


Some of what we do in optometry can be described as an art more than science, and a well-fitting scleral lens can be compared to a beautiful art piece.
It can be a beautiful thing to see, but a lot of hard work went into its creation, design, and iterations to get it to that point. That being said, nothing lasts forever, and whether it is a brand-new fit or modifying what was once a masterpiece, any lens is susceptible to some common fitting issues.
This article looks to address some of the most likely problems a fitter can encounter when managing scleral contact lenses and how to overcome them to reach your Mona Lisa.
Vital vocabulary
Throughout this article, we’ll reference a few key phrases or parameters as they relate to scleral lenses. If you’re new to fitting or if it’s just been a while since you’ve heard them, here is a brief overview of just a couple of them.
- The sagittal height, or sag, of a scleral lens is the distance measured from the back surface of a lens’ apex to the edge-to-edge chord.
- The vault or clearance of a lens is the distance from the back surface of the lens to the anterior surface of the cornea. Typically, this is referenced at the lens’ apex, limbally, and also over key corneal areas (such as over INTACS, graft junctions, etc.)
- A lens’ landing zone is the area where the edges of the lens contour on the sclera.
Clearance complications
One of the key features of a scleral lens is the fact that it vaults the cornea without contact, allowing us to, in a sense, recreate a smooth anterior surface of someone’s eye. This function is made possible in part by the lens’ sagittal height. The clearance of a lens is at its highest immediately after insertion, and as the lens remains on the eye, it begins to settle further back and nestles into its place.
The majority of settling takes place over the first couple of hours that a lens is on. For this reason, many practitioners like a lens to be worn into an assessment to more accurately gauge its fit, though further settling can occur well beyond this timeline.1
“A lens’ clearance from the cornea is one of the most important factors in optimizing the oxygen transmission of a scleral lens system.”
There are multiple fitting philosophies when it comes to scleral lenses, so there are no hard-and-fast rules as to the vault a lens needs to have over the cornea. Generally, a central clearance of about 100 to 200 microns is acceptable post-settling, but there can be reasons to increase or decrease this amount, as well. Issues with clearance can manifest in a number of ways.
If there is too much clearance, the lens may decenter inferiorly as the force of gravity pulls it downward. Epithelial swelling or damage can occur if the clearance is in need of adjusting as well.2 When a lens has less clearance, more oxygen transmission may be able to occur, but you also run the risk of not providing adequate hydration via the fluid reservoir.3
Figure 1 is an anterior segment optical coherence tomography (AS-OCT) of a scleral lens with a very low corneal vault (34μm).

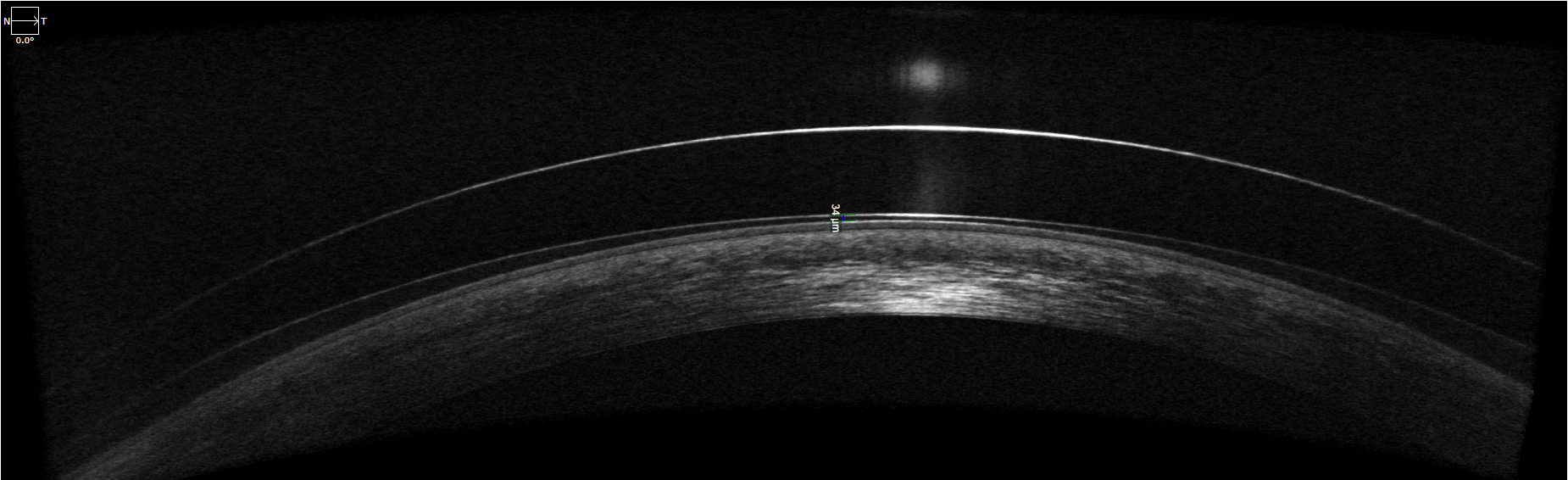
Figure 1: Courtesy of Alex Tharman, OD.
