



What are choroidal nevi?
Choroidal nevi are benign melanocyte tumors of the uvea and are the most common benign intraocular tumor.1 Though relatively common, they can vary in size, location, and appearance. While nevi in many other body parts are readily visible, those within the eye may only be noted with a dilated ophthalmic exam.
Additionally, choroidal nevi are challenging to access. The necessity for specialized examination combined with challenging tissue access makes proper differentiation of choroidal nevi from other lesions complex.

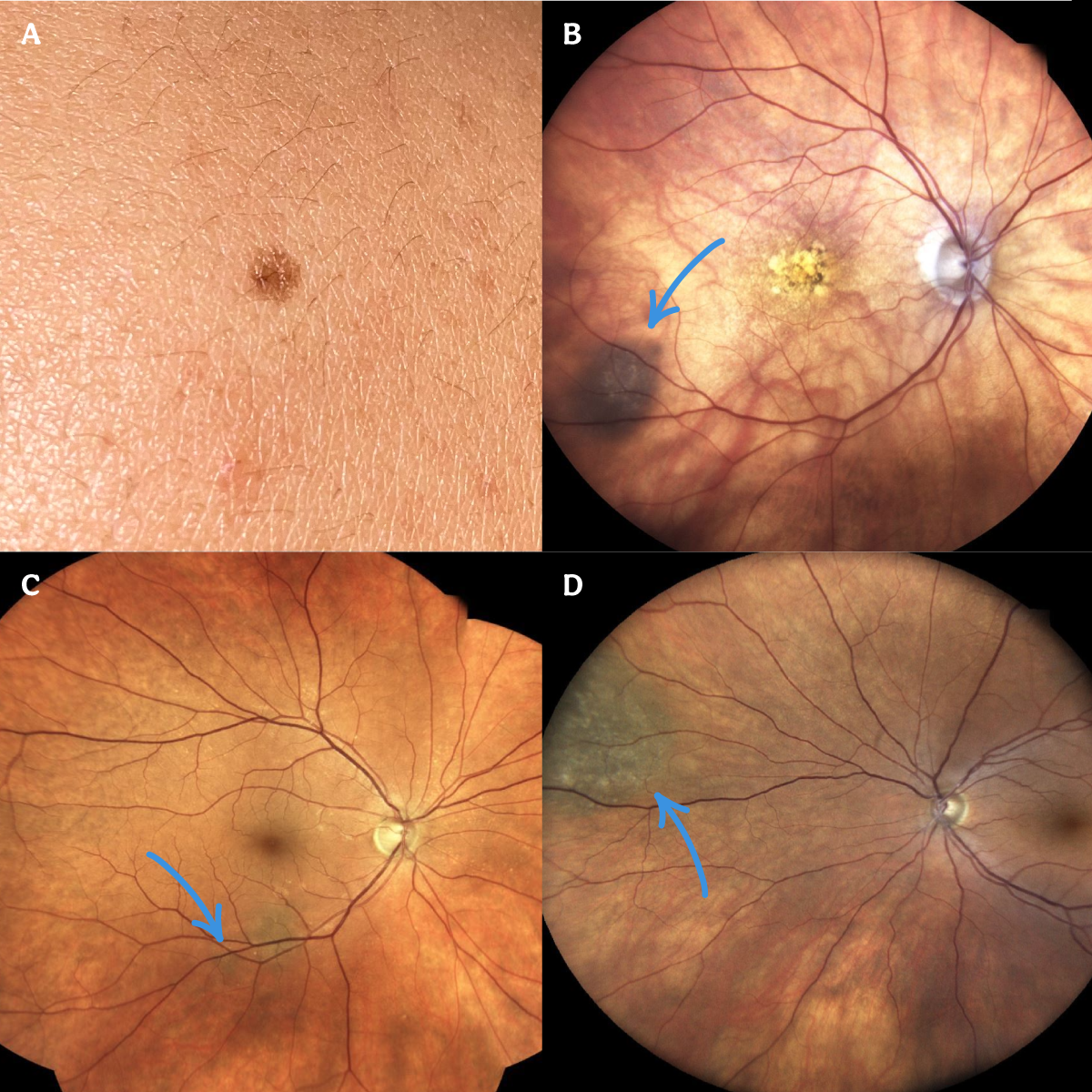
Figure 1: skin nevus (A) choroidal nevi (B,C,D).
