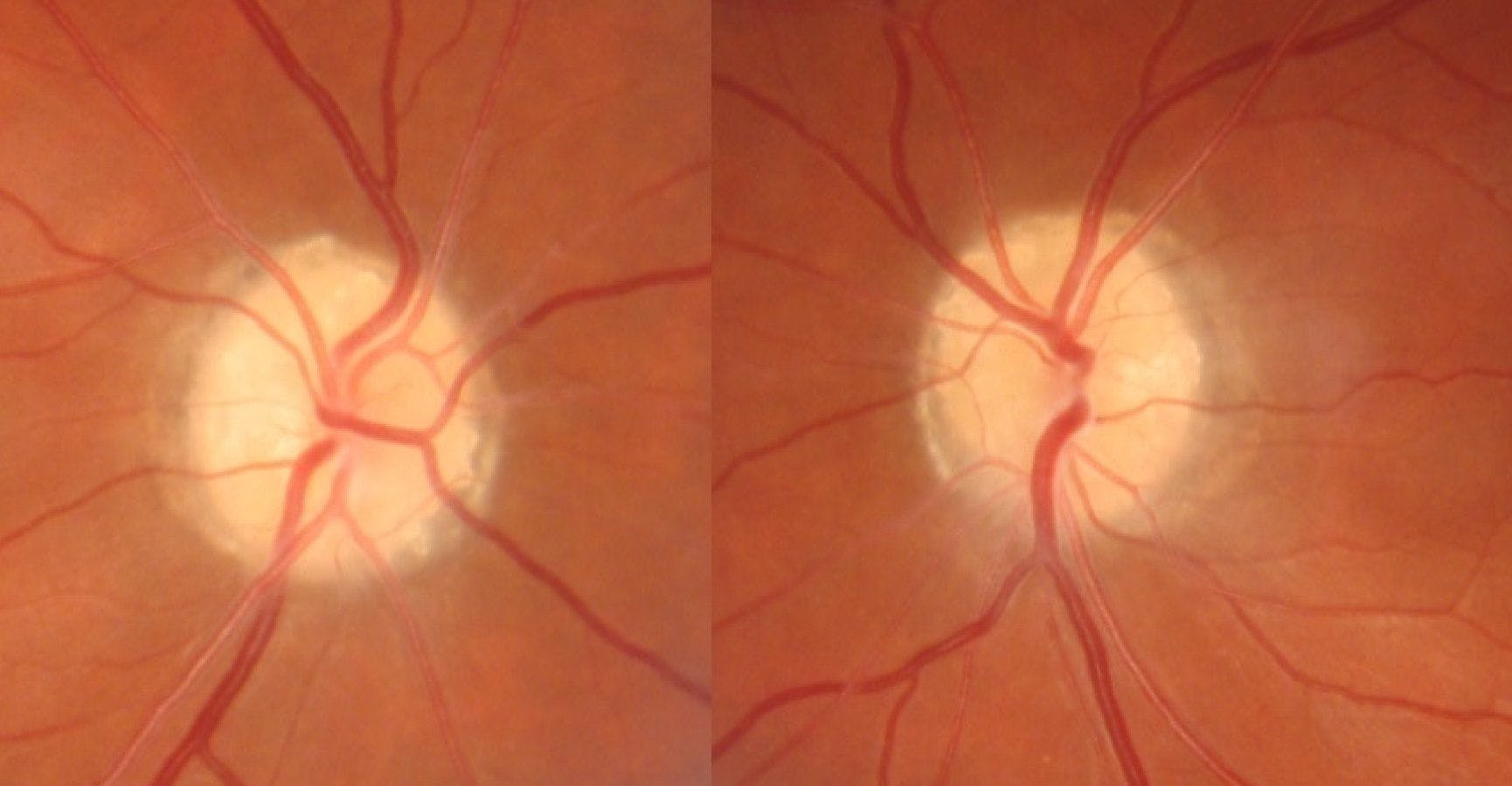
13Arteritic ischemic optic neuropathy
Figure 13 shows fundus photography of arteritic ischemic optic neuropathy.
Figure 13
Patients with AION are frequently above the age of 50, with symptoms including headache, scalp pain, fever, and malaise.
13 Ocular signs include abrupt unilateral vision loss with reduced visual acuity, which can be as low as 20/200, altitudinal visual field defects, an afferent pupillary defect, and
white pallor of the optic disc with diffuse edema (Figure 13).
13Furthermore, transient vision loss is an early symptom of AION, and if not treated promptly, the contralateral eye may develop visual loss 50% of the time.13
Management of AION is the same as management of
giant cell arteritis; urgent corticosteroid therapy is recommended.
13 Results of erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) tests, and complete blood count (CBC), as well as patient symptoms, are all used to guide the levels of steroids given.
13 Initially, high doses of steroids are given for 2 to 3 weeks, then tapered back over time; however, a lifelong low-dose regimen is usually needed to prevent blindness.
13Non-arteritic ischemic optic neuropathy
Figure 14 shows fundus photography of non-arteritic ischemic optic neuropathy.
Figure 14
Hypertension, diabetes, atherosclerosis, sleep apnea, nocturnal hypotension, small discs, and certain drugs are all risk factors for
non-arteritic ischemic optic neuropathy.
13 NAION patients frequently report painless, unilateral vision loss that lasts a few hours to several days, transient visual loss is uncommon in NAION.
13 NAION patients can have an afferent pupillary defect, sectoral or diffuse disc edema (Figure 14), and concomitant visual field loss upon testing.
13The disc swelling normally diminishes over a few weeks to months.13 There is currently no effective therapy for non-arteritic ischemic optic neuropathy.13 Comorbidities should be addressed and managed with the patient’s primary care provider.
In general, younger individuals have a better prognosis for visual recovery, and vision in the afflicted eye usually stabilizes within 2 months.13 Also, there should be a prompt re-evaluation of a NAION diagnosis if there is recurrence more than 2 months after the initial presentation.13
In conclusion
Optic nerve abnormalities frequently have distinguishing characteristics; however, they can also present similarly to other ocular conditions as well. It is critical to distinguish between benign and pathologic ocular disease since various instances may necessitate extended follow-up, STAT treatment, and/or surgical intervention.
A thorough understanding of the pathophysiology and clinical manifestations of optic disc abnormalities will result in
expert quality patient care, appropriate treatment, and avoiding vision-threatening complications.