


Glaucoma surgery has dramatically transformed since the first successful trabeculectomy was performed in 1968.1 As we have learned more about the disease, the techniques we have used to treat it have continued to advance.
With the advent of each new surgery comes new complications and different techniques to help our patients obtain the best outcomes.
Comparing glaucoma surgery and MIGS procedures
An observational cohort study from 2020 indicated that 75.5% of the glaucoma surgeries being performed in the United States were minimally invasive glaucoma surgeries (MIGS), 11.4% were various forms of glaucoma drainage implants, and 13.1% were trabeculectomies.2
While this is a large shift from the distribution of incisional glaucoma surgeries performed many years ago, the decision of selecting the type of surgery for patients is still determined on an individualized basis.
One of the advantages of MIGS is a higher safety profile, but there remain many patients who still would benefit from tubes and trabeculectomies over MIGS. Thus, it is important to be aware of all of the complications of glaucoma surgeries and what we can do to reduce their occurrences.
Complication #1: Hypotony
Hypotony, or excessively low intraocular pressure (IOP), is not an infrequent concern following glaucoma surgery. We have a variety of ways to decrease pressure, but are very limited when it comes to remedies for hypotony.
While controlled lowering of IOP is the desired outcome of glaucoma surgery, hypotony can have serious vision-threatening consequences, including maculopathy, keratopathy, and choroidal effusions.3 Hypotony after glaucoma surgery can be due to overfiltration, wound or conjunctival leaks, ciliary body shutdown, and cyclodialysis clefts, among other reasons.4
It is important to ensure that once deemed hypotonous, the patient is no longer taking aqueous suppressants in that eye. The most crucial factor to consider when presented with a patient with low IOP post-operatively is to determine the mechanism, as that will guide the treatment. It is also important to rule out a bleb leak, cyclodialysis cleft, or excessive inflammation.
Overfiltration occurs when there is an excessive outflow of aqueous humor from the eye. In trabeculectomies, this can be secondary to a large ostium, poorly placed sutures or their failure to maintain the desired tension on the scleral flap, or aberrant wound healing.
For glaucoma drainage implants, overfiltration can be secondary to a faulty valve mechanism in valved devices or insufficient ligation of the tube for non-valved devices.
Managing hypotony
A good surgical technique can prevent many of these issues, but in some cases, complications still occur. Hypotony has been shown to have a lower incidence in MIGS procedures—but can still occur—although it is more common with Xen gel stents and traditional incisional glaucoma surgery.
How do we treat it? You can try the placement of a large-diameter bandage contact lens, which is thought to create some resistance in the bleb and slow down filtration.
In some cases, treatment may require reoperation to completely replace a glaucoma drainage device in the case of a faulty valve system or to ligate the tube. For trabeculectomies, you can consider transconjunctival compression sutures of the flap (if the flap is visible), revision of the bleb, or resuturing of the flap.5
If you are planning to resuture the flap, you may need to place a scleral patch graft, as the sclera can be very friable after mitomycin C application.
Complication #2: Choroidal effusions
Choroidal effusions, or serous choroidal detachments, often go hand in hand with hypotony. Treatment typically consists of cycloplegic agents and topical corticosteroids (and, in more severe cases, systemic corticosteroids). Cycloplegics are thought to relax the ciliary muscle and reduce fluid accumulation.
Oftentimes, the choroidal effusions resolve spontaneously as the IOP stabilizes; however, if conservative treatment is not sufficient, surgical intervention may be necessary, such as choroidal drainage.6 Choroidal effusions are typically drained inferiorly by creating a peritomy 5 to 6mm posterior to the limbus and creating a radial scleral incision that reaches the suprachoroidal space.
This will become apparent by the release of straw-colored fluid. The sclerotomy is left open to continuously drain, but the conjunctiva and Tenon’s layers are closed.
Figure 1 shows B-scan imaging demonstrating a small choroidal effusion.


Figure 1: Courtesy of Alanna James, MD.
Figure 2 highlights B-scan imaging showing a large choroidal effusion.