Who gets choroidal nevi?
Choroidal nevi are often benign and asymptomatic, and it is not unusual for them to go unnoticed until spotted on an unrelated eye exam. While they are the most common benign intraocular tumor, they are still relatively rare, with a prevalence of only 2.1%.2 Some may be more likely to develop nevi, such as individuals who have fairer complexions. Regarding age, studies have had variable outcomes as to whether any association exists between age and the prevalence of nevi. There is no significant difference between genders.
Clinical presentation
How do these patients present?
Choroidal nevi are typically noted incidentally on routine ophthalmic examination. Often these patients are completely unaware they have a lesion inside their eye. The majority are asymptomatic, but less commonly choroidal nevi can be associated with visual complaints. These visual symptoms may include visual field deficits or decreased visual acuity.
Exam
Fundus examination
Ophthalmic examination often reveals a pigmented lesion with varying associated features. These lesions are usually small but can vary in size from under a disc diameter to greater than five disc diameters. They are often circular or oval shape and flat or minimally elevated (<2mm thick). Pigmentation can vary, and less commonly, lesions may be amelanotic.
Additional clinical significance findings include the absence of drusen, subretinal fluid, orange pigment, and choroidal neovascularization (CNV). It’s crucial to assess every nevus for these features as they can be associated with an increased risk of malignancy.
Natural history
Most nevi appear in the preteen or teenage years and remain benign over time. However, 31% of these lesions may continue to grow in size.3 Of clinical significance is differentiating which features increase concern for malignant transformation.
Benign or malignant?
Most nevi are benign however, malignant transformation is possible, and nevi must be carefully assessed for any concerning features. It is estimated that 1 in 8845 nevi will undergo malignant transformation each year.4 Extensive discussion and research have gone into identifying these characteristics. Landmark studies by Shields et al. identified risk factors predictive of growth of choroidal melanocytic tumors.5-6
These studies identified the following critical features in the evaluation of the malignant potential of a choroidal nevus: apical thickness over 2.5 mm, presence of subretinal fluid or serous retinal detachment, positive symptoms (e.g., a decline in visual acuity, photopsias), presence of orange pigment (also known as lipofuscin which is intracellular macrophage drusen), tumor proximity within 3 mm of the optic disc, ultrasound hollowness, absent peripheral hypopigmented halo, and absent drusen (Table 1).5,6,7
A mnemonic commonly used to abbreviate these risk factors is “To Find Small Ocular Melanoma Using Helpful Hints Daily” (TFSOMUHHD).

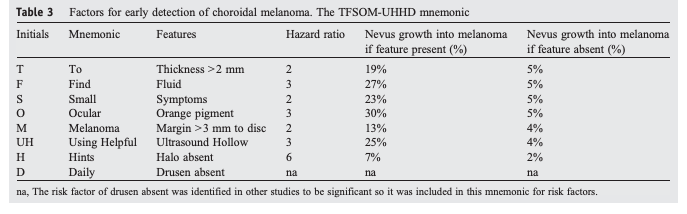
Table 1: Adapted from Shields et al, "Melanoma of the eye: Revealing hidden secrets, one at a time," illustrates the factors for early detection of choroidal melanoma.
Diagnosis & workup
Early identification of a malignant mass can mean the difference between life and death. Malignant lesions may easily masquerade as benign choroidal nevi, and appropriate diagnosis can be challenging. The most crucial tool in properly assessing these lesions is a comprehensive clinical exam, but ancillary tests still provide critical information. These tests include ultrasonography, fluorescein angiography, indocyanine green angiography, enhanced depth imaging optical coherence tomography (OCT), autofluorescence, and fine needle aspiration biopsy.
