


Corneal dystrophies are a group of inherited genetic eye disorders.1-8 Here, abnormal material builds up in the cornea layers and is usually bilateral.1-3 Most corneal dystrophies are slowly progressive and run in families.1-3 This article and study guide will outline the more commonly encountered corneal dystrophies as well as important key facts.
In order to understand the various presence of corneal dystrophies, it is often important to break them down by corneal layer. From anterior-to-posterior (external to internal) the layers of the cornea are:
- epithelium
- Bowman’s membrane
- stroma
- Descemet’s membrane
- endothelium
These layers work together to help maintain the cornea’s transparency. Accumulation of abnormal substances in the corneal layers can disrupt corneal transparency and lead to varying degrees of blurred vision.1-3
For the complete list plus clinical photos, download the Corneal Dystrophies Study Guide!
📖
Download the Study Guide
Get the complete list of common corneal dystrophies with clinical photos for easy reference!
ANTERIOR CORNEAL DYSTROPHIES
Anterior corneal dystrophies affect the outermost layers of the cornea—the epithelium and Bowman’s membrane. Due to a disturbance in the anterior layers of the cornea, patients may experience recurrent erosions.1-3
Anterior basement membrane dystrophy
AKA: ABMD, Map-dot fingerprint corneal dystrophy, Cogan’s microcystic dystrophy, epithelial basement membrane dystrophy (EBMD)1-3
Inheritance: Autosomal dominant1-4,8
Exam findings: Slit lamp exam may show transparent microcysts, ‘fingerprint lines’, and gray dots in the corneal epithelium which can be subtle or very pronounced.1-6,9 Due to abnormal build-up of material under the epithelium, the corneal epithelium can become irregularly elevated. This can lead to reduced adherence of the epithelium to the underlying stroma, predisposing the patient to recurrent erosions as well as blurry vision.1-6,9
Demographics: Patients of all ages can be affected, with a range of presentation from 25 to 75 years.1,4,7,9 The onset can be spontaneous or may be triggered by traumatic injury to the cornea (fingernail scratch, paper cut, even LASIK surgery).1,4,7,9
Histology: Here, extra sheets of basement membrane are seen extending abnormally into the corneal epithelium (“maps”), while maturing epithelial cells migrating towards the anterior surface of the epithelium become entrapped in these extra sheets and form cysts (“dots”).6,7,9 In addition, concentric or parallel lines of thickened basement membrane may present as ‘fingerprints.’6,7,9
Meesmans dystrophy
AKA: Juvenile hereditary epithelial dystrophy, Meesmann-Wilke syndrome1-3
Inheritance: Autosomal dominant, KRT3 (locus 12q13.13) or KRT12 (locus 17q11-q1) responsible for encoding two cornea-specific cytokeratin units in the epithelium1-4,8
Exam findings: Slit lamp exam may show bilateral symmetric development of intraepithelial microcysts that lead to intense fragility of the corneal epithelium.1,4,7,9 Over time, these epithelial vesicles increase and involve the central visual axis and mid-peripheral cornea, but may extend to the limbus.1,4,7,9 Most patients remain asymptomatic with minimal visual disturbances, while some suffer from recurrent erosions.1,4,7,9
Demographics: Disease onset may begin in early childhood, but may not become noticeable until adulthood1-4
Histology: Histopathology here shows clusters of small, clear, intraepithelial cysts diffusely distributed at different levels within the corneal epithelium, which is irregular in thickness.4-7,9 The microcysts are found in basal epithelial cells and contain degenerated epithelial cells and cellular debris that stain PAS positive.4-7,9
Reis-Bucklers dystrophy
AKA: Granular corneal dystrophy type III, Corneal dystrophy of Bowman’s type I1-3
Inheritance: Autosomal dominant, TGFB-1, locus 5q311-4,8
Exam findings: Slit lamp exam may reveal a smooth corneal surface with irregular, gray-white, geographic-like opacities in Bowman’s layer and anterior stroma.1,4,7,9
Demographics: Patients may develop painful corneal erosions, opacification, and progressive visual decline within the first decade of life.1,4,7,9,10
Histology: Histology shows anterior stromal and subepithelial hyaline-like deposits which can disrupt and replace Bowman’s layer.4,7,9 These deposits stain red with Masson trichrome.4,7,9
Thiel-Benke dystrophy
Inheritance: Autosomal dominant, considered a variant of Reis-Bucklers1-4
Exam findings: Slit lamp exam findings are similar to Reis-Bucklers; patients here may have decreased corneal sensation as well. There may be a honeycomb opacity in the subepithelial region that develops in the second decade.1-6
Demographics This dystrophy typically presents in early childhood and may present with recurrent erosions and decreased vision.4-6,9,10
Histology: Histology shows anterior stromal and subepithelial hyaline-like deposits which can disrupt and replace Bowman’s layer.4,6,9 These deposits stain red with Masson trichrome.4,6,9 Electron microscopy can show presence of ‘curly fibers’ beneath the basal epithelium.4,6,9
STROMAL CORNEAL DYSTROPHIES
Stromal corneal dystrophies affect the middle and thickest layer of the cornea—the stroma.
