


Iridotomy is a long-standing therapy used in the treatment of pupillary block and acute angle-closure glaucoma. The first reported surgical treatment for glaucoma was a surgical iridectomy performed through a corneal wound in 1857 by Albrecht von Graefe.1
As technology continued to progress, argon laser iridotomy began to be used in the mid-1970s as a less invasive treatment.
This was associated with high iridotomy closure rates and other complications; thus, in the 1980s, neodymium-doped yttrium aluminum garnet (Nd:YAG) laser began to be used as it required less energy and had a lower risk of closure and other complications.2
Overview of iridotomy for glaucoma
In a normal eye, aqueous fluid created by the ciliary processes passes from the posterior chamber into the anterior chamber by traveling around the pupillary margin. However, in cases of pupillary block (angle closure), fluid is unable to use this passage and builds up behind the iris, which pushes the iris forward and obstructs the trabecular meshwork.
A peripheral iridotomy entails creating a peripheral ostomy in the iris to allow aqueous to pass from the posterior chamber into the anterior chamber in cases of pupillary block.3
Through retroillumination, Figure 1 shows laser peripheral iridotomy of the left eye at 10 o’clock.

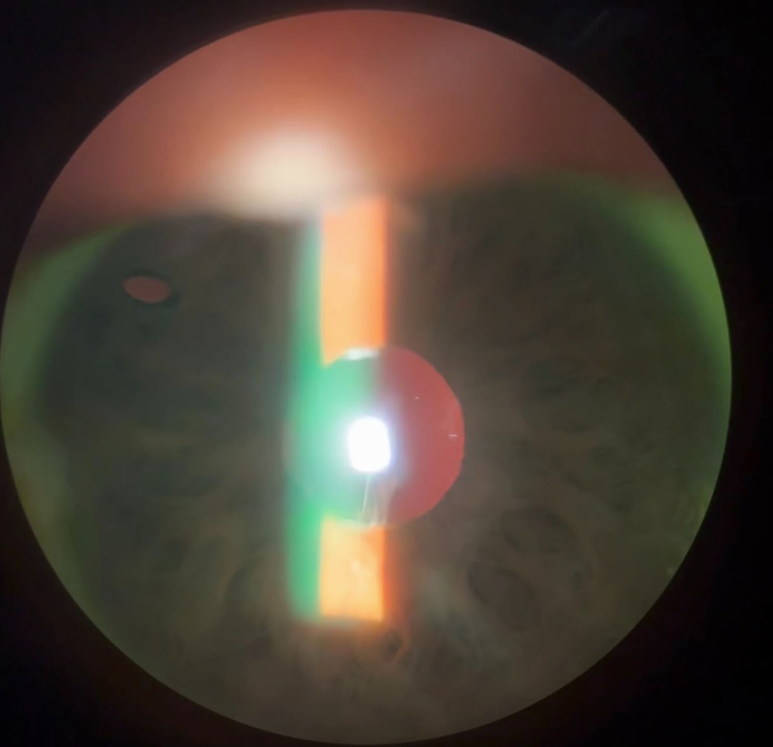
Figure 1: Courtesy of Alanna James, MD.
When should iridotomy be used?
Iridotomy is useful in cases of acute pupillary block (acute angle-closure glaucoma) and is used as prophylaxis in patients who may be predisposed to pupillary block (i.e., narrow-angle patients). Acute primary-angle closure is a common indication in which iridotomy is used, along with iris bombe.
This procedure is also thought to be helpful in preventing acute angle-closure attacks in patients with primary angle-closure suspect (narrow angle), primary angle closure, and primary angle-closure glaucoma. It is also used as a diagnostic agent to rule out pupillary block as an etiology of angle closure in patients with plateau iris or aqueous misdirection.4
Surgical iridectomy, which is a similar procedure but done in the operating room without laser, is often used in procedures such as silicone oil placement and Descemet’s membrane endothelial keratoplasty (DMEK) as prophylaxis, as the oil and air used in each, respectively, can lead to pupillary block.