Fundus photography
Fundus photography is a fast, non-invasive, and effective tool for documenting and observing choroidal nevi. Having prior reference photographs is extremely helpful during serial examinations. Pictures from previous visits may better document features such as size, shape, and lesion characteristics. Clinical examination is still critical as inconsistencies with image color, artifact, and other image capture-related issues can make interpretation of photos alone difficult at times.
Ultrasonography
A-scan and B-scan ultrasonography provide important clinical information when evaluating a choroidal mass and differentiating malignant lesions. In contrast to choroidal nevi, A-Scan ultrasound of a choroidal melanoma will characteristically demonstrate a hypoechoic signal with low-to-medium internal reflectivity. B-scan ultrasonography is helpful to assess and monitor tumor size and can be used to search for any extra-ocular extension.
Choroidal nevi can also be carefully observed with serial measurements on A-scan and B-scan. Specific characteristics such as the presence of a mushroom configuration are highly-concerning for choroidal melanoma. Choroidal hemangiomas, osteomas, and metastases are examples of other retinal lesions in which ultrasonography can also be useful.
Enhanced depth imaging optical coherence tomography (EDI-OCT)
EDI-OCT is a non-invasive, readily available imaging modality that can quickly acquire retinal images. In contrast to traditional OCT, EDI-OCT captures a longer image that allows for better assessment of the choroid. Certain OCT characteristics should increase concern for possible malignancy; for example: presence of subretinal fluid, shaggy (i.e., elongated) photoreceptors, subretinal lipofuscin deposits, increased thickness, and outer retina disruption.8 The presence of any of these features increases the risk of melanoma.
Fundus autofluorescence (FAF)
Fundus autofluorescence photography generates images by way of the natural fluorescence of intraocular tissues. Lipofuscin deposition occurs over time in the retina and creates fluorescent signals. These signals can be captured and analyzed. Studies researching the significance of fundus autofluorescence imaging in the evaluation of choroidal nevi have revealed clinically relevant characteristics. Choroidal nevi can have variable FAF.
In contrast, subretinal fluid may be associated with hyperautofluorescence most apparent at the margins of the fluid. Subretinal fluid is a risk factor for choroidal melanoma. Additionally, lipofuscin, visible as orange pigment is hyperautofluorescent and is a risk factor for melanoma.9
Fluorescein angiography (FA)
Fluorescein angiography (FA) is less relevant for choroidal nevi and choroidal melanomas because it is a more invasive and time-consuming imaging modality. FA of some melanomas can demonstrate a “double circulation” with intrinsic tumor vasculature circulation apparent on imaging; the latter is not present in choroidal nevi. Additionally, if orange pigmentation - a risk factor for melanoma - is present, the fluorescence in those areas will typically be hypofluorescent.
Indocyanine green angiography (ICG)
Indocyanine green angiography provides some advantages over FA imaging in that it allows for better evaluation of choroidal vasculature and circulation. Malignant melanoma will classically demonstrate a “double circulation”. This is most apparent in areas of relative hypopigmenation or amelanotic lesions. Pigmentation lesions can block ICG fluorescence due to the overlying melanin. ICG is also helpful in differentiating other retinal lesions such as choroidal hemangioma and metastasis.