Lattice dystrophy
Type 1
AKA: Biber-Haab-Dimmer corneal dystrophy, TGFB1 type Lattice dystrophy, classic lattice dystrophy1-3,8
Inheritance: Autosomal dominant, TGF-B1 gene on 5q31 locus1-4,8
Exam findings: Slit lamp exam may show glass-like filamentous deposits that may progress or change in character over time from anterior refractile stromal lesions to more nodular threadlike and thicker lesions in the deep stroma.4,6,7,9 The limbus is generally spared and clear spaces between lesions may progress to take on a ground-glass appearance.4,6,7,9 Irregular astigmatism and recurrent erosions may be present, as well as decreased vision.4,6,7,9
Demographics: Signs of lattice dystrophy type 1 usually appear in early childhood but become more prominent in the 20s and 30s.1-4,8
Histology: +Amyloid staining in anterior stroma6,9
Note: Mild lattice dystrophy may respond well to contact lenses—scleral lenses here may be especially helpful.11 Prompt recognition and treatment of erosions is key to prevent infection.11 PTK laser should be avoided as the laser energy is hypothesized to activate TGFB-1 and increase the number of lesions deposited.11 Penetrating keratoplasty is the definitive treatment here; patients should be warned that the dystrophy can recur in the graft.11
Type 2
AKA: Finnish Familial Amyloidosis, Meretoja syndrome, Amyloidosis V, Familial amyloidotic polyneuropathy IV1-3,8
Inheritance: Autosomal dominant, Gelsolin gene, locus 9q341-4,8
Exam findings: Slit lamp exam may show glass-like filamentous deposits that may progress from the limbus inward and are less dense than those present in type 1 lattice dystrophy.4,6,7,9 Patients may experience decreased corneal sensation, lagophthalmos, glaucoma, and dermatochalasis due to amyloid deposition.4,6,7,9 Systemic findings may also be present, such as dry, itchy skin, laxity of the facial skin, cardiac conduction abnormalities, orthostatic hypotension, and facial paresis (also due to systemic amyloidosis).4,6,7,9
Demographics: Vision typically is unaffected until middle age.1-4,8
Histology: Anterior stromal amyloid deposits and intra-lamellar amyloid deposits most prominent at the limbus.6,9 Mutated gelsolin deposits may be found in the conjunctiva, sclera, extraocular arterial walls, peripheral nerves, and kidneys.6,9
Granular dystrophy
Type 1
AKA: corneal dystrophy Groenouw type I1-3,8
Inheritance: Autosomal dominant, TGFB-1 gene, 5q31 locus1-4,8
Exam findings: Slit lamp exam here may show discrete, ‘breadcrumb’-like opacities in the anterior stroma.4,6,7,9 In early disease, these granules are separated by the clear cornea and tend to become more numerous over time and extend deep into the posterior stroma.4,6,7,9 The lesions here typically do not extend to the limbus. 4,6,7,9 Recurrent erosions may occur as well.4,6,7,9
Demographics: Visual symptoms such as glare and photophobia may occur early in life, but a decline in vision is usually not present until about 40 years old.1-4
Histology: Hyaline deposits are seen in the stromal tissue that stain red with Masson Trichrome4,6,9
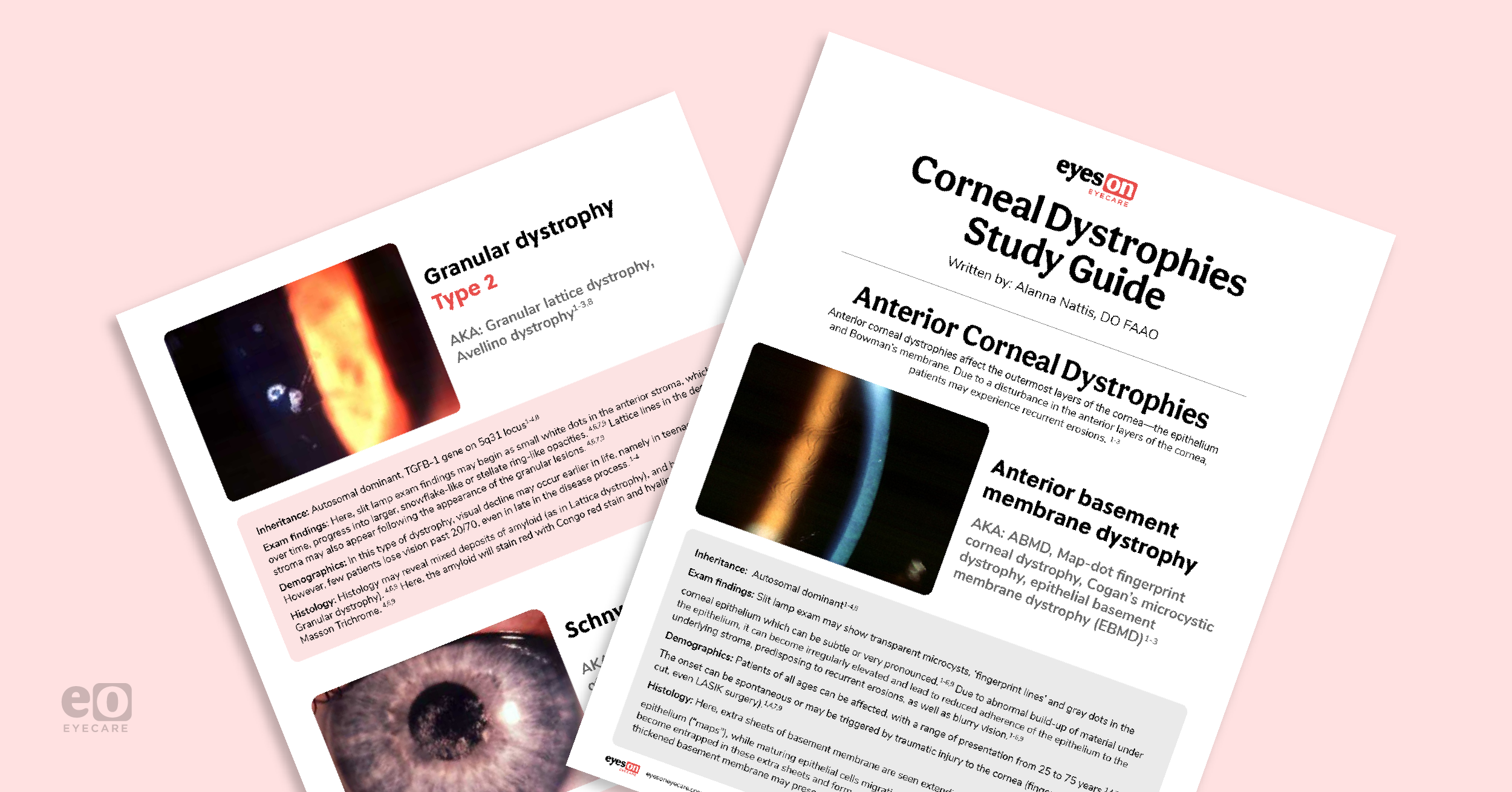
Type 2
AKA: Granular lattice dystrophy, Avellino dystrophy1-3,8
Inheritance: Autosomal dominant, TGFB-1 gene on 5q31 locus1-4,8
