


Chorioretinal folds (CRFs) are visible striations due to undulations in the choroid, Bruch’s membrane, the retinal pigment epithelium (RPE), and the overlying retina.1 CRFs can be asymptomatic and identified on either a routine eye exam or while evaluating another retinal condition.
More rarely, CRFs with complications can lead to symptoms of metamorphopsia, visual disturbances, or photopsia, which would prompt a patient to seek evaluation.1
The condition can be idiopathic, a result of the anatomy of a hyperopic eye, or associated with ophthalmic or systemic disease. Therefore, the presence of CRFs warrants a careful workup to rule out the more ominous causes.
Diagnosis of chorioretinal folds
CRFs can be detected on dilated fundus exam and with the use of multimodal imaging techniques. The folds appear as yellowish striations that can be oriented in horizontal, vertical, radial, or oblique patterns.1 On fluorescein angiography (FA) and fundus autofluorescence (FAF), they appear as alternating striations of hyper and hypofluorescence. On FA, the striations present in the early phase and persist.1,2
On optical coherence tomography (OCT), there is signal reduction of the choriocapillaris in the area of the folds and apparent undulations of all of the involved retinal layers.2,3 OCT angiography (OCTA) can demonstrate a decrease in perfusion to the choriocapillaris in the areas associated with the folds.2 Indocyanine green angiography (ICGA) in these cases shows delayed choroidal filling, patchy hypofluorescence, and dilation of choroidal veins.1
Differential diagnoses for chorioretinal folds
CRFs can present either as unilateral or bilateral findings, with the incidence of each being about equal, but mostly depending on the underlying cause.
The most common causes for unilateral presentation are trauma and ocular tumors, while the most common causes for bilateral cases are thyroid eye disease, uveitis, and choroiditis. Age-related macular degeneration (AMD), scleritis, hypotony, and hyperopia can cause unilateral or bilateral CRFs.1
Hyperopia and neovascularization
Hyperopia, primary or acquired, is identified as the cause of CRFs in up to a quarter of cases. Primary hyperopia-related CRFs would present without symptoms, while acquired would present with painless visual loss or visual distortions.2 Primary hyperopia-related CRFs usually appear as bilateral, symmetric, and mostly limited to the posterior pole.4 This was consistent with the findings in the case report.
Pathology causing neovascularization at the macula can also lead to CRFs. The proposed mechanism is a contraction of a fibrovascular membrane that causes a pucker in the underlying choroid.1 CRFs can lead to secondary maculopathy, termed CRF-maculopathy, which involves RPE atrophy and hyperplasia and is often difficult to differentiate from non-exudative AMD without the associated factor of the folds themselves.2
Scleritis
If scleritis is the underlying cause of chorioretinal folds, this is usually accompanied by a painful eye with or without a headache, conjunctival hyperemia, and chemosis with thickened and inflamed sclera.1
If scleritis is identified, the patient should be worked up with an autoimmune panel since there is a strong association with conditions like systemic lupus erythematosus, rheumatoid arthritis, polymyalgia rheumatica, and Wegener’s granulomatosis.1,3
Hypotony
Hypotony, a state where the intraocular pressure is under 5mmHg, can either be asymptomatic or cause changes to vision. Hypotony can be secondary to intraocular surgery (i.e., glaucoma filtration procedures and retinal or corneal procedures), ciliochoroidal detachment, or iridocyclitis.
In hypotony cases, the CRF striations are arranged irregularly in a non-uniform pattern and may be accompanied by engorged and tortuous retinal vessels.4
Intracranial pressure
Intracranial hypertension, idiopathic intracranial hypertension (IIH), and empty sella syndrome causing increased intracranial pressure can also cause CRFs, sometimes even in the absence of papilledema.1,5 CRFs from papilledema usually appear circumferentially around the optic disc with some horizontal striations at the macula. The patient with papilledema would typically report symptoms of nausea, headache, and transient visual obscurations.4
Compression of the orbit by a retrobulbar or intraocular tumor can lead to eventual CRFs. In such cases, the striations are often arranged circumferentially around the tumor base. Central serous chorioretinopathy (CSCR), uveal effusion syndrome, and nanophthalmos can also cause CRFs. Another rare cause is space-flight-associated neuro-ocular syndrome. Roughly 15% of cases of CRFs were identified as idiopathic after thorough evaluation.1,3,4
Management of chorioretinal folds
The management of CRFs usually entails treating the causative condition, and therefore, a workup to evaluate for the above differential diagnoses is necessary. Imaging such as OCT, OCTA, FA, FAF, and ICGA play a major role in detecting underlying or related conditions like CSCR, AMD, or pathology of the optic disc for example.
Blood pressure, neuroimaging, and possibly lumbar puncture are indicated if papilledema or IIH are suspected. B-scan ultrasonography does not detect CRFs but can evaluate for tumors (along with neuroimaging) and posterior scleritis.
Thyroid function testing and an autoimmune workup are also warranted. Lastly, remember relevant case history questions that can be correlated to CRFs, such as the patient’s refractive error or history of ocular surgery or trauma.4
Choroidal folds case report
This report involves a patient who presented for a diabetic eye exam and was found to have RPE abnormalities and choroidal folds in addition to mild non-proliferative retinopathy.
It will review the clinical appearance, multimodal imaging results, differentials, and management of CRFs.
Patient history
A 75-year-old Caucasian male presented for a diabetic eye exam. His ocular history included early dry AMD and visually insignificant cataracts at his eye exam 1 year ago. He had no history of diabetic retinopathy, and his family ocular history was unremarkable. He denied any new visual or ocular complaints at the present exam.
He reported having type 2 diabetes for 35 years and that he was compliant with his treatment and care plan. The patient was taking metformin with a last A1c of 8.0, tested 1 month ago. He also had a medical history of borderline hypertension and chronic kidney disease. The patient did not have a history of smoking, alcohol abuse, or any illicit drug use.
Exam findings
Entering corrected visual acuity was 20/20 OD and 20/20 OS. His spectacle prescription was +3.25-0.75x90 OD and +2.75-0.50x80 OS. Extraocular motilities and confrontation visual fields were full in each eye. Pupils were equal, round, and reactive without afferent pupillary defect. Amsler grid was without distortion or scotoma in either eye.
A slit lamp exam of the anterior segment revealed mild anterior blepharitis and pinguecula nasal and temporal in each eye. The cornea was clear, anterior chamber deep and quiet, and the iris flat and intact without neovascularization in each eye. Intraocular pressure via applanation was 14mmHg in each eye at 1:24pm. The patient had grade 1 nuclear sclerotic and grade 1 anterior cortical cataracts in each eye.
On dilated fundus exam, a small C:D ratio of 0.25 was observed in each eye, with both optic nerves appearing healthy and with distinct borders. Both maculas had RPE changes with pigment migration. There was no sign of diabetic retinopathy OD but one single parafoveal dot hemorrhage was present OS.
In both eyes, yellow striations were present that ran in an oblique pattern throughout the posterior pole in the area of the arcades. There was also an irregular area of atrophy superior to the optic nerve in the left eye.
Multimodal imaging of the patient
Optos images in color and with FAF were obtained to document the folds along with foveal RPE metaplasia and the dot heme OS.
Figure 1 highlights Optos color fundus photos OD (left image) and OS (right image).