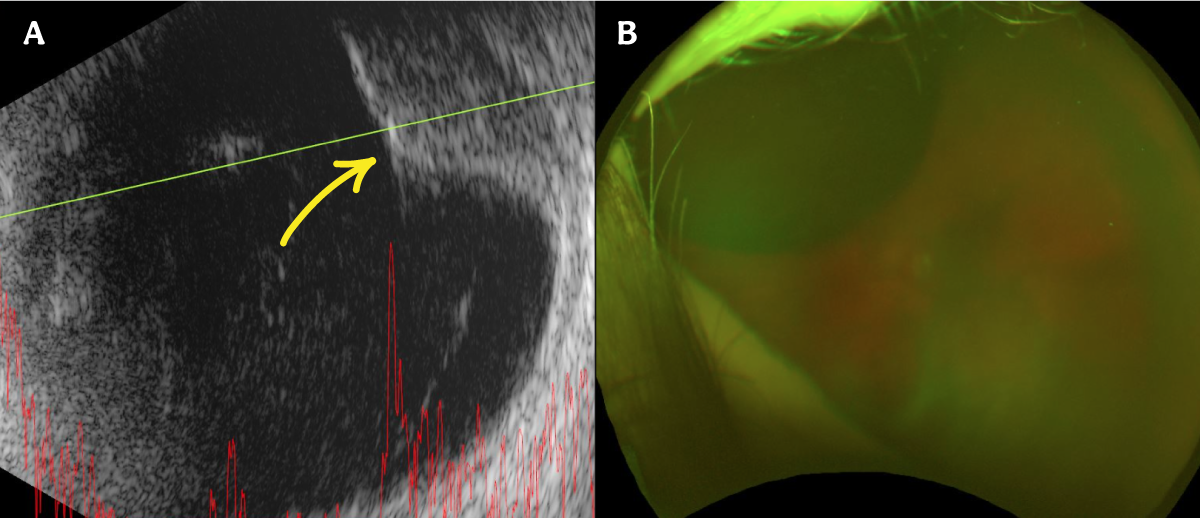
Figure 2: Malignant melanoma and associated B scan.
Fine needle aspiration biopsy (FNAB)
A thorough clinical exam in combination with modern-day ancillary imaging will provide an accurate diagnosis for most intraocular tumors without the need for procedure or surgery. However, some cases do require tissue diagnosis. FNAB is a safe and effective way to obtain a surgical specimen for further analysis. Histopathology, cytology, and cytogenetic studies can provide a diagnosis. There are risks with FNAB, such as hemorrhage, retinal detachment, endophthalmitis, and needle tract seeding.
Management
Asymptomatic choroidal nevi without any concerning risk factors are monitored with serial examinations and appropriate imaging every 4 to 12 months. This interval may be shortened if there is increased concern for malignant transformation.
The management of malignant melanoma is much more complex, and there is considerable debate about how best to approach these tumors. Depending on the clinical presentation, possibilities include observation, transpupillary thermoplasty, plaque radiotherapy, charged particle irradiation, external resection (exoresection), internal resection (endoresection), enucleation, orbital exenteration, systemic chemotherapy, and systemic immunotherapy.
Prognosis
The prognosis for choroidal nevi is excellent. The majority of patients with these lesions will be completely asymptomatic and never develop any visual symptoms. Rarely, nevi can transform into neoplastic lesions with the ability to grow and metastasize. This can result in loss of vision, loss of the eye, or loss of life. Careful examination, monitoring, and workup can help identify these more dangerous lesions.
Differential diagnosis
A careful ophthalmic examination in combination with ancillary testing is crucial for the appropriate diagnosis of choroidal nevi. However, it is essential to keep other choroidal lesions in mind when assessing a patient for a possible nevus. The differential can be quite broad, but there are some more common possibilities to keep in mind.
Melanoma
The most important differential diagnosis to keep in mind when evaluating a possible choroidal nevus is melanoma. While some of these are striking and relatively straightforward to identify, many can be quite challenging. The previously mentioned risk factors (thickness over 2.5 mm, subretinal fluid, symptoms, orange pigment, tumor proximity within 3 mm of the optic disc, ultrasound hollowness, halo absent, and drusen absent) are helpful when attempting to differentiate possible choroidal melanomas.5,6,7 Growth over a short period of time can also increase concern for melanoma.
Workup involves a thorough ocular exam with the ancillary testing previously described. Systemic workup may include genetic testing, liver function and imaging, magnetic resonance imaging, computerized tomography scans, and positive emission tomography. Treatment is variable and broad depending on how high the level of concern is for melanoma. It may be closely observed if a lesion is small in size, appears most likely a nevus, and is without significant risk factors.
Treatments can then escalate from photocoagulation and transpupillary thermoplasty for smaller melanomas to plaque radiotherapy, proton beam therapy, local resection, enucleation, and orbital exenteration. If there is a concern for metastasis, additional systemic treatment may be necessary.