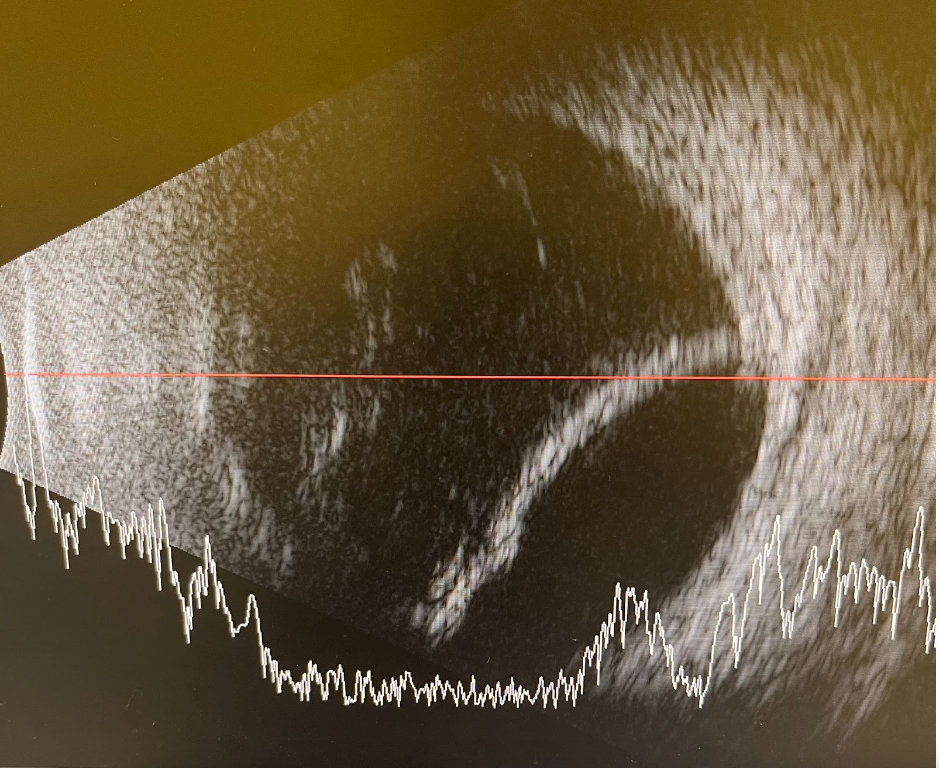
Figure 2: Courtesy of Alanna James, MD.
Complication #3: Aqueous misdirection (malignant glaucoma)
The exact mechanism of aqueous misdirection is still not well understood, although there are many theories. It is thought to be related to aqueous fluid traveling posteriorly into the vitreous cavity, causing uniform shallowing of the anterior chamber and increased IOP.
This could initially be caused by sudden shallowing of the anterior chamber with conjunctival leaks or overfiltration after suture removal, but is especially common after trabeculectomy in cases of chronic angle closure glaucoma. Initial treatment involves aqueous suppressants and cycloplegics; however, if conservative management fails, surgical intervention is required.7
The Nd:YAG laser can be used in aphakic or pseudophakic eyes to attempt to disrupt the anterior hyaloid, but occasionally, incisional procedures may be required. Previously, needle aspiration of the vitreous has been done, but pars plana vitrectomy with disruption of the anterior hyaloid face is more commonly performed.
Careful monitoring is important for these patients as there is the possibility of relapse. The patient may need long-term cycloplegic eye drops, and the fellow eye carries the risk of the development of aqueous misdirection post-operatively.
Complication #4: Suprachoroidal hemorrhage
Suprachoroidal hemorrhage is a rare but terrifying complication of glaucoma surgery. Risk factors include anticoagulant or antiplatelet use, uncontrolled hypertension, atherosclerosis, glaucoma with high IOP for a long duration, advanced age, and hypotony during surgery.8
The risk is very high in patients with high episcleral venous pressure, such as cavernous sinus-carotid fistulas or Sturge-Weber syndrome. The use of hyperosmotic agents or releasing aqueous gradually through a paracentesis has been discussed as methods of prevention.