Figure 1: Courtesy of Danielle Kalberer, OD, FAAO.
Figure 2 demonstrates FAF Optos photos OD (left image) and OS (right image).


Figure 2: Courtesy of Danielle Kalberer, OD, FAAO.
As seen in Figures 3 and 4, OCT imaging revealed a small area of intraretinal fluid nasal to the fovea OD and more prominent non-central intraretinal fluid OS.
Figure 3 shows OCT imaging of the patient's macula OD.

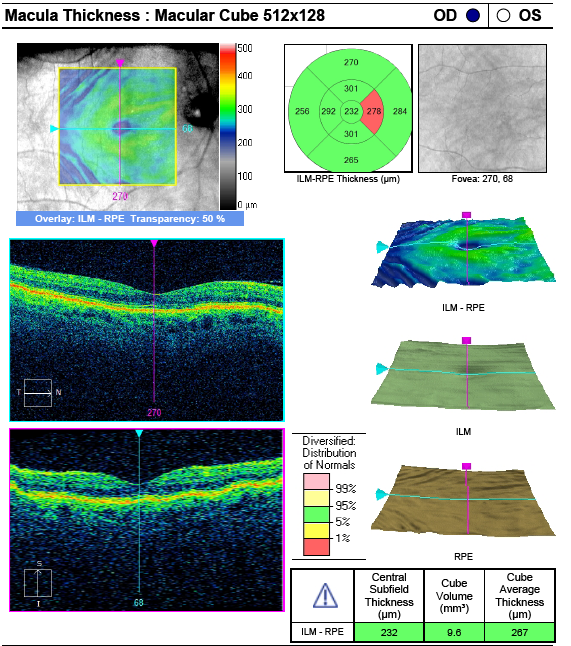
Figure 3: Courtesy of Danielle Kalberer, OD, FAAO.
Figure 4 features OCT imaging of the patient's macula OS.