Congenital hypertrophy of the retinal pigmented epithelium (CHRPE)
CHRPE are benign congenital lesions that are generally asymptomatic. CHRPE lesions can come in three different forms: solitary, grouped, or dispersed. Like choroidal nevi, they are often picked up incidentally on routine eye examination. On examination these appear as flat, circular, hyperpigmented lesions with well-demarcated smooth edges and possible areas of hypopigmentation (lacunae).
The heavily pigmented and well-circumscribed appearance with “punched out” looking lacunae can sometimes help differentiate CHRPE from other lesions. The pigmentation can be more mild and brown or significant and black.

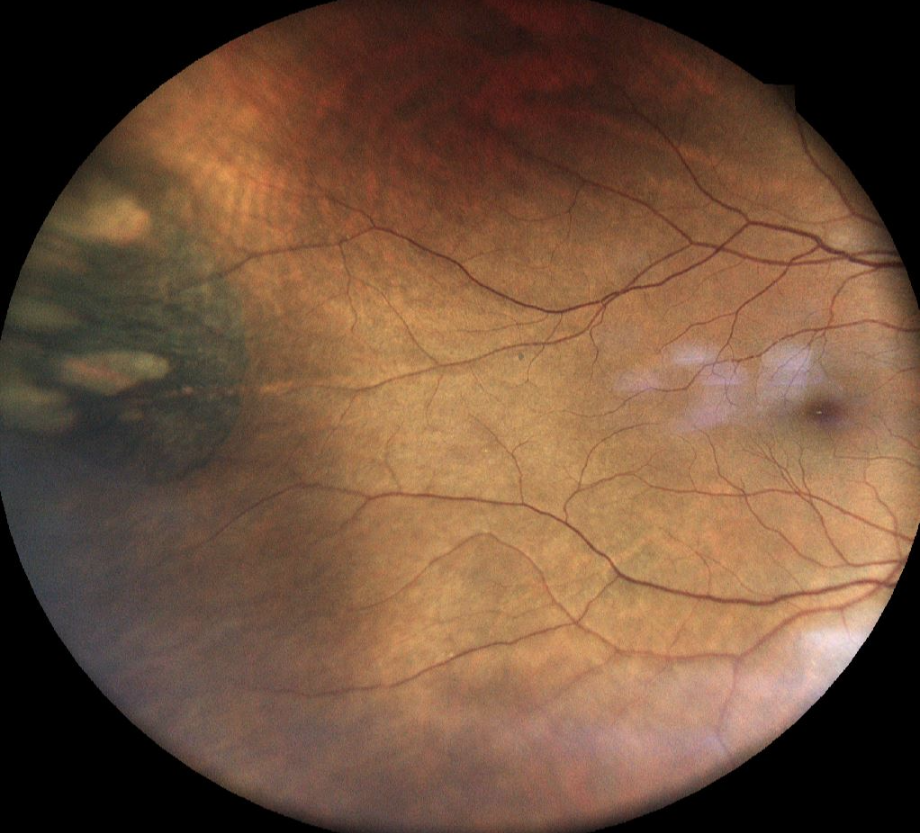
Figure 3: Congenital Hypertrophy of the Retinal Pigmented Epithelium (CHRPE).
The size of these lesions is variable, from less than a disc diameter to quite large. Rarely they can become symptomatic by extension into the fovea or undergo malignant transformation to adenocarcinoma. The grouped form of CHRPE is known as “bear tracks”. Moreover, multiple discrete CHRPE can be associated with familial adenomatous polyposis (FAP), an autosomal dominant disease associated with colon polyps and an increased risk of gastrointestinal cancer.
FAF will typically show hypoautofluorescence except in areas of lacunae, and FA imaging will be hypofluorescent with blockage and no leakage. Management generally is observation unless there is a concern for malignant transformation.
Choroidal hemangioma
Choroidal hemangiomas are benign vascular lesions that can be associated with systemic abnormalities. There are two forms: solitary and diffuse masses. Solitary hemangiomas are typically idiopathic, while the diffuse form can be related to Sturge Weber syndrome. Choroidal hemangiomas are generally posterior in location and appear as well-circumscribed orange-red masses and can be associated with overlying subretinal fluid, retinal hemorrhages, macular edema, serous retinal detachment, exudates, choroidal neovascularization, and epiretinal membrane formation. Depending on their location and associated features they can be associated with vision loss.