Figure 2 is an AS-OCT demonstrating a scleral lens with good centration and adequate central corneal clearance (226μm).

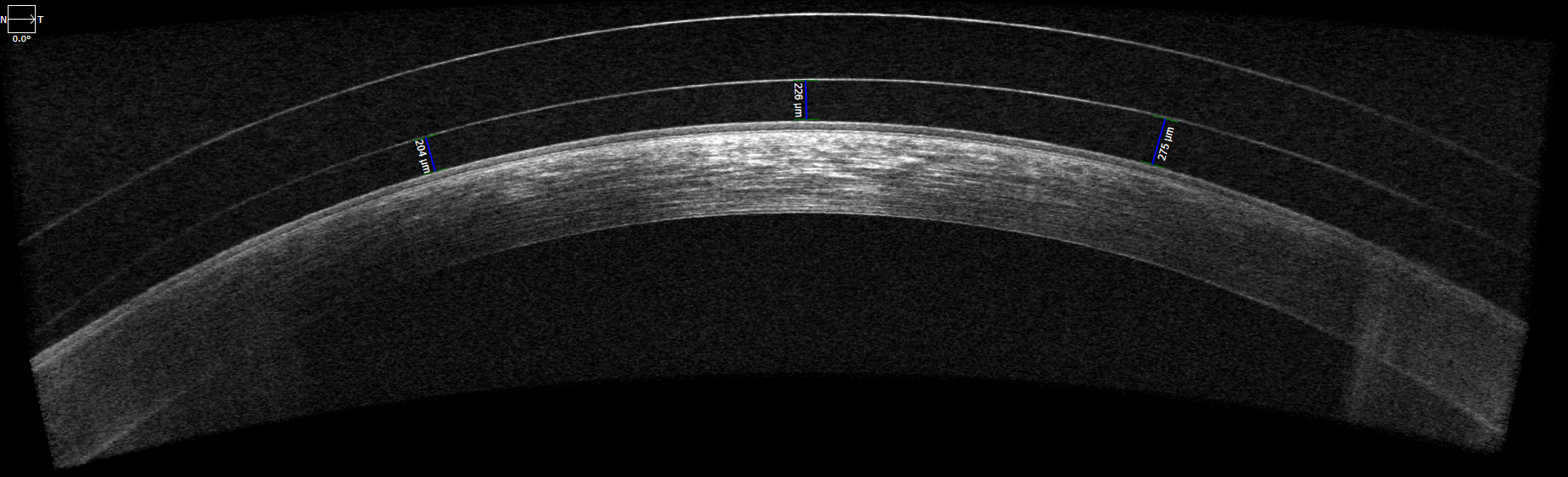
Figure 2: Courtesy of Alex Tharman, OD.
Problem-solving scleral lens clearance issues
Adjusting the clearance of a lens can be as simple as increasing or decreasing the sag parameter, but some cases may call for more specific refinements. For example, if the limbus is demonstrating excessive clearance but the lens looks good centrally, consider focusing on altering the limbal or transition zone.
Likewise, clearing INTACS rings that lie in the midperiphery can be aided by using an oblate-shaped lens design or even looking at the base curve of the lens and flattening it to fit this portion of the eye better.4
It’s worth noting that when altering the parameters of a lens, you don’t want to get too deep into the weeds until it’s necessary. Also, in some cases, it can be wise to minimize the changes you make from lens to lens so you’re not biting off too much in an edit or unintentionally counteracting one change with another.
Edge enigmas
The edges of a lens are arguably one of the most important factors in the overall success of a fitting. Since a scleral lens vaults the cornea, the weight of the lens should be equally distributed across the sclera at the landing zone 360°.
A lens with a poorly aligned landing zone can be plagued by fogging, redness, or pain with wear or following lens removal, difficulty with removal, air bubbles, and, as we’ll discuss later, can cause vision complaints.