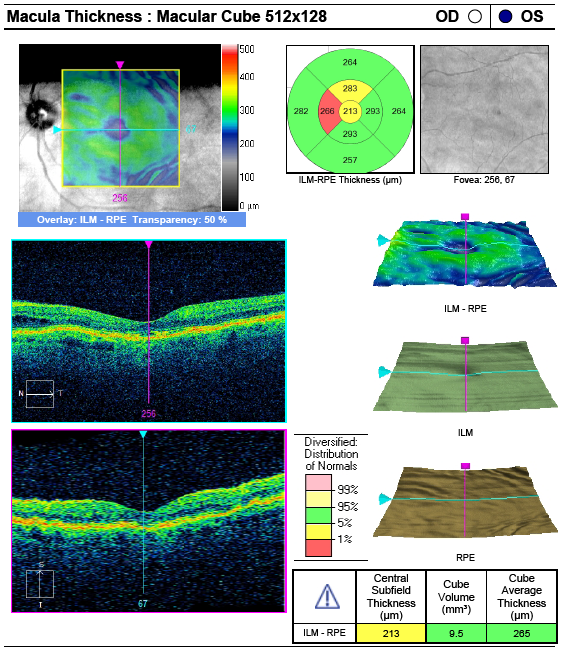
Figure 4: Courtesy of Danielle Kalberer, OD, FAAO.
Visible undulations were present in the layer of the RPE and overlying retina outside the fovea. Based on the clinical fundus exam and imaging results, the patient was diagnosed with CRFs and mild non-proliferative diabetic retinopathy (NPDR) in the left eye.
A fluorescein angiogram was performed 2 weeks later. The test showed diffuse, bilateral CRFs with areas of late intraretinal leakage away from the fovea more OS than OD. There was also evidence of mild NPDR OU (initially subclinical OD with more signs than detected funduscopically OS revealed on the angiogram), as seen in Figure 5.
Figure 5 is FA Optos photos, mid-phase OD (left image) and OS (right image).

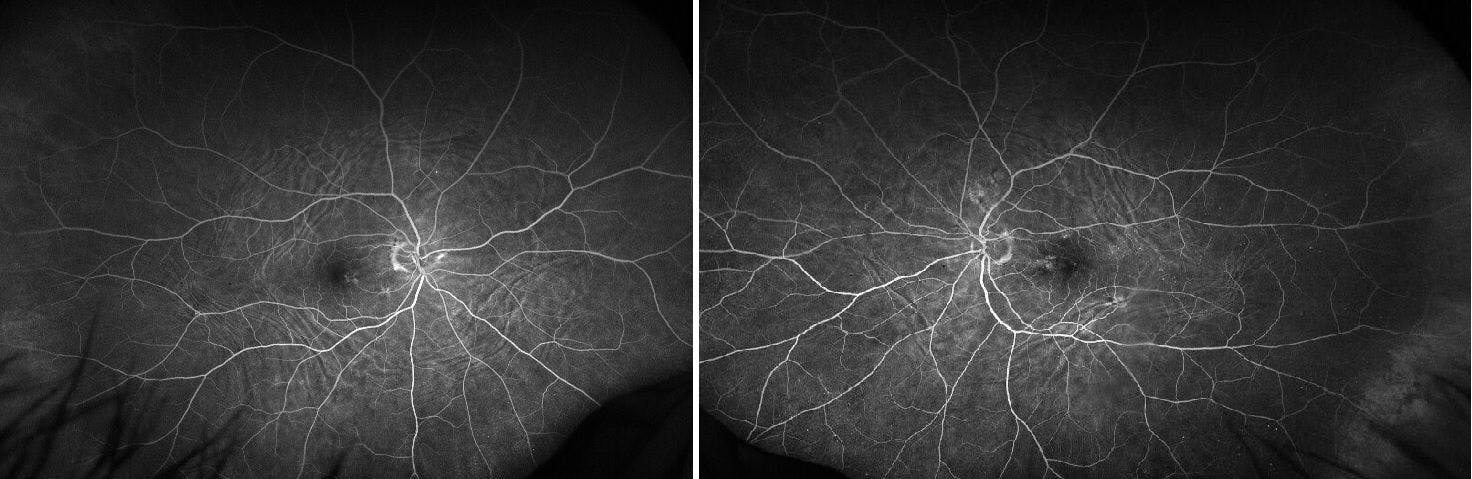
Figure 5: Courtesy of Danielle Kalberer, OD, FAAO.
Management
Since the patient had excellent visual acuity and was not symptomatic, he was asked to return for follow-up in the retina clinic in 2 months to monitor closely. Though the non-symptomatic nature of the condition, along with its bilateral and symmetric appearance and the patient’s hyperopic refractive error, were all suggestive of a non-pathologic cause of the CRFs, the patient was still referred for magnetic resonance imaging (MRI) of the brain and orbit without contrast.
This was recommended to rule out compressive pathology or empty sella syndrome because he had a history of renal impairment related to diabetes. The importance of maintaining compliance with his diabetes treatment plan was also discussed, along with potential sight-threatening ocular sequelae of diabetes.
Additionally, AMD risk factors were reviewed, though, at this time, it is unknown if the maculopathy observed was secondary to the retinal pathology, true AMD, or a multifactored condition. The patient was asked to perform daily Amsler grid monitoring at home and to return promptly if any changes were noticed.
Conclusion
Chorioretinal folds are a rare retinal condition. The condition ranges in severity from associations with benign conditions like primary hyperopia or idiopathic nature to more severe associations with retrobulbar tumor or systemic disease.
With clinical examination and imaging, providers can detect CRFs and recommend the appropriate workup and management for their patients.