Ultrasonography reveals a hyperreflective lesion on A- and B-scans. FA shows early hyperfluorescence while FAF findings show variable hypo or hyperautofluorescence. ICG testing shows a characteristic rapid filling followed by a washout phenomenon. Most lesions can be observed; however, symptomatic lesions may be treated with vascular endothelial growth factor inhibitors, laser retinopexy, or radiotherapy, depending on their severity.

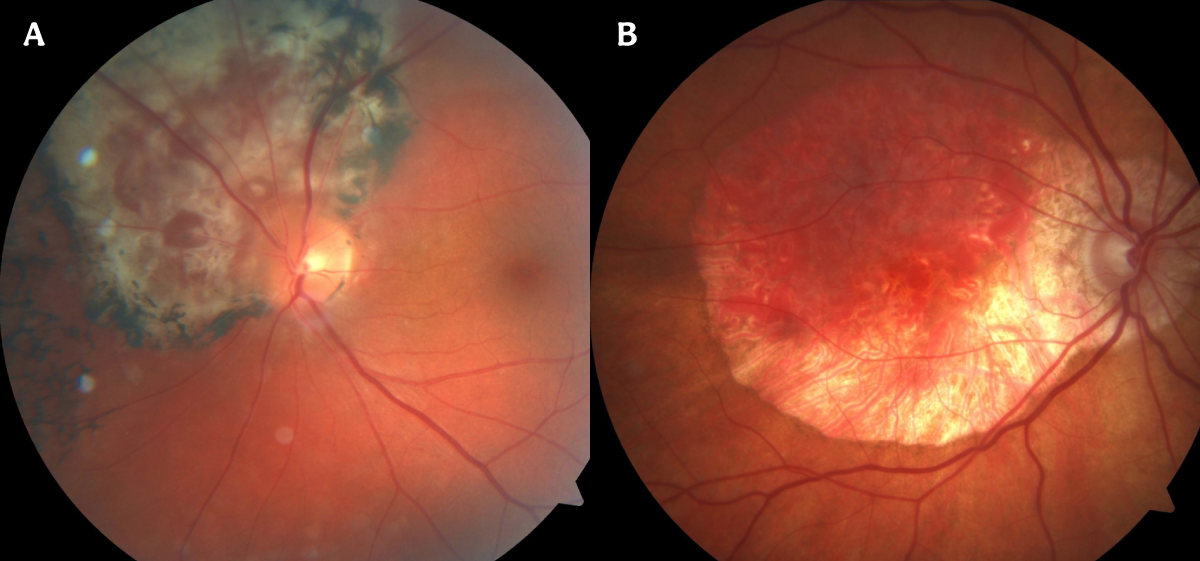
Figure 4: Two examples of choroidal hemangioma.
Choroidal osteoma
Choroidal osteomas are benign calcified lesions that have undergone ossification and are composed of bone. They are rare and typically appear in young, healthy individuals. Most cases are unilateral and less commonly bilateral. Lesions are often in the posterior retina and near the optic disc and macula. They have an orange-yellow appearance. Though typically asymptomatic, they can be associated with choroidal neovascularization and subretinal fluid. In these cases, patients are more likely to have visual disturbances. Osteomas usually have a round, well-defined shape, but there can be some variation in their appearance.
Ultrasonography is helpful in the diagnosis and may show hyperechoic signals with shadowing. These calcifications can sometimes be appreciated on computed tomography and magnetic resonance imaging scans. Management is typically observation; however, if a patient has a complicating choroidal neovascular membrane, therapy may be indicated.
Metastasis
While choroidal nevi are the most common benign intraocular tumor, choroidal metastases are the most common intraocular tumor overall in adults.10,11 Patients can be asymptomatic or develop vision loss; 20-40% of cases can be bilateral, and 20% of cases reveal multiple lesions in the same eye.12 Choroidal metastatic lesions are typically creamy-yellow and associated with a serous or exudative retinal detachment. A- and B-scans will often have high reflectivity. Metastases can originate from several primary cancers, but in men, lung cancer in men and breast cancer in women are the most common primary sites.