Exam findings: Here, slit lamp exam findings may begin as small white dots in the anterior stroma, which, over time, progress into larger, snowflake-like, or stellate ring-like opacities.4,6,7,9 Lattice lines in the deeper stroma may also appear following the appearance of the granular lesions.4,6,7,9
Demographics: In this type of dystrophy, visual decline may occur earlier in life, namely in teenage years.1-4 However, few patients lose vision past 20/70, even late in the disease process.1-4
Histology: Histology may reveal mixed deposits of amyloid (as in Lattice dystrophy), and hyaline (as in Granular dystrophy).4,6,9 Here, the amyloid will stain red with Congo red stain and hyaline strains red with Masson Trichrome.4,6,9
Macular dystrophy
AKA: Groenouw corneal dystrophy type II, Fehr spotted dystrophy1-4,8
Inheritance: Autosomal recessive, Carbohydrate sulfotransferase 6 gene ( CHST) on 16q221-4,8
Exam findings: Slit lamp exam findings here show stromal opacities with indistinct borders with intervening haze that can extend from limbus-to-limbus.4,6,7,9 Some cases can extend to Descemet’s membrane.4,6,7,9
Demographics: Severe vision impairment may occur in childhood.4,6,7,9,10 Recurrent erosions may also be present; there may also be loss of corneal sensation.4,6,7,9,10
Histology: In macular dystrophy, there is an accumulation of glycosaminoglycans (GAGs) in the stroma, which stain with colloidal iron or Alcian blue.6,9 There are 3 variants of macular dystrophy based on the immunoreactivity of the deposits to antigenic keratan sulfate:
- Type 1a: no reactivity in the cornea or serum4,6,9
- Type 1b: intracellular reactivity in the corneal stroma4,6,9
- Type 2: reactivity intracellular and extracellular in the cornea with low-normal serum reactivity4,6,9
Schnyder dystrophy
AKA: hereditary crystalline dystrophy of Schnyder, Schnyder corneal crystalline dystrophy, Crystalline stromal dystrophy, central stromal crystalline corneal dystrophy1-4,8
Inheritance: Autosomal dominant, UbiA prenyltransferase domain containing 1 gene (UBIAD1) on locus 1p261-4,8
Exam findings: Slit lamp exam here shows central corneal haze with/without crystal deposits (~50% cases).4,6,7,9
Demographics: Diagnosis is typically in the second or third decades of life, with increasing haze causing progressive visual loss in the mid-50s.4,6,7,9
Histology: Phospholipid and cholesterol deposits are present in the stroma, Bowman’s layer, and basal epithelium—this is best seen with special stains (Sudan black, Oil Red O).4,6,9
Congenital stromal corneal dystrophy (CSCD)
AKA: Congenital hereditary stromal dystrophy, congenital stromal dystrophy of the cornea1-4,8
Inheritance: Autosomal dominant, Decorin gene on locus 12q21.331-4,8
Exam findings: Here, slit lamp exam may show snowflake, white opacities throughout the entire cornea without inflammation.4,6,7,9
Demographics: There is moderate to severe loss of vision from birth due to corneal opacification3,4,6,7,9,10
Histology: Histologic exam here reveals abnormal stromal lamellae that may be separated by amorphous deposits.4,6,9 Electron microscopy shows collagen fibrils that are half of normal thickness.4,6,9