As technology has evolved, our understanding of the ocular system and the way that scleral lenses are fit has also greatly advanced. Multiple studies have been performed to consider the curvature and shape of the sclera, and the vast conclusion has shown that the temporal scleral shape is much steeper than nasally, with the superior and inferior curvature being somewhat similar.5
Figure 3 demonstrates comparisons of edge fits and alignments of scleral lenses.

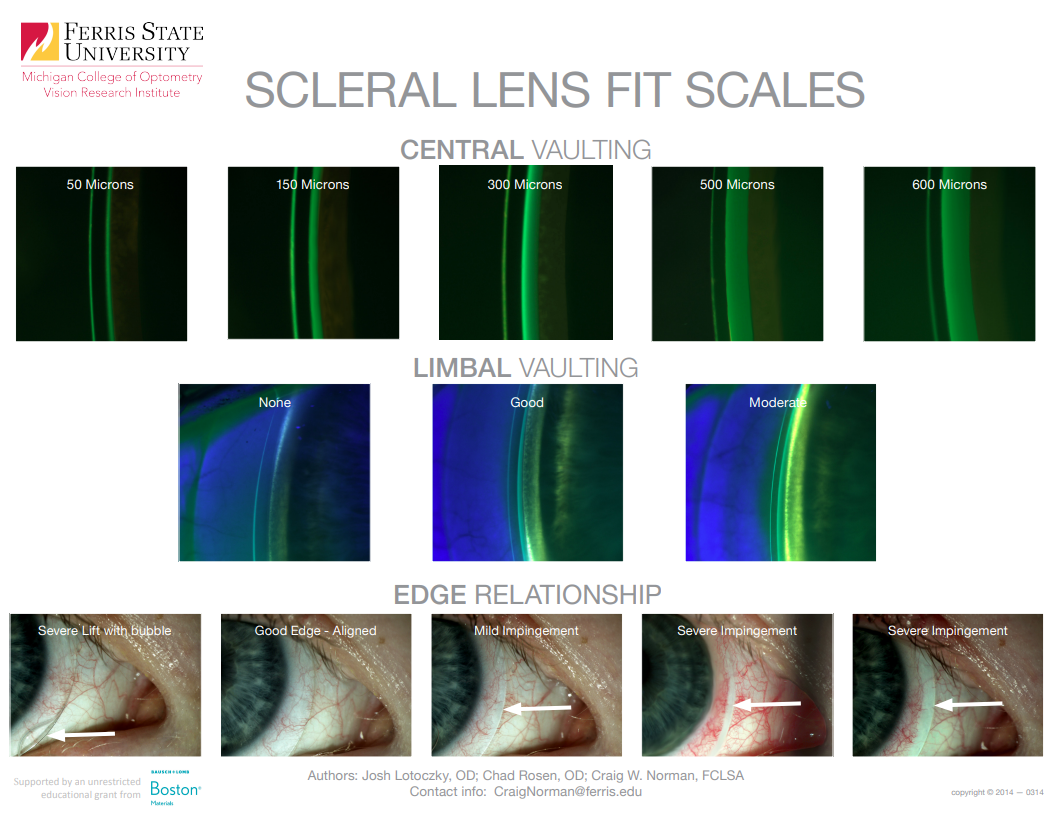
Figure 3: Courtesy of the Gas Permeable Lens Institute (GPLI) and Ferris State University.
Managing decentration and edge problems
Because of this data, we’re able to understand the decentration temporally that can be seen clinically when fitting lenses. It also means that toric peripheral haptics in lens designs have become more prevalent over the past number of years to better align to the flat and steep meridians of the wearer’s sclera.
Newer fitting technology also allows practitioners to utilize more specific designs to more accurately fit the sclera using quadrant-specific lens designs or sclera topography/mapping or impression-based molds to measure the peripheral shape of the eye.
Beyond the issue of decentered optics, edges of a lens that are too flat can lead to midday fogging of the layer of fluid between the eye and the contact lens as tear film debris, proteins, and other components can slip under the lens too quickly or easily.
Conversely, if edges land too steeply or the lens rides too tight for a patient, their eye can become irritated, the lens may be difficult to remove, or they may experience rebound hyperemia following lens removal.
Flat edges can be simple to discern if there is obvious liftoff similar to the depictions in Figure 3 above, but flat edges of a lens can also demonstrate blanching, so it is important to observe the vessels to discern how the edges of the lens are aligned.