Conclusions
Choroidal nevi are not uncommon in the population and are generally asymptomatic and benign. However, they can mimic several other lesions that are more dangerous and may require close follow-up and intervention. Appropriate management involves monitoring and documentation of nevi size and features in conjunction with ancillary testing and imaging. It is vital to keep a low threshold for more dangerous differential diagnoses as they can be vision, eye, or life-threatening.
References
- Shields JA, Shields CL. Choroidal Nevus. In: Intraocular Tumors. An Atlas and Textbook. 3rd Edition. Philadelphia, PA: Lippincott Williams and Wilkins, Wolters Kluwers; 2015. Pp. 69–80.
- Greenstein MB, Myers CE, Meuer SM, Klein BEK, Cotch MF, Wong TY, Klein R. Prevalence and characteristics of choroidal nevi: the multi-ethnic study of atherosclerosis. Ophthalmology. 2011;118(12):2468-2473. doi:10.1016/j.ophtha.2011.05.007
- Shields CL, Furuta M, Mashayekhi A, Berman EL, Zahler JD, Hoberman DM, Dinh DH, Shields JA. Clinical spectrum of choroidal nevi based on age at presentation in 3422 consecutive eyes. Ophthalmology. 2008;115(3):546-552.e2. doi:10.1016/j.ophtha.2007.07.009
- Singh AD, Kalyani P, Topham A. Estimating the risk of malignant transformation of a choroidal nevus. Ophthalmology. 2005;112(10):1784-1789. doi:10.1016/j.ophtha.2005.06.011
- Shields CL, Cater J, Shields JA, Singh AD, Santos MC, Carvalho C. Combination of clinical factors predictive of growth of small choroidal melanocytic tumors. Arch Ophthalmol. 2000;118(3):360-364. doi:10.1001/archopht.118.3.360
- Shields CL, Furuta M, Berman EL, Zahler JD, Hoberman DM, Dinh DH, Mashayekhi A, Shields JA. Choroidal Nevus Transformation Into Melanoma: Analysis of 2514 Consecutive Cases. Archives of Ophthalmology. 2009;127(8):981-987. doi:10.1001/archophthalmol.2009.151
- Shields CL, Kels JG, Shields JA. Melanoma of the eye: Revealing hidden secrets, one at a time. Clinics in Dermatology. 2015;33(2):183-196. doi:10.1016/j.clindermatol.2014.10.010
- Shields CL, Kaliki S, Rojanaporn D, Ferenczy SR, Shields JA. Enhanced Depth Imaging Optical Coherence Tomography of Small Choroidal Melanoma: Comparison With Choroidal Nevus. Archives of Ophthalmology. 2012;130(7):850-856. doi:10.1001/archophthalmol.2012.1135
- Shields CL, Pirondini C, Bianciotto C, et al. Autofluorescence of choroidal nevus in 64 cases. Retina. 2008;8:1035-1043. - Google Search. Accessed August 14, 2021. https://www.google.com/search?q=Shields+CL%2C+Pirondini+C%2C+Bianciotto+C%2C+et+al.+Autofluorescence+of+choroidal+nevus+in+64+cases.+Retina.+2008%3B8%3A1035-1043.&oq=Shields+CL%2C+Pirondini+C%2C+Bianciotto+C%2C+et+al.+Autofluorescence+of+choroidal+nevus+in+64+cases.+Retina.+2008%3B8%3A1035-1043.&aqs=chrome..69i57.1071j0j9&sourceid=chrome&ie=UTF-8
- Ferry AP, Font RL. Carcinoma metastatic to the eye and orbit. I. A clinicopathologic study of 227 cases. Arch Ophthalmol. 1974;92(4):276-286. doi:10.1001/archopht.1974.01010010286003
- Bloch RS, Gartner S. The incidence of ocular metastatic carcinoma. Arch Ophthalmol. 1971;85(6):673-675. doi:10.1001/archopht.1971.00990050675005
- Shields JA. Diagnosis and Management of Intraocular Tumors. C.V. Mosby; 1983.