Zhongshan Angle Closure Prevention study
In 2019, He et al. published the Zhongshan Angle Closure Prevention (ZAP) trial, which looked at the rates of progression from primary angle-closure suspects (PACS) to primary angle closure (PAC) with a more recent 14-year follow-up published in August 2023.5,6
Of note, PACS was defined as two or more quadrants without visible trabecular meshwork, no peripheral anterior synechiae (PAS), baseline intraocular pressure (IOP) less than or equal to 21mmHg, and negative dark room prone-position test (DRPPT).
DRPPT is performed by placing the patient in a prone position in a dark room for 15 minutes and comparing the pressure before and after. PAC was defined as IOP greater than or equal to 24mmHg, formation of one or more clock hours of PAS, or an episode of acute primary-angle closure (APAC).
Findings from the ZAP study
They enrolled 889 patients with bilateral PACS and performed laser peripheral iridotomy (LPI) in one eye while using the other eye as a control. Their data showed that five of the control eyes and one of the LPI eyes developed acute primary-angle closure, but this difference was not statistically significant.
The progression risk to PAC was 3-fold lower in the treated eyes compared to the controls; however, this was largely due to the lower risk of PAS formation, not the other criteria for PAC.
More notably, the progression risk of 1.4% per eye-year was very low in the control eyes, although higher than in the primary 6-year data (0.8% per eye-year). The number needed to treat to prevent one case of PAC was 12.4, and only two LPI and four control eyes developed primary angle-closure glaucoma (PACG).
Previously, many providers were performing laser peripheral iridotomy on all patients found to have narrow angles on gonioscopy. The ZAP trial showed that observation was a viable option for many patients with narrow angles.
Weighing the risks and benefits of iridotomy
Although not thought of as a very risky procedure, iridotomy can have complications. There is a risk of inflammation, hyphema, laser energy hitting the natural lens or cornea, and post-operative dysphotopsias.
Further, the ZAP trial noted the LPI eyes had increased IOP and formation of cataracts compared to the control eyes.4 Also, the procedure is not painless in many scenarios.
However, the vision loss that can occur in the setting of an acute angle-closure attack or primary angle-closure glaucoma can be devastating. Thus, it is important to identify patients who are at higher risk in order to determine good candidates for iridotomy.
Alternatives to iridotomy
The alternatives to iridotomy include observation, as discussed in the ZAP trial above, or lens extraction, which was discussed in the Effectiveness of Early Lens Extraction for the Treatment of Primary Angle-Closure Glaucoma (EAGLE) study.7
This study included patients 50 years or older without cataracts and with mild or moderate PACG or newly diagnosed PAC with IOP of 30mmHg or greater who were randomized to LPI or clear lens extraction.
The results showed that clear-lens extraction had greater efficacy and was more cost-effective than laser peripheral iridotomy.7
5 pearls for performing an iridotomy
1. Set patient expectations
I try to undersell and overdeliver. I always tell my patients that this is not a painless procedure and most times they tell me it was better than they expected. Discussing the risks pre-operatively is important as they may develop a hyphema, which can blur the vision afterward.
I also let them know before placing the pilocarpine that they can have a headache from the drops. It’s also important to let them know that they will have to wait after the laser procedure for a pressure check.
2. Use pre-operative drops
Pilocarpine is helpful to stretch the iris and make it thinner, which can make it easier for the laser to make the opening. Instillation of apraclonidine or brimonidine can help to prevent a post-operative IOP spike.
3. Find an iris crypt
There are thinner parts of the iris that are easier to create a hole through. Finding an iris crypt peripherally can reduce the amount of energy and shots needed to create a patent iridotomy.
4. Use an iridotomy lens
While the procedure can be performed without an iridotomy lens, I find the lens helpful to control the eye and it gives good magnification which is helpful for visualization.
5. Use a higher power
When I first started performing iridotomies, I was very timid with the laser power as I was worried this might cause more pain for the patient.
With time, I’ve found you need fewer shots if you start at a higher power which can lead to a shorter procedure time with less pain for the patient. I usually start around 6 to 8mJ now for my power.
In closing
In summary, laser peripheral iridotomy remains an excellent treatment to have in our toolbox for the treatment and prevention of pupillary block and it is important to be able to perform this procedure skillfully.
Recent studies show that we need further research to show which patients may actually benefit from prophylactic iridotomy.