Tight or steep edges will result in blanching at the edge of the lens, while blanching from a flat landing zone will be more interior, and there will be another border of vessels underlying the edge of the lens.6
Prescription problems
Unlike lenses of other designs, the prescription of a scleral lens may not be remotely close to the prescription that was measured during the initial refraction or even from the beginning of the fit to the final stages. This is because so many factors of a scleral’s design affect one another. In these systems, remember, the eye has a power, the lens has a power, but the tear layer created by the lens’ shape also has a power.
Changes to a scleral prescription, of course, are influenced by patient needs. But, how these are incorporated can depend on a fitter’s comfort and level of experience. For example, some fitters find the best practice is to push spherical equivalent prior to adding astigmatic correction to the design, or likewise provide the best distance correction before considering multifocal options.
Occasionally, if a patient is demonstrating an abnormal sphero-cylindrical over-refraction, a topography performed over the scleral lens can be a helpful tool to detect if lens flexure is present. Typically, if this scan reveals ≥0.50D of toricity, flexure of the scleral is occurring and needs to be addressed.
Optimizing the scleral lens fit
Since the primary cause for flexure is known to be haptic misalignment, optimizing the lens’ fit or increasing the center thickness of the lens can improve this. Some labs have a specific feature or parameter of their lens that can be adjusted to counteract flexure as well.
As with any fit, centration of the lens is of utmost importance to provide the best quality of vision possible. It may be worth revisiting the lens’ fitting relationship to the eye if a prescription seems hard to pin down. Of course, the more complex a prescription or design becomes, the more important this is.
With advanced lens technology, we’re more capable than ever in controlling scleral lens design. Systems are able to decenter optics to land over a patient’s visual axis, and multifocal zones can be specifically based on pupil sizes. With these adjustments and complex designs, vision improvement and quality can be impressive.
Fogging frustrations
As you can imagine, issues with fogging can be quite a nuisance for a patient as it may require removing their lenses throughout the day, multiple follow-up visits to address, and/or adding extra solutions to their toolkits such as a preservative-free, highly viscous solution (ex. Refresh Celluvisc).
As discussed earlier, the edges of a lens can play a huge role when it comes to posterior lens fogging. A flat area may allow protein and debris to flow under the lens and cause a buildup under the lens body. It’s also possible to have visual fogging occur if oxygen transmissibility isn’t appropriate and corneal changes are occurring during wear. Vital dyes can be very helpful to incorporate when trying to closely assess these portions of a lens fit.
“It’s also worth considering ocular surface disease or lens dryness in these instances, as those symptoms can closely mimic fogging.”
Perhaps they are experiencing ocular allergies and need to onboard a topical medication. Maybe their ocular surface or lid disease is in need of improved management, or perhaps they’re in a flare-up episode. Ensuring a proper lens care routine is in place, and the recommended solutions are used is another part of the puzzle that should be considered when dealing with persistent fogging.
In any case, there are a variety of issues that could be contributing to issues with midday fogging, and there are nearly countless aspects of a lens fitting to consider when attempting to improve it.7 Understanding the root cause of the issue is important as their management strategies would be very different.
Since fogging can be so prevalent, patients can be driven online in search of suggestions for improvement. As their providers, it is important that we give them accurate information and the best recommendations to optimize their outcomes.
Dryness difficulties
As with some of our previous points on addressing common scleral lens fittings, dryness difficulties are plentiful and have a number of routes to improving them. Thankfully, there are also a number of plans we can have going into a fit to set us and the patient up for success.
First of all, selecting a lens material that balances patient's needs of oxygen transmission, UV protection, and wetting angles sets up the base of the lens to have a good foundation for fighting dryness. Also, addressing ocular surface disease prior to fitting a lens can improve their lids and tear chemistry in advance and get ahead of issues this may cause.
You can also use a Hydra-PEG coating on the lenses to improve their wettability, and this layer can be a true investment for patients worth protecting using the proper solutions and treatments like Tangible Boost. Similar to addressing dryness for any other patient, its treatment plan can be multifactorial and should, of course, be compliant with their lens wear.
Conclusions
Though this article looks to address and discuss some of the most prevalent issues that can arise during the fitting process of a scleral lens, some of these can be quite intricate and require a careful history to fully understand how to best handle each case.
Thankfully, we’re lucky to have such numerous and quality resources at our fingertips that we can look to help us navigate this territory and work towards a solution for patients experiencing these issues.