For trabeculectomies, pre-placing scleral flap sutures can lead to a quicker closure of the scleral flap and a shorter duration of hypotony. Further, for very high-risk eyes, preventive sclerotomies should be placed.
Signs of a suprachoroidal hemorrhage intra-operatively include:
- Shallowing of the anterior chamber
- Loss of the red reflex with the appearance of a dark posterior segment mass
- Pain
Managing suprachoroidal hemorrhage
The scleral flap should be closed immediately, and intravenous mannitol can be given to reduce the IOP. Sclerotomies may be needed in certain cases to promote drainage. Additionally, suprachoroidal hemorrhage can also occur after surgery.
Patients will typically present with abrupt onset pain, nausea, and decreased vision. The exam is notable for a uniformly flat anterior chamber, loss of the red reflex, and appearance of dark brown dome-shaped choroidal elevations. B-scan imaging shows blood in the suprachoroidal space.
Smaller hemorrhages can resolve spontaneously with topical and systemic steroids, but larger hemorrhages will require drainage. Drainage is usually not done immediately, as the blood clots and can prevent any drainage. However, blood is toxic to the retina, and the longer the blood sits, the more damage that can occur.
After liquefaction of the clots, which may occur 2 to 4 weeks after the initial bleed, drainage can be performed through an inferior sclerotomy, as mentioned above.9 Visual prognosis varies depending on the extent of the hemorrhage, with smaller localized hemorrhages outside of the macula portending a better prognosis.
Figure 3 features B-scan imaging of a suprachoroidal hemorrhage.

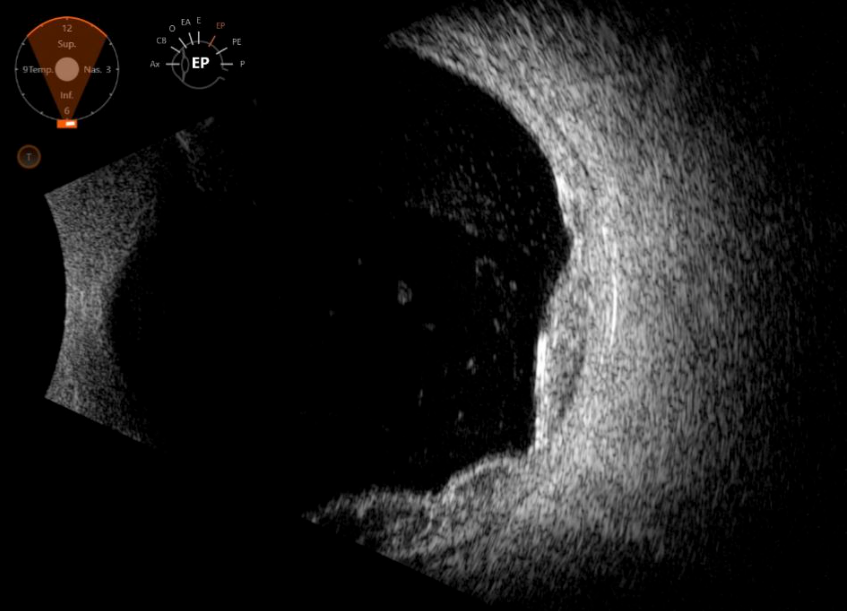
Figure 3: Courtesy of Alanna James, MD.
Final thoughts
In conclusion, there is a long list of complications that can occur with glaucoma surgery, many of which we did not even begin to cover in this article. A critical part of preventing complications involves pre-operative planning.
It is important to know what your patient’s eye could be at risk for in order to take steps to reduce the risk of complications. Additionally, it is crucial to discuss with patients the risks of glaucoma surgery pre-operatively, including decreased vision and the need for additional procedures.
If you do enough surgery, complications are inevitable. Being able to recognize and treat these complications is a critical part of the practice of the specialty of glaucoma.