Fleck corneal dystrophy
AKA: Francois-Neetens speckled corneal dystrophy1-4,8
Inheritance: Autosomal dominant, Phosphatidylinositol-3-phosphate/phosphatidylinositol 5-Kinase type III gene (PIP5K3) on 2q351-4,8
Exam findings: Slit lamp exam reveals small, scattered, discrete gray-white dandruff-like opacities in an otherwise clear stroma4,6,7,9
Demographics: Usually patients are asymptomatic!4,6,7,9
Histology: Histology here shows swollen keratocytes with vacuoles containing glycosaminoglycans and lipid4,6,9
POSTERIOR CORNEAL DYSTROPHIES
Posterior corneal dystrophies affect the innermost parts of the cornea—Descemet’s membrane and the endothelium.
Posterior Polymorphous corneal dystrophy
AKA: PPMD, PPCD, Schlichting dystrophy1-4,8
Inheritance: Autosomal dominant, mapped to different loci on chromosomes 1,8, 10, and 201-4,8
Exam Findings: Here, slit lamp exam may show bilateral, (although occasionally asymmetric) diffuse corneal opacification with corneal edema.4,6,9,12 There may be endothelial vesicular changes, band lesions, central and peripheral corneal grayish opacities.4,6,9,12
Demographics: Most cases of PPMD are asymptomatic and therefore do not require treatment; severe cases involving corneal clouding and edema may require corneal transplantation.4,6,9,12
Histology: Due to abnormal developmental differentiation, the endothelial layer transforms into cells similar to stratified squamous epithelium, causing an abnormal basement membrane and thickening of Descemet’s membrane.4,6,9 These epithelium-like endothelial cells are usually pleomorphic, have multiple surface microvilli, are multi-layered, and stain positive for cytokeratin.4,6,9 The abnormal epithelialized cells migrate randomly, secrete defective basement membrane cells, and can cause peripheral synechiae. This, therefore, leads to ineffective fluid drainage from the corneal stroma, resulting in corneal edema and glaucoma.4,6,9 In addition, the thickened Descemet’s membrane and possible resulting stromal edema may lead to blurred vision and corneal clouding.4,6,9,12
Fuchs endothelial corneal dystrophy
AKA: N/A
Inheritance: Autosomal dominant, may be sporadic1-4,8
Exam Findings: Slit lamp exam may show loss of endothelial cells and small excrescences of Descemet’s membrane (“guttata”), with or without pigment deposition on the endothelium.3,4,6,9 In progressive cases, fluid from the anterior chamber will collect in the corneal stroma, leading to increased corneal thickness and decreased vision.3,4,6,9 Without treatment, the corneal edema can progress to collect in the epithelial layer, causing small blisters (“bullae”) to develop, which can be quite painful.3,4,6,9 Chronic corneal edema can also produce corneal fibrosis and scarring, leading to further opacification.3,4,6,9
Demographics: This condition usually presents in the early 30s-40s; it may present earlier in women.3,4,6,9
Histology: Histology will often reveal an edematous cornea due to paucity of endothelial cells and thickening of Descemet’s membrane.3,4,6,9 There may be separation of the epithelium from Bowman’s layer due to fluid accumulation.3,4,6,9 Guttae are usually present, to a variable degree (depending on the severity of the disease).3,4,6,9


